To identify anatomic sex differences in the osseous and cartilage structures of the knee.
We performed a comprehensive review of imaging investigations of knee morphology comparing male and female subjects using PUBMED, with search terms for CT/MRI, knee anatomy, and gender. Inclusion criteria were primary imaging investigations of knee osseous/cartilage anatomy (minimum 15 subjects); exclusion criteria were studies of post-operative patients, those with comorbid orthopedic conditions, and review articles. Sex differences in osseous/cartilage anatomy were extracted and aggregated.
Of 1550 citations reviewed, 84 studies met inclusion criteria and fell into 5 categories: Bony axes of the knee (n = 21), morphology of the distal femur (n = 38), proximal tibia (n = 15) and patella (n = 8), and articular cartilage (n = 16). Knee axes studies suggested trochlear groove-tibial tuberosity distance and posterior tibial slope may be greater in females. Distal femur studies showed larger metrics in males, and narrower metrics in females with smaller intercondylar notch volumes. Regarding tibial morphology, females had smaller tibias (normalizing for height), with narrower tibial plateaus and deeper medial tibial plateaus. Female patellas were smaller and different enough in morphology to be accurate in predicting sex in forensic studies. Cartilage studies mostly suggested that articular cartilage thickness and volume were greater in males.
Sex differences in anatomic structures of the knee have been reported. Given the increasing emphasis on individualized medicine, the emergence of sex-based diagnosis and treatment protocols, radiologists should be aware of anatomic sex differences.
Women’s sports medicine is a growing field in the world, as research has shown that women are more susceptible to certain sports-related injuries and require tailored treatment and prevention programs. An understanding of anatomic sex differences is important in the recognition of sex-related injury patterns. In the knee, most researches have focused on the Anterior Cruciate Ligament (ACL), with orthopedic surgery, physical therapy, and other clinical sports medicine fields producing the majority of the research regarding the functional and biomechanical aspects of knee stability and ligament differences. Women are known to have 2-8 times more frequent non-contact ACL injuries than men. While the etiology and implications for this sex difference remained unclear, functional, hormonal and anatomic factors may play a role, and sex differences in bone anatomic features have been studied, as they relate to the ACL [1]. For example, sex differences had been suggested in the posterior tibial slope of injured knees, a parameter which had been shown to play a role in knee stability in addition to ACL injury [2,3], and differences in notch dimensions and lim alignment may be a causal factor in the developing of tears of the ACL [1]. However, there has been no systematic comparison of knee anatomy as it related to gender differences.
Another area of research relating to bone and cartilage sex differences has been performed outside the acute sports medicine practice, with the goal of personalizing arthroplasty components. Sex-specific implants are now being used clinically, despite some disagreement on whether the differences are truly related to sex or simply the size of the femur and tibia [4]. Additionally, whether sex-specific components improve outcomes after surgery is a controversial topic on its own [5].
Hence, we sought to evaluate the current literature to identify areas of agreement, controversy, and knowledge gaps that may better inform both radiologists and sports medicine clinicians about sex differences in the anatomy of the knee. If radiologists can accurately identify patients at risk of injury, can detect risk factors for post-operative complications, or help aid the clinical and surgical team in operative planning or rehabilitation planning by noting sex differences, the field of radiology will be invaluable in customizing care for patients moving forward. Thus, the purpose of this study was to perform a comprehensive review of the English literature for original scientific researches on sex differences in osseous and cartilage anatomy of the knee.
To identify original articles for this review, a computerized MEDLINE database search was performed through the PubMed service of the National Library of Medicine for articles in the English language with the search criteria listed (Figure 1). The search included articles published between 2001 and December 2016. Limiting the search to articles in English was done for practical reasons, but very few articles were eliminated using this filter. A manual search and perusing of reference lists was also performed in MEDLINE following the comprehensive search, to identify any potential additional primary studies. The search was performed on March 24, 2016.
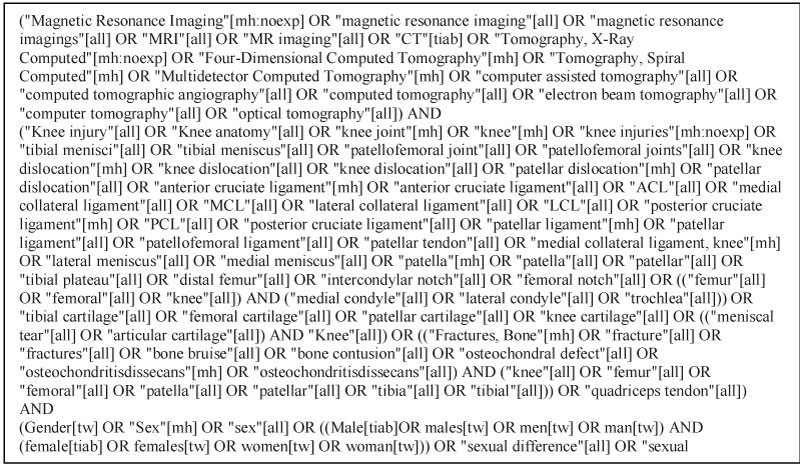 Figure 1: Pubmed search strategy is shown.
View Figure 1
Figure 1: Pubmed search strategy is shown.
View Figure 1
Inclusion criteria were primary investigations of cross-sectional imaging of knee anatomy by Computed Tomography (CT) or Magnetic Resonance Imaging (MRI) in males and females of all ages. We excluded studies with fewer than 15 subjects due to small sample size. Studies examining injury patterns, functional anatomy, anatomy of soft tissues (tendons, ligaments, muscles, menisci), and knee development were not included in this study. We also excluded studies focusing on modalities outside of CT/MR, such that studies examining differences based on radiography and nuclear medicine modalities were rejected. Studies reviewing joints other than the knee (e.g. the hip), studies in patients with comorbid conditions affecting the knee (example: Arthritis), studies in postsurgical patients and review articles were also excluded. The search also returned articles which were unrelated to the subject of interest (example: Treatment of tension pneumothorax) which were excluded as well.
Each citation was reviewed by one observer (LP) based on the inclusion and exclusion criteria, starting with title. If question of appropriateness of the study persisted, the abstract and finally the full text were reviewed prior to inclusion or exclusion of the study.
Each eligible article was examined by one observer (LP), for imaging features that compared males and females on cross-sectional imaging, and the features were then divided into bony axes, distal femur morphology, proximal tibia morphology, patella morphology, and articular cartilage. If a study examined sex differences in multiple categories and/or subcategories, all applicable categories were assigned to that study.
Each study was categorized as above, and anatomic features of males and females were extracted and tabulated. A descriptive analysis was performed. As the studies covered multiple categories of findings, with varied inclusion criteria, a meta-analysis could not be performed.
The literature search identified 1550 citations for consideration. A hand search yielded three additional articles satisfying inclusion criteria. Review of the article titles excluded 1104 citations, leaving 449 articles for further consideration. Finally, a full-text review excluded 365 studies, leaving 84 articles, as detailed in Figure 2. The range of sample sizes in the included investigations was as low as 17, to as large as 1062 subjects, as shown in Table 1.
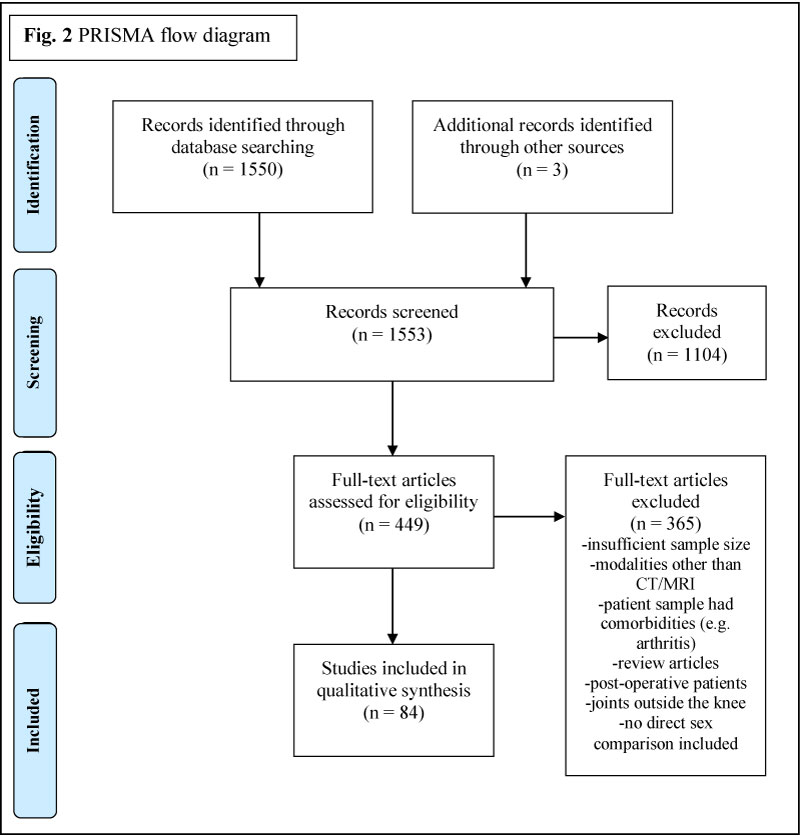 Figure 2: Diagram showing study inclusion and exclusion.
View Figure 2
Figure 2: Diagram showing study inclusion and exclusion.
View Figure 2
Table 1: Study characteristics and categories. View Table 1
The 84 included articles spanned 5 major categories shown in Table 1: Bony axes of the knee (21 papers), morphology of the distal femur (38 papers), morphology of the proximal tibia (15 papers), morphology of the patella (8 papers), and articular cartilage (16 papers). The axes category was divided into 7 subcategories (Table 2): Condylar angles, flexion, Insall-Salvati ratio (ratio of patellar length to patellar tendon length), Posterior Tibial Slope (PTS), tibial rotation, Tibial Tuberosity to Trochlear Groove (TT-TG) distance, and valgus. The distal femur category was divided into 9 subcategories (Table 3): Anteroposterior (AP) condylar length, mediolateral (ML) condylar width, condyle height, condyle ratios, notch, posterior offset, trochlea, red marrow, and surface area/volume. The proximal tibia category was divided into 8 subcategories (Table 4): Plateau depth, AP plateau diameter, ML plateau diameter, plateau ratio, tibial offset, master shape of the proximal tibia, posterior proximal tibia, and ACL insertion site in the proximal tibia. The patella category was divided into 7 subcategories (Table 5): Patella height, patella width, patella thickness, patella bone volume, patella surface area, patella width to thickness ratio, patella morphology sex model (3D-CT modeling for forensic sex analysis with a single patella). The articular cartilage category was divided into 7 subcategories (Table 6): T2 cartilage values, thickness, surface area, general volume, tibial volume, patellar volume, and femur volume.
Table 2: A summary of investigations of the bony axes of the knee. View Table 2
Table 3: A summary of investigations of the distal femur. View Table 3
Table 4: A summary of investigations of the proximal tibia. View Table 4
Table 5: A summary of investigations of the patella. View Table 5
Table 6: A summary of investigations of the articular cartilage. View Table 6
Bony axes of the knee: Although there were some common results, most of the metrics studied in articles investigating bony axes of the knee showed controversy with regards to sex differences, and some articles investigated unique metrics not evaluated in other articles. Studies evaluating the TT-TG showed either no sex difference (3/5 studies), or greater values in females, particularly with a history of patellar instability (2/5 studies showing 14.1-19.5 mm in females vs. 12.6-17.0 mm in males). The majority of studies examining PTS showed no sex difference in either the medial (7/10 studies) or lateral tibial plateau (8/10 studies), although the remaining studies showed a greater slope in females (2/10 studies for lateral tibial plateau; 3/10 studies for medial tibial plateau), with females having a mean medial PTS ranging from 4.9 - 6.3 degrees compared to 3.0 - 5.1 degrees in males [6-8], and a mean lateral PTS ranging from 6.3 - 7.0 degrees in females compared with 4.8 - 5.4 degrees in males [6,8]. Females had greater average Insall-Salvati ratios (1.0878 in females vs. 1.0032 in males) and valgus angles at the knee (mean of 5.3 degrees in females vs. 3.1 degrees in males), although these metrics were only described in one study each [9,10]. Males exhibited a greater degree of flexion at the knee, also only described in one study [11]. Femoral rotation was described in three studies, which showed no sex difference; however, one study showed greater tibial rotation in males [12].
Morphology of the distal femur: This group of studies had the largest volume of articles and metrics investigated. Examples of distal femur metrics studied are seen in Figure 3. In nearly all femoral size metrics (including metrics such as epicondylar width, AP diameter of each condyle, height of the condyles, surface area of the distal femur etc.), males had greater unadjusted values. For example, unadjusted measurements of the AP dimensions of the medial condyle ranged from 55-64 mm in females with significantly greater dimensions in males in most papers, ranging from 61-70 mm [13-18]. Unadjusted AP measurements of the lateral condyle were also greater in males, ranging from 58-66 mm in females compared with 65-72 mm in males [13-17]. However, when adjustments for height, weight, femoral length, leg length, etc., were performed, many of these sex differences decreased or disappeared, or disagreement existed within the investigations. For example, one study showed statistically greater mean AP medial femoral condyle measurements in females (77 mm compared to 74 mm) and greater mean AP lateral femoral condyle measurements in males (79 mm compared to 74 mm) when normalized to the transepicondylar width of the femur [19]. Condylar aspect ratios were also controversial, with some studies showing no sex difference, some showing greater aspect ratios in males, and some showing greater aspect ratios in females. Studies also looked specifically at the intercondylar notch and found that while males have greater unadjusted notch widths, when using the notch width index or adjusting for other factors, the sex difference often decreased or disappeared.
 Figure 3: (a) Example figures showing distal femur metrics. Transepicondylar width is an example of a mediolateral (ML) metric; (b) Posterior offset of the femur; (c) Trochlear depth (solid line) and lateral condyle height (solid arrow).
View Figure 3
Figure 3: (a) Example figures showing distal femur metrics. Transepicondylar width is an example of a mediolateral (ML) metric; (b) Posterior offset of the femur; (c) Trochlear depth (solid line) and lateral condyle height (solid arrow).
View Figure 3
Three studies looked at posterior femoral offset and two thirds of the studies found greater femoral offset in males. Two of the studies looked at posterior offset as a ratio to femoral size; however, one study calculated the ratio based on AP diameter of the distal femoral condyles, finding no sex difference, while the other study used the diameter of the femoral diaphysis, finding the medial condyle ratio to be greater in females, but not different in the lateral compartment [20,21].
The trochlea was evaluated in 10 different studies, which showed a general trend (with some exceptions) towards more metrics suggesting trochlear dysplasia in females (such as shallower sulcus/greater sulcus angle, or greater asymmetry). One final unique study evaluated anatomical sex differences in the femur, finding greater residual red marrow in females than males [22].
Morphology of the proximal tibia: The majority of studies showed greater proximal tibial metrics in males (such as plateau depth, and AP/ML diameter of the tibia), often persisting with adjustment for body height and weight. For example, unadjusted mediolateral tibial plateau widths were larger in males, measuring 77-81 mm in males compared to 69-70 mm in females [23,24]. Tibial plateau ratios were less conclusive, with 2/3 studies showing greater or no difference between sexes.
There were 5 studies evaluating unique sex differences of the proximal tibia: Two studies were performed by the same group at the same institution which evaluated a master shape of the proximal tibia produced through a contour detection algorithm, finding no sex differences [25,26]. One study looked at the anterolateral offset of the tibial shaft relative to the tibial plateau, which was greater in males [27]. Another study evaluated the morphology of the posterior aspect of the proximal tibia, finding no sex difference in either the arc angle or radius of the arc forming the posterior contour [28]. Finally, another study calculated the tibial insertion site of the ACL as a percentage of the AP tibial plateau dimension and found that there were no significant sex differences in this percentage [29].
Morphology of the patella: The majority of studies evaluating the patella showed greater metrics in males, which usually persisted after adjustment for height and weight. However, one paper evaluated the patella width to thickness ratio and found no sex difference [30]. Interestingly, two studies from the same institution looked at 3D forensic modeling using CT and found that the patellar morphology was able to be modeled with at least 93% accuracy when predicting sex of the donor [31,32].
Articular cartilage: We found articles that discussed T2 cartilage metrics (thickness, area, and volumes) as well as T2 signal characteristics. Not all studies adjusted findings for patient height and weight. Males had greater cartilage size metrics when no adjustments were made. When adjusting for height and weight, two studies found that females had less cartilage volume, thickness, and joint surface area, while two other studies found no sex discrepancy in cartilage metrics. For example, in two studies that showed statistically greater total knee cartilage volume in males (mean ranging from 23-27 cc) compared to females (mean 18 cc) [33,34], statistical significance was lost after adjusting for patient height/weight [34]. The other study showed greater cartilage volume in males, to a lesser degree after normalizing to weight (male to female volume difference decreasing from 9 cc to 5 cc) or height (difference decreasing from 9 cc to 7 cc) [33]. Of potential importance, one of the two studies which showed the sex difference also described a faster cartilage loss in females with aging relative to males, and this was not evaluated in other studies in our sample [35]. Finally, four studies looked at sex differences in T2 signal characteristics, and only one found statistically significant higher T2 values in females, only in the medial femur cartilage.
This was the first report comprehensively assessing the existing literature to identify differences in the osseous and cartilage structures of the knee between the sexes. While sex differences in the knee had been previously documented, they had largely focused on the ACL anatomy, injury rates and outcomes. The sex differences of bone and cartilage were less well understood, and this comprehensive review demonstrated that there were some well-established sex differences, some trends toward differences in anatomy, and that other sex differences still require further investigation.
As women’s sports medicine is still an emerging field, we uncovered investigations of anatomic sex differences that utilized varied and non-uniform anatomic metrics and study methods. In particular, many of the studies did not normalize the metrics to patient size (such as patient height, weight, femur length etc), or did not normalize the metrics to patient size in a standard way (such as to a particular bone diameter). In addition, in some studies, sex comparisons were secondary objectives rather than the primary endpoint of the investigation, perhaps resulting in a study design that less optimally assessed sex differences. Another factor that might explain some of the varied results observed was the potential for measurement error in many of the metrics utilized; whether measurements were made by hand or with an automated tool, inter-observer reliability statistics were not available in many investigations. Hence, this comprehensive review yielded a heterogeneous group of studies, upon which a meta-analysis could not be performed; rather, we aimed to accurately summarize current knowledge and gaps in information.
Overall, the literature indicated that unadjusted size metrics in the knee, including various femoral, tibial, patellar, and cartilage metrics, were larger in males than females. However, once adjustments were made for factors such as subject height, weight, and total femur length, some of the sex differences in anatomic metrics did not persist. This phenomenon was particularly true in many distal femur, proximal tibia, and articular cartilage metrics. Thus, adjusting for body size factors was critical to determining whether observed sex differences were innate, or whether they were due solely to the patient size.
The majority of studies showed no sex differences in measurements of the bony axes of the knee, although in studies where a difference was observed, females were shown to have larger metrics (including in the TT-TG, the Insall-Salvati, the PTS PTS, and the valgus angulation). Alterations in such metrics had been posed as potential risk factors for sports injuries in females. For example, sex differences in the PTS were thought to be a risk factor in developing ACL and meniscus tears, due to accompany altered biomechanics [36]. Given the known female predilection for ACL tears, such investigations of anatomic differences in the PTS may provide important insight into why this female predilection existed, and when designing a treatment plan, anatomic differences might play an important role in therapy and future prevention.
Another area of interest that was explored in this study was the trochlear morphology. Unfortunately, the studies found in our search were fewer in number and heterogeneous, resulting in limited conclusive power. Included studies that analyzed trochlear morphology suggested a trend towards a more shallow trochlea in females with lesser trochlear depth, greater sulcus angle, and greater asymmetry in the trochlea, all important anatomic features to further exploring the diagnosis of trochlear dysplasia and its predisposition to patellar maltracking. Our findings regarding the trochlea were therefore consistent with observations in sports medicine, that females had higher rates of patellar instability (including patellofemoral pain and sensation of patellar subluxation),higher rates of primary dislocation during the high-risk adolescent period (age 10-17), and higher rates of recurrent dislocations in patients with instability symptoms [37,38].
Other than the trochlea, most measures of the distal femur, when adjusting for height, weight and other confounding factors, were not significantly different between males and females (including aspect ratios and notch width). However, one measure that reported important in the assessment of knee arthroplasty functionality was the posterior femoral offset. This measurement was found to be greater in males than females in two of three anatomic studies. Hence, customized arthroplasties designed with attention to the offset were probably important to subsequent restoration of function in patients requiring surgery, and care was often taken to consider this factor in treatment planning [39].
In the patella, it appeared that sex differences likely persisted after adjusting for confounding factors, with males had generally larger and exaggerated morphology compared to females. Additionally, it was very interesting that the sex differences of the patella were enough that a trained neural network in forensic CT modeling can identify patient sex with a high degree of accuracy [32,32]. These findings might have clinical implications to both developing injury (also potentially contributing to patellar instability/dislocation in addition to trochlear morphology), and to arthroplasty design and surgical treatment. Similarly, in the tibia, males tended to have larger tibias with more pronounced features (such as greater depth or greater anteroposterior to lateral diameter). These proximal tibial differences likely had clinical implications, with resulting alterations to the biomechanics and stability of the knee joint, shear forces (and therefore injury risk) on the intra-articular soft tissues such as cruciate ligaments, articular cartilage and menisci might be different between the sexes as a consequence.
Our comprehensive review had limitations. We excluded studies that were not written in the English language, which limited the scope of our search. We included studies focusing on certain ethnic/racial populations, such as studies looking specifically at Chinese subjects only [12,20,27,28,40-44]. Such a specific patient population focus might limit the generalizability of the findings; we did not adjust for ethnicity, race or age, as not enough data was available to do so. Also, as already mentioned, the study populations, research methodology and outcome measures were highly variable between investigations; due to the heterogeneity of studies, a quality assessment tool could not be utilized to capture quality differences and a meta-analysis could not be performed. In addition, measurement from different studies made by different modalities could influence the results, but there was no inter-modality comparison available to determine the accuracy and interplay between modalities.
In conclusion, while a robust understanding of the bony and cartilaginous sex differences in the knee were still emerging, we had provided a compendium of current knowledge in this important field. Such information was valuable to potentially providing a customized radiology interpretation for individual patients of different sexes and identifying patients at risk of injury. In this way, imaging metrics of sex differences might help promote better surgical outcomes and post-operative care, as an understanding of the sex differences continues to be elucidated. Finding metrics that had no sex difference would also be beneficial in directing resources away from sex-specific approaches in sports medicine, to those that were influenced by patient sex. Radiology was uniquely positioned to study these anatomic differences in a noninvasive manner with continually improving imaging techniques, including high-resolution and increasingly fast acquisitions, which can improve the standardization of measurements and findings. Moving forward, investigations looking at sex differences should conduct rigorous, reproducible measurements that were normalized to patient height, weight, and femur length at a minimum, so that any sex differences discovered can be attributable to sex rather than patient size alone.
Individuals who are not authors: We thank Katie Lobner, clinical informationist at the Johns Hopkins Welch Medical library, for her assistance in developing/refining our search strategy and assistance in collecting the articles reviewed for this project.
None.