To investigate the effect of a single-session manual needle acupuncture procedure on peak isometric muscle torque and resistance to muscle fatigue.
Healthy participants (mean age 27.8 ± 9.8 years) were assigned to an acupuncture or control group. Each participant was required to perform a peak isometric muscle torque and 1-min isometric muscle fatigue task of the right knee extensors. Following 20-min of needle acupuncture (acupuncture group, N = 17) or 20-min rest (control group, N = 8), participants were required to repeat the peak isometric muscle torque and 1-min isometric muscle fatigue tasks. The acupoints included LV3, LI4, and GV20. ANOVA was performed for peak isometric muscle torque, muscle fatigue, muscle fatigue coefficient of variation (CV%), blood lactate, and heart rate.
There was a group by time interaction for the peak isometric torque (F = 5.9, P = 0.02, partial eta squared = 0.21). The control group revealed a 6.4% decline and the acupuncture group showed a 1.6% increase and in the repeat performance of the peak isometric muscle torque. No main effects were observed for isometric muscle fatigue, CV%, blood lactate, or heart rate.
Repeat performance of the peak isometric muscle torque was sustained following a 20-min acupuncture procedure compared to a decline in the control group following a 20-min rest procedure. Differences between groups might be associated with acute acupuncture procedure and acquired performance bias.
Exercise, Performance, Strength, Lactate, Heartrate
The procedure of needle acupuncture requires the insertion and manipulation of a fine needle at selected acupoints on the body to induce therapeutic effects. Acupuncture is widely recognised as a treatment for several disorders [1-3]. Application of acupuncture has been shown to influence cardiovascular performance including blood pressure [4], heart rate [5] and endothelial function [6]. It has been proposed that acupuncture elicits discharges in afferent nerve fibers and initiates the release of neurotransmitters and bio substances to mediate physiological function [7-9].
Based on the effects of acupuncture on physiological function, it has been proposed that this procedure might enhance exercise performance and recovery [10,11]. There are limited controlled trials, however, in one study the level of muscle soreness following exercise was reduced following acupuncture compared to the control group [12]. In a 20-km cycling trial among trained cyclists, the perceived exertion was significantly elevated following acupuncture compared to sham and control groups [13]. The increased perceived exertion immediately after exercise in the acupuncture group was associated with reduced cycling time-trial and lower limb pain, however, this was not statistically significant. During sports competition among elite football athletes, acupuncture was shown to reduce cortisol levels and lower the subjective rating of muscle tension and fatigue [14]. In contrast, no difference in rating of perceived exertion, oxygen uptake, or heart rate was shown during cycling exercise following acupuncture procedure [15]. In the animal model, previous research has shown enhanced swimming endurance following acupuncture [16].
The potential of acupuncture to mediate physical performance is of benefit for athletes and patients with chronic diseases [17]. Additional research is required to evaluate the effects of an acute single-session acupuncture on exercise performance and fatigue. Therefore, the purpose of this study was to assess whether an acute single-session needle acupuncture procedure influences peak isometric muscle torque and resistance to muscle fatigue in healthy participants.
The participants included 25 apparently healthy subjects with a mean age (± SD) of 27.8 ± 9.8 years. All participants were over 18 years of age. Each participant was screened with a Physical Activity Readiness questionnaire (PAR-Q), [18] prior to exercise. Exclusion criteria comprised the use of medications such as analgesics and anti-inflammatory drugs, prior history of leg/knee injury or surgery, acute and chronic disease. The study was conducted with the approval of Charles Sturt University Human Research Ethics Committee (PN: 2014/022) and all participants signed a letter of informed consent. Participants had no experience or minimal (several years prior) previous experience with acupuncture procedure.
Participants completed the PAR-Q, assessments for height and bodyweight prior to performing exercise within a controlled laboratory environment. Random assignment of participants into acupuncture treatment and control groups was performed prior to exercise. Group characteristics for the acupuncture and control groups are shown in Table 1. Following the group assignment and assessment of physical characteristics, each participant was required to perform exercise to determine the peak isometric muscle torque (PT) and the Muscle Fatigue (MF) of the right knee extensor muscle group at before (Pre) and after (Post) 20-min acupuncture or 20-min rest period. Following the assessment of Pre-PT and Pre-MF, the acupuncture group completed acupuncture procedure for 20-min and the control group rested for 20-min. Following the acupuncture procedure or rest period, a Post-assessment of the PT and the MF were performed. A timeline of the sequence of assessments is shown in Figure 1. Participants were verbally encouraged during the performance of each isometric PT and MF procedure.
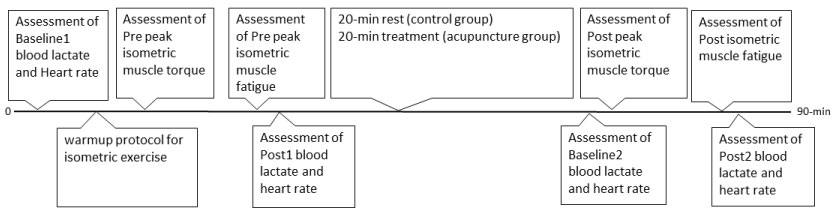 Figure 1: Timeline showing the sequencing of assessments for the acupuncture and control groups. View Figure 1
Figure 1: Timeline showing the sequencing of assessments for the acupuncture and control groups. View Figure 1
Table 1: Demographic and anthropometric characteristics of the acupuncture and control groups. View Table 1
For acupuncture treatment, a combination of bilateral Taichong (LV3) and Hegu (LI4), and unilateral Baihui (GV20) was performed. LV3 is located on the dorsum of the foot, in the depression distal to the junction of the first and second metatarsal bones. LI4 is located on the dorsum of the hand between the first and second metacarpal bones approximately in the middle of the second metacarpal bone on the radial side. GV20 is located on the midline of the head approximately on the midpoint of the line connecting the apex of the two auricles.
The acupuncture treatment procedure was performed by qualified acupuncturist (BK). Acupuncture treatment was performed for 20-min following the Pre isometric MF procedure. For each acupoint, the inserted needle was manipulated at 5-min intervals over 20-min by the acupuncturist. During the acupuncture procedure, each participant was reclined in the Humac seat and the leg was removed from the lever arm strapping. Following the 20-min acupuncture treatment, participants completed a repeat (Post)assessment of the PT and MF.
For the control participants, the Humac seat was reclined and the leg removed from the lever arm strapping for a 20-min rest period following the Pre PT and MF procedure. Following the 20-min rest period the control participants completed a repeat (Post)assessment of the PT and MF.
To assess the peak isometric muscle torque and muscle fatigue each participant was required to perform maximal contraction of the right knee extensor muscles while positioned in a dynamometer (Humac, Computer Sports Medicine Inc., Stoughton). The PT and MF were assessed for each participant following individualised adjustments for dynamometer height, lever arm length, chair tilt, chair rotation, with the lower limb lever arm set for a knee angle of 110°.
For the PT assessment, each participant was required to complete a standardised warm-up procedure comprising 2 × 50%, 2 × 75%, 2 × 90%, and 1 × 100% of self-determined maximum isometric effort with each trial separated by 1-min rest. Following a 2-min rest period after the warm-up procedure, participants were required to perform 5 × 100% of maximum isometric effort contractions, each separated by 1-min rest period. The PT was determined as the single highest peak torque measured across the 5 maximum efforts. The PT procedure was repeated after 20-min acupuncture treatment or 20-min rest for the acupuncture and control participants, respectively.
The MF was performed after a 2-min rest following the PT procedure. For the assessment of the MF, participants were required to perform maximal isometric contraction of the right knee extensor muscle group for 1-min while positioned in the Humac dynamometer. The fatigue index was determined by the percentage difference of the mean torque at the beginning 5-s epoch and the mean torque at the end 5-s epoch of the 1-min contraction. In addition to the fatigue index we also assessed for the percentage Coefficient of Variation (CV%) of the muscle torque at the beginning 5-s epoch and end 5-s epoch of the 1-min contraction. The CV% was determined as the standard deviation divided by the mean torque, multiplied by 100. The MF procedure was repeated after a 20-min rest (Control group) or after 20-min acupuncture treatment (Acupuncture group). Isometric muscle torque data was collected at 1000 samples per second and digitally stored using Lab view software (National Instruments Corp., Austin).
The Heart Rate (HR) was assessed by telemetry system (Polar RS200, Polar Electro, Kempele, Finland). Metabolic load was assessed from capillary blood [BLa-] at the finger site by whole blood analyser (Radiometer ABL 800 Flex, Copenhagen). Both the heart rate and blood lactate were assessed before and immediately after the MF procedure.
All muscle torque data were visually inspected for artefact prior to analysis. Statistical checks for homogeneity of data were performed for each analysis. Total sample size using G*Power for ANOVA with between factors and effect size at 0.25, power 0.8, was determined at 100 participants [19]. However, due to time and equipment limitations we aimed to recruit at least 20 participants as a convenience sample to assess potential trends.
Data are presented as mean ± standard deviation. Statistical analysis included between-group ANOVA (IBM SPSS statistics V.20, Armonk, NY, USA) with significance set at P < 0.05. Where P value approached significance (P < 0.2) magnitude-based inference analysis was performed using Hedges' g for unequal size groups to determine effect size differences [20]. Effect sizes of small, medium, large are 0.2, 0.5, and 0.8, respectfully.
The participant characteristics are shown in Table 1. Two control participants withdrew from the study due to unforeseen commitments.
Results for the PT at Pre and Post for the acupuncture and control group are shown in Figure 2. Box's test of equality of covariance matrices across groups showed no statistically significant difference between groups (P = 0.23). ANOVA for peak isometric muscle torque revealed a significant group x time interaction (F = 5.9, P = 0.02, partial eta squared = 0.21). The acupuncture group revealed a 1.6% increase and the control group revealed a 6.4% decrease in peak isometric muscle torque at Post. There was no main effect for time (P = 0.17) or group (P = 0.28). Effect size analysis between acupuncture and control groups at Post revealed a Hedges' g of 0.63.
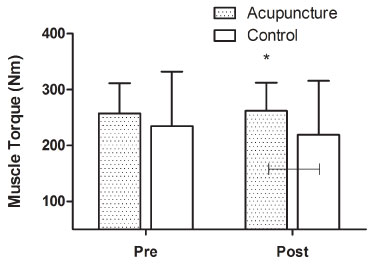 Figure 2: Peak isometric muscle torque (± SD) at Pre and Post for the acupuncture and control groups. *Significant interaction between Acupuncture and Control groups at Post (P < 0.05). Effect size analysis performed, horizontal bar. View Figure 2
Figure 2: Peak isometric muscle torque (± SD) at Pre and Post for the acupuncture and control groups. *Significant interaction between Acupuncture and Control groups at Post (P < 0.05). Effect size analysis performed, horizontal bar. View Figure 2
Results for the isometric muscle fatigue at Pre and Post exercise for the acupuncture and control groups are shown in Figure 3a. Box's test of equality of covariance matrices across groups showed no statistically significant difference (P = 0.75). ANOVA revealed no significant main effect for time (P = 0.85) or group x time interaction (P = 0.96) for isometric muscle fatigue.
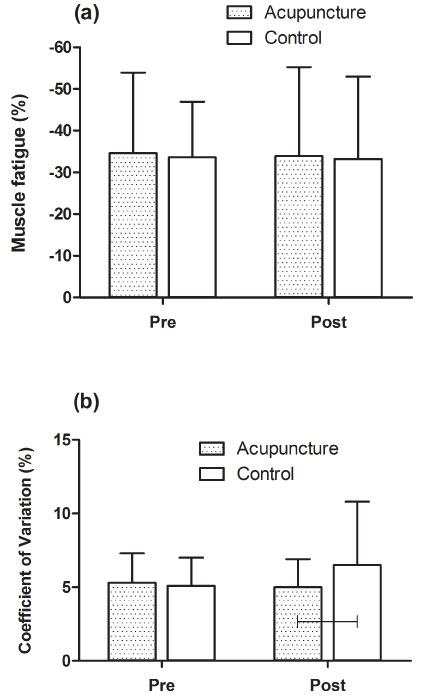 Figure 3: (a) Percentage muscle fatigue; (b) Muscle torque coefficient of variation for acupuncture and control groups at Pre and Post. Effect size analysis performed, horizontal bar. View Figure 3
Figure 3: (a) Percentage muscle fatigue; (b) Muscle torque coefficient of variation for acupuncture and control groups at Pre and Post. Effect size analysis performed, horizontal bar. View Figure 3
Results for the isometric muscle fatigue CV% at Pre and Post for the acupuncture and control group are shown in Figure 3b. Box's test of equality of covariance matrices across groups showed no statistically significant difference (P = 0.09). ANOVA on the CV% for isometric muscle fatigue revealed no significant main effect for time (P = 0.32) or group x time interaction (P = 0.14). Effect size analysis between acupuncture and control groups at Post revealed a Hedges' g of 0.53.
Results for blood lactate concentration for the acupuncture and control groups at Pre and Post 1-min isometric muscle fatigue are shown in Figure 4a. Checks for homogeneity of variances showed no statistically significant difference between groups (P > 0.05). ANOVA for blood lactate concentration revealed no significant difference between groups at Baseline1 (P = 0.44), Post1 (P = 0.42), Baseline2 (P = 0.07), or Post2 (P = 0.87). Effect size analysis between acupuncture and control groups at Baseline2 reveals Hedges' g of 0.93.
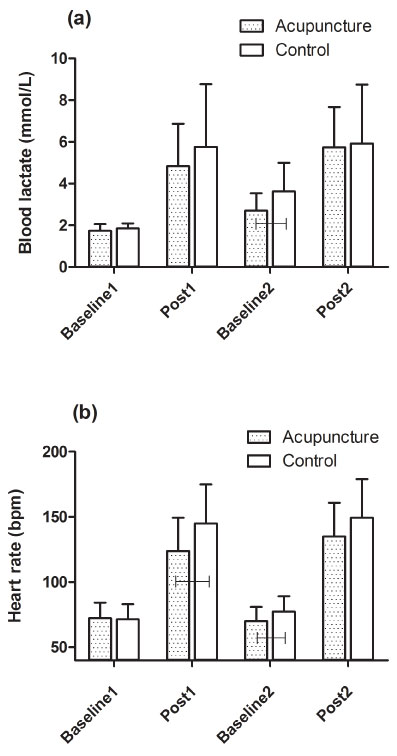 Figure 4: (a) Blood lactate responses before (Baseline1, Baseline2) and after (Post1, Post2) repeated isometric muscle fatigue exercise for acupuncture and control group; (b) Heart rate responses before (Baseline1, Baseline2) and after (Post1, Post2) repeated isometric muscle fatigue exercise for the acupuncture and control group. Effect size analysis performed, horizontal bars. View Figure 4
Figure 4: (a) Blood lactate responses before (Baseline1, Baseline2) and after (Post1, Post2) repeated isometric muscle fatigue exercise for acupuncture and control group; (b) Heart rate responses before (Baseline1, Baseline2) and after (Post1, Post2) repeated isometric muscle fatigue exercise for the acupuncture and control group. Effect size analysis performed, horizontal bars. View Figure 4
Results for heart rate at Pre and Post-isometric muscle fatigue exercise for the acupuncture and control groups are shown in Figure 4b. Tests for homogeneity of variances showed no statistically significant difference between groups (P > 0.05). ANOVA for heart rate revealed no significant difference between groups at Baseline1 (P = 0.85), Post1 (P = 0.08), Baseline2 (P = 0.14), or Post2 (P = 0.23). Results for effect size analysis between acupuncture and control groups at Post1 and Baseline2 reveals Hedges' g of 0.79 and 0.65, respectively.
The present results show a significant difference in the repeat performance of the peak isometric muscle torque following acute acupuncture procedure compared to the resting control group. After the 20-min acupuncture procedure, the acupuncture group were able to repeat the peak isometric torque at a similar level to the pre-acupuncture peak muscle torque assessment. However, the control group revealed a 6.4% decline in the repeat performance of peak isometric muscle torque following the 20-min rest procedure. This performance difference in the acupuncture group might be associated with the acute needle acupuncture procedure or an acquired performance bias. Moreover, we cannot definitively report that acupuncture sustained the repeat performance of peak isometric strength since our study is underpowered. This result is further discussed in the context of the additional performance measures assessed in the present study.
The present results did not show a significant improvement in peak isometric muscle torque in the acupuncture group following the acupuncture treatment. In contrast, previous research shows a 7.7% increase in peak isometric muscle torque following acupuncture [21]. A potential reason why the present study did not show an increase in the peak muscle torque compared to previous research is that we performed a repeat trial of the peak muscle torque immediately after the 20-min acupuncture procedure, whereas previous research compared the effect of acute acupuncture at repeat trials of 1-week apart. Instead, our results show potential for acupuncture to sustain peak muscle torque with repeat efforts. In accord with our results, previous research has also shown no difference in peak torque during a knee flexion-extension task following an acute acupuncture procedure [22].
Previous research has also shown that acute acupuncture can significantly reduce the peak muscle force, although this effect was associated with acupuncture points located at the exercise muscle site [23]. The acupoints in the present study included LV3, LI4, and GV20 which were located away from the exercising muscle site in order to avert antagonistic effects and to elicit central and peripheral influence on performance [24,25]. GV20 has shown improved cerebral blood flow [26]. Significant increases in autonomic nervous system activity and reduced muscle fatigue have been associated with acupoint LI4 [14,27]. LV3 was shown to enhance perceived exertion during an exercise endurance task [13]. However, there is no standard practice of acupoint selection for enhancing exercise performance [28]. In summary, the sustained repeat performance of peak muscle strength in the present study might be associated with the central and peripheral effects of acupuncture.
The effect of manual needle acupuncture procedure on isometric muscle fatigue was investigated in the present study by the 1-min isometric muscle fatigue task. Our results show no difference in the decline of muscle torque during the 1-min fatigue task between the acupuncture and control groups. This is in accord with previous research showing no difference in the muscle fatigue index following acupuncture procedure [22]. However, in the present study there was a medium effect size difference in the coefficient of variation of muscle torque between the acupuncture and control group for the repeat performance of the muscle fatigue task. The coefficient of variation represents a relative variation of the distribution of data [29] for the muscle torque output during the 1-min fatigue task. Our results show a 5.7% reduced Coefficient of Variation (CV) in the acupuncture group whereas the control group revealed a 30% increase in CV for the repeat performance of the muscle fatigue task. The effect size difference between groups was present only in the repeat assessment of the CV for the 1-min muscle fatigue task. This suggests that the acupuncture group was able to produce less variability in the muscle torque during the isometric muscle fatigue task following the 20-min acupuncture procedure compared to the control group. Previous research show changes in electromyographic (EMG) activity in the performing muscle following acupuncture procedure [22]. The alterations in EMG activity were attributed to the indwelling needle inducing micro-punctuation at the muscle site, potentially evoking changes in muscle use and distribution. However, the present study did not involve needle penetration at the exercising muscle site. In summary, the acupuncture group showed a medium effect size difference in the muscle torque coefficient of variation compared to the control group, however, this effect was not statistically significant.
Previous research show significant differences in lactate metabolism during cycling exercise following acupuncture [30]. This suggests that acupuncture treatment enhances the plasma clearance of lactate which potentially improves exercise performance. In previous research, 5-weeks of acupuncture treatment revealed a statistically significant 6.6% increase in exercise work output at the lactate-determined anaerobic threshold, compared to a 3.4% decline in the control group [30]. In the present results, there was no statistically significant difference in blood lactate concentration between the acupuncture and control groups for the 1-min isometric muscle fatigue task. There was evidence in the effect size analysis showing that the acupuncture group had a greater return to baseline lactate level compared to the control group. Our data are limited here in that further baseline assessments of lactate levels were not performed after the repeated muscle fatigue task and this may have yielded further information on the lactate kinetics following repeated exercise.
Potential reason for the non-significant effect of acupuncture on blood lactate is that the present study included a single 20-min acute acupuncture procedure prior to the repeat performance of the muscle fatigue task. In practice, acupuncture therapy requires a series of individualised treatments [31] in order to induce clinical effects. Our results suggest that a single-session acupuncture procedure does not show a significant difference in the plasma lactate kinetics compared to a control group during an isometric muscle fatigue task.
In the present results, there was no statistically significant difference in the heart rate response for the 1-min isometric muscle fatigue exercise between the acupuncture and control groups. In contrast, previous research shows a significant reduction in heart rate during aerobic exercise and a more rapid recovery heart rate in the post-exercise period following acupuncture [30]. It is possible that the non-significant effect on heart rate in the present results may be due to the application of a single acupuncture treatment [15] compared to 5 treatments as performed in previous research by Ehrlich and Haber [30]. Congruently, 10 acupuncture-combination treatments over 5 weeks revealed lower exercise heart rate responses in the acupuncture group [32]. In contrast, it has previously been shown that a single acupuncture procedure reduces heart rate via changes in autonomic function [27]. However, this effect was shown at 60-min post-acupuncture whereas our heart rate data was recorded at 20-min after acupuncture.
Effect size differences in the present study were shown for the heart rate response in the acupuncture group at Post1 and Baseline2, however, this was not statistically significant. These heart rate differences were not shown in the repeat assessment of the muscle fatigue task at Post2. It is uncertain why the acupuncture group showed effect size differences in heart rate at Post1 when this was assessed before the acupuncture procedure. However, it is possible that the acupuncture group acquired differences due to the effect of treatment expectancy prior to the acupuncture procedure [33]. It has been shown that treatment expectancy during placebo acupuncture can independently show analgesic effects [34].
A limitation in the present study is that we did not include a sham acupuncture group. However, procedures involving sham acupuncture such as needling outside the acupoint are not physiologically inert. In research by Hübscher & Vogt, et al. [21], both needle-acupuncture and sham-acupuncture procedure showed significant effects. In this context, acupuncture procedure may elicit effects through a performance bias. However, it is possible with the inclusion of sham acupuncture procedures such as inert placebo laser [35] might have further differentiated the effect of treatment expectancy on performance outcomes in the present study.
In conclusion our results show that an acute single-session acupuncture procedure of 20-min sustained the repeat performance of the peak isometric muscle torque output compared to a control 20-min rest procedure. Differences between groups might be associated with acute acupuncture procedure and an acquired performance bias. Additional measures of muscle fatigue, blood lactate, and heart rate did not reveal significant differences between groups.
This research was supported by the Dongguk University Research Fund of 2014.
The study was conducted with the approval of Charles Sturt University Human Research Ethics Committee (PN: 2014/022) and all participants signed a letter of informed consent. Participants had no experience or minimal (several years prior) previous experience with acupuncture procedure.
The authors declare that they have no conflict of interest.