Introduction: Lung cancer being one of the main causes of mortality in Morocco, the coronavirus pandemic (COVID-19) has changed the processes of diagnosis and referral of lung cancer cases to oncology services. The objectives of this study were to describe the changes in the process of caring for lung cancer and to identify the activities affected during the COVID-19 pandemic in the Mohamed VI center for the treatment of cancers of the CHU IBN ROCHD of Casablanca in Morocco.
Method: This was a longitudinal study carried out in the Mohamed VI center for the treatment of cancers of the CHU IBN ROCHD of Casablanca in Morocco from January 2019 to December 2020, including patients with lung cancer treated at the center Mohammad VI. The KHI2 test has been used to test the association between the proportions of activities during the periods without-COVID-19 and with COVID-19 with a value of p ≤ 0.05 as the threshold of significance. Data have been analyzed using SPSS 16 software.
Results: We included 955 patients, 47% of whom during the COVID-19 period. Eighty-nine percent (89%) of patients were male. The median age of patients was 63 years (interquartile range was 13 years). There was a significant difference between the period without COVID-19 and the COVID-19 period concerning the diagnostic stage of lung cancer (II: without- COVID-19 = 61%, with COVID-19 = 39%, III: without- COVID-19 = 66%, with COVID-19 = 34%; IV: without- COVID-19 = 46% and with COVID-19 = 54%; p < 0.001), the proportion of patients referred to palliative care for symptomatic treatment (without- COVID-19 = 48% and with COVID-19 = 52%; p = 0.02) and the proportion of patients who did not have an extension assessment (without COVID-19 = 44.8%, with COVID-19 = 55.2%; p < 0.001).
Conclusion: The proportion of patients with metastatic lung cancer increased during the COVID-19 pandemic with a significant proportion of patients who could not receive specific cancer-related treatment, compared to the non- COVID-19 period.
COVID-19, Lung cancer, Stage
CHU: University Hospital Center; COVID-19: Coronavirus 2019; ENOVA: Electronic Patient Registration Computer System, M: Masculine, F: Feminine, NSCLC: Non-Small Cell Bronchopulmonary Carcinoma, SCLC: Cell Lung Carcinoma; POV: Out of Sight
Globally, cancer is the second leading cause of death in the world. Indeed, it causes about 10 million deaths per year [1]. In particular, lung cancer is a public health problem, as it is the second cancer in the world after breast cancer of all sexes combined and the main cause of mortality with nearly 2,206,771 deaths in 2020, which represents ten- eight percent (18%) of all cancer deaths [1].
In Morocco, it ranks first with 26% of all cancers recorded in men. It is also the leading cause of cancer death in Morocco with nearly 18.6% of all cancer deaths [1,2].
Over the past decade, lung cancer mortality has experienced a substantial decline, due to successful public health campaigns, such as smoking cessation and improved management, including diagnostic and therapeutic [3].
On December 2019, a new coronavirus called coronavirus 2019 (COVID-19) was first described in WUHAN, China [4]. On January 30, 2020, COVID-19 was declared a public health emergency by the World Health Organization (WHO) and later qualified as a pandemic on March 11, 2020 [5]. Like most countries in the world, Morocco had recorded its first case of COVID-19 on March 02, 2020, then an outbreak with widespread community transmission [6]. On March 20, 2020, it adopted drastic measures for collective and individual hygiene and safety on a large scale very early on, opting for general confinement and the compulsory wearing of mask [7]. As a result, the pandemic has led to a sharp drop in referrals to oncology services, resulting in an increase in the number of cases of lung cancer discovered at an advanced stage, leading to an increase in the mortality rate [8].
Thus, the Ministry of Health adopted a response plan based on sanctuary (this was a policy of prioritizing oncology centers by maintaining activities and staff during the COVID-19 pandemic without development) as much as possible of oncology centers. In addition, a plan to strengthen the accessibility of treatment for cancer patients far from oncology centers has been put in place to ensure their transport in order to ensure continuity of care [9].
Despite these measures, the high contagiousness of the virus with the risk of contamination of patients and caregivers will lead to the implementation of barrier measures and restrictive health protocols that can seriously limit care capacities, including early diagnosis [10].
The objectives of this study were to describe the changes in the process of caring for lung cancer and to identify the activities affected by the COVID-19 pandemic in the Mohamed VI center for the treatment of cancers at the CHU IBN ROCHD of Casablanca in Morocco.
The Mohamed VI center for the treatment of cancers at the CHU IBN ROCHD of Casablanca has a capacity of 37 hospital beds and 50 treatment chairs with 4 accelerators and a scanner. The center receives 4,000 patients/month and hospitalizes 350 to 400 patients/month.
This was a longitudinal study carried out in the Mohamed VI center for the treatment of cancers at the CHU IBN ROCHD of Casablanca, Morocco from January 2019 to December 2020.
The study concerned patients with lung cancer treated at the Mohammed VI center for the treatment of cancers during the study period.
We included patients who were received in the center with a histologically confirmed diagnosis of lung cancer from January 2019 to December 2020 and we excluded cases of radiological suspicion without histological diagnosis and non-usable medical records.
All patients who met the inclusion criteria were included in the study.
Our variables were; age in years, sex, smoking (yes and no). The histological type which had as modalities non-small cell bronchopulmonary carcinoma (NSCLC) and small cell lung carcinoma (SCLC). The diagnostic stage (II, III and IV). Exclusive care in the palliative care unit (yes and no). The holding of multidisciplinary consultation (yes and no). The status of follow-up patients categorized by dead, lost to sight and alive. The period which had as modality period "without covid-19" represented by the year 2019 and "covid-19 period" represented by 2020. The therapeutic delay is the time interval between admission and the start of treatment expressed in number of days (< 15, 15-30 and > 30 days). The consultation period (in number of months) is the time interval between the first symptoms and the first consultation (< 3, 3-6, 7-12 and > 12 months). The access time (number of days) is the time interval between histological confirmation and access (admission) to the center.
The diagnostic delay (in number of days) is the time interval between the first (1st) radiological assessment and the diagnosis of histological confirmation of the cancer (> 30 days: yes and no). The extension assessment was categorized according to whether it was benefited or not (yes and no).
The data were collected from the ENOVA computerized platform (computer system for electronic registration of all patients admitted for cancer) from an operating sheet designed on the basis of literature and medical records.
The study was authorized by the head of service of the Mohamed VI center for the treatment of cancers in Casablanca. Anonymity and data protection were considered with limited access to investigators.
The qualitative data were described by the percentages and the quantitative by the median with the interquartile range. The KHI2 test has been used to compare the proportions of the period without-COVID-19 to those of the period with COVID-19. The significance level was set at 0.05. Data were analyzed using SPSS version 16 software.
On the 955 patients included in our study, nearly 90% of the patients were male. The median age of the patients was 63 years with 13 years as an interquartile range. Smoking accounted for 85% of patients. Patients cared for during the COVID-19 period represented 47% of patients. The proportion of stage IV patients was 66%. The therapeutic delay was < 15 days for 76% of patients. The diagnostic delay was less than 30 days for 77% of patients. Extension assessment was performed in 56% of patients. Lost to follow-up accounted for 43% of patients (see Table 1, Figure 1 and Figure 2 for details).
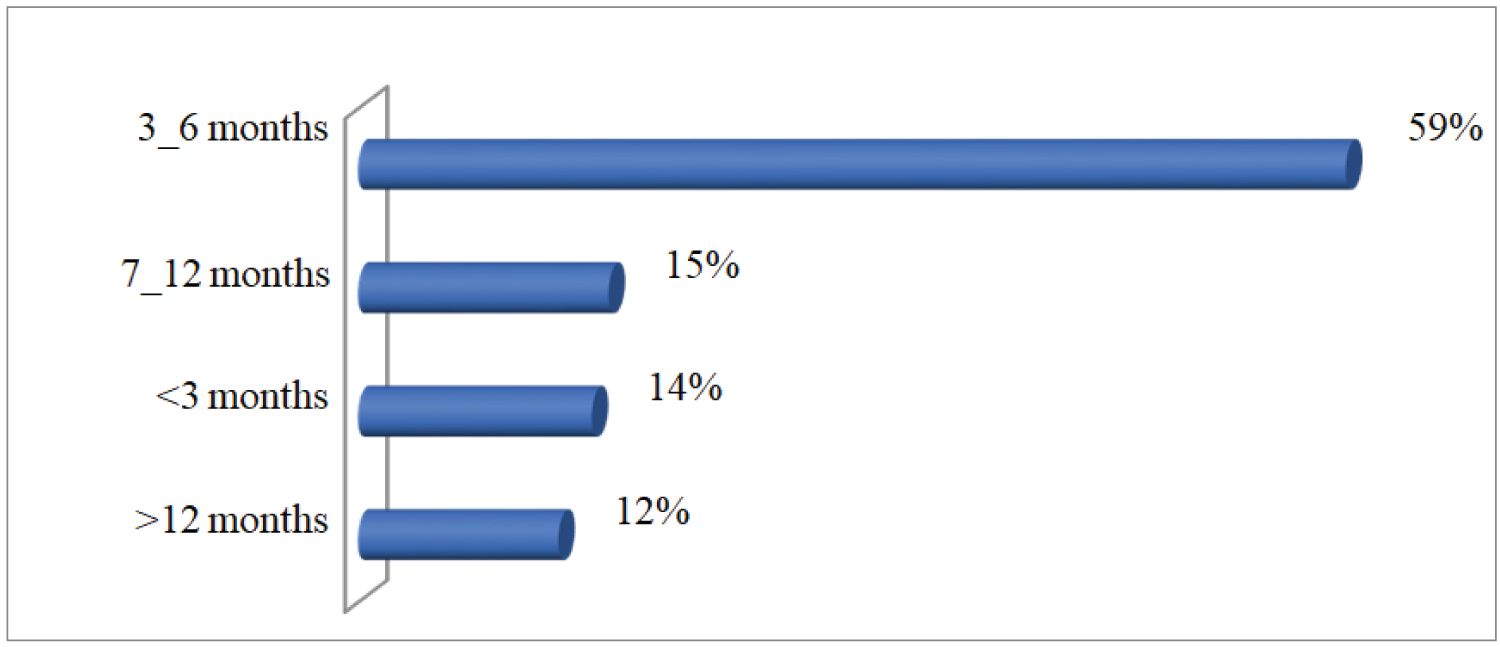 Figure 1: Distribution of consultation period.
View Figure 1
Figure 1: Distribution of consultation period.
View Figure 1
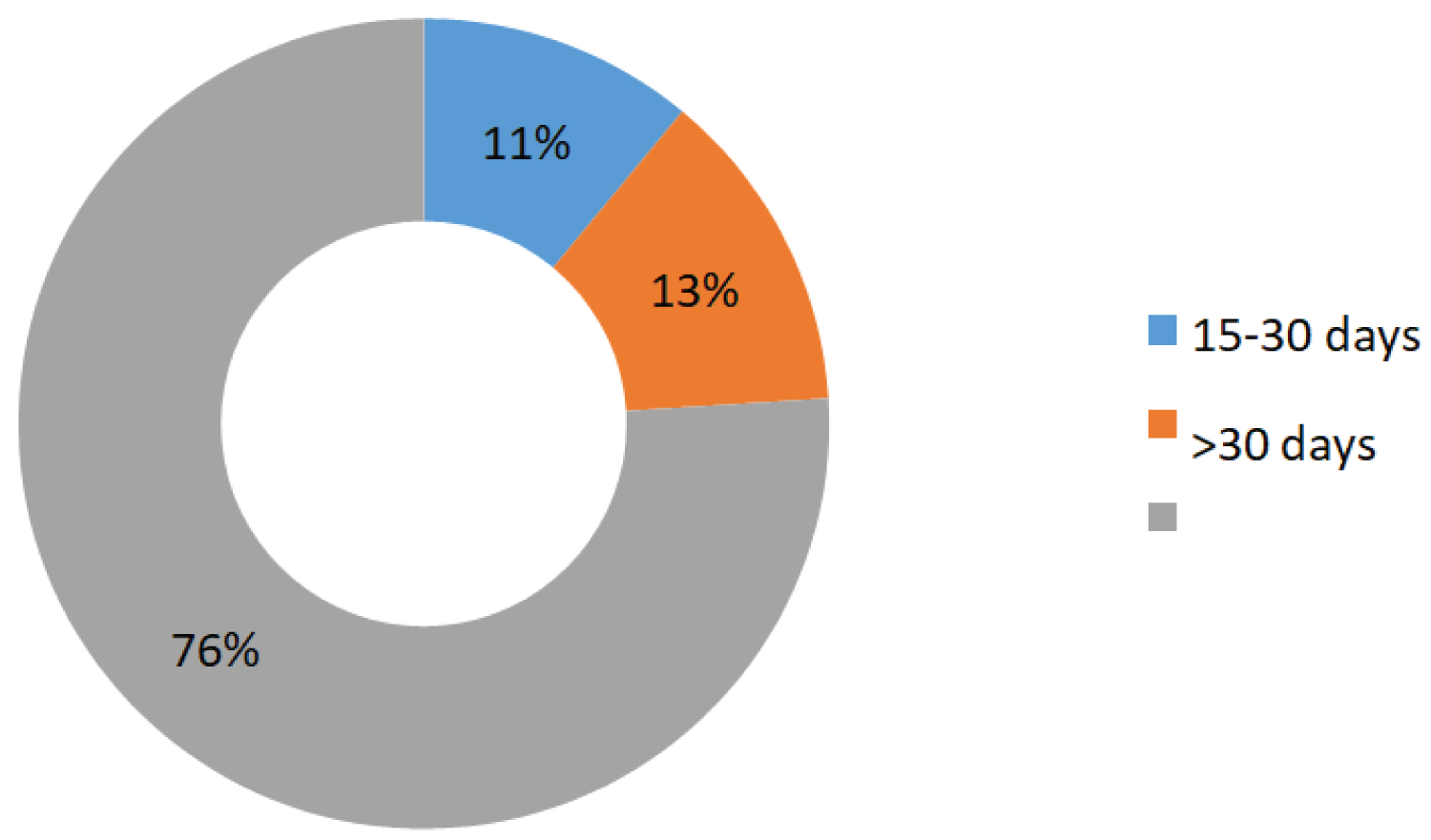 Figure 2: Distribution of therapeutic delay.
View Figure 2
Figure 2: Distribution of therapeutic delay.
View Figure 2
Table 1: Description of patients and management process. View Table 1
There was a significant change between the COVID-19 and no- COVID-19 periods regarding stage of diagnosis, performance of extension workup, and exclusive management in the palliative care unit (see Figure 3, Figure 4 and Figure 5).
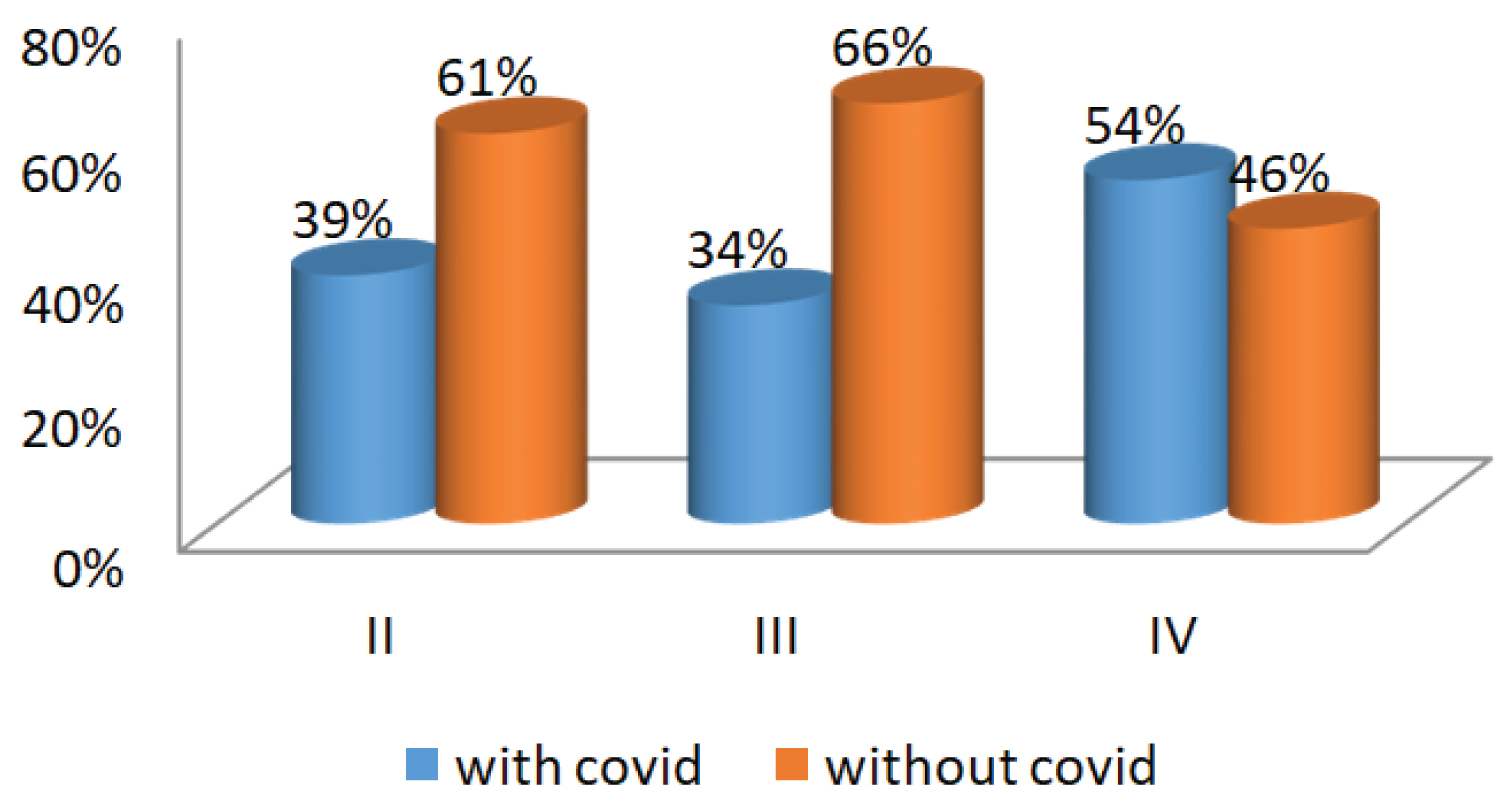 Figure 3: Distribution of stages according the periods.
View Figure 3
Figure 3: Distribution of stages according the periods.
View Figure 3
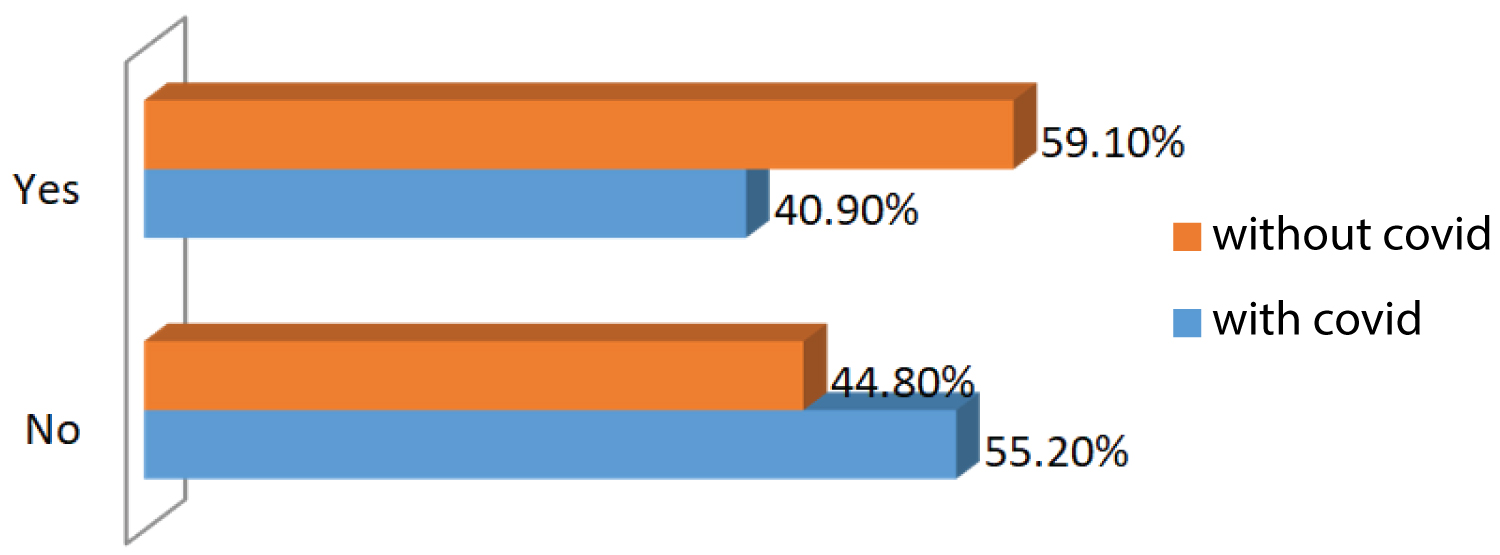 Figure 4: Distribution of spreading assessment according the period.
View Figure 4
Figure 4: Distribution of spreading assessment according the period.
View Figure 4
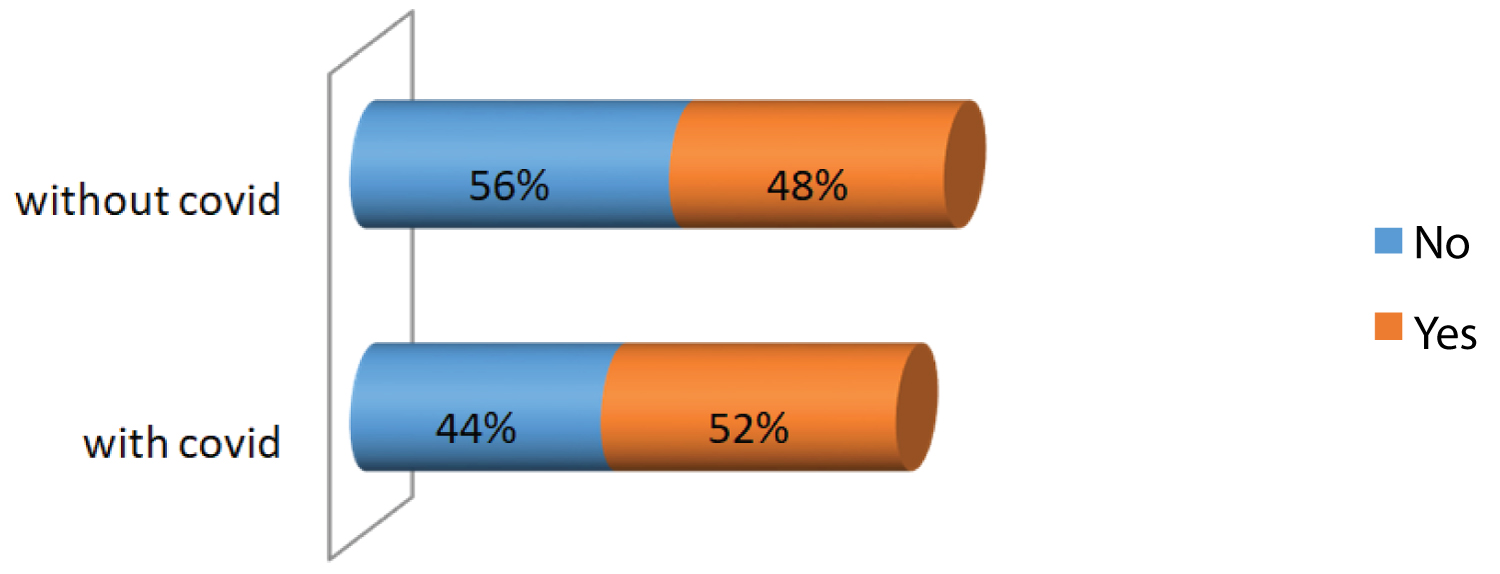 Figure 5: Distribution of palliative care according the period.
View Figure 5
Figure 5: Distribution of palliative care according the period.
View Figure 5
The COVID-19 pandemic with the general confinement has negatively affected the health system in Morocco, in particular the limitation of access to health centers [11]. Indeed, a significant reorganization of healthcare provision has taken place to cope with the increasing burden of patients requiring hospitalization and to minimize infection of healthcare workers [12,13]. As a result, we observed in our study that the number of patients admitted for lung cancer in two thousand and twenty (2020) fell by fifteen percent (15%). Similarly, a report on the impact of COVID-19 on cancer diagnosis, showed that the registration of new cancer patients in the Dutch national cancer registry has dropped by around twenty-five percent (25%) between March and May two thousand and twenty (2020) [14]; which is significantly higher than the rate observed in our study. This can be explained by the adoption by the Moroccan Ministry of Health of a response plan based on the sanctuarization of oncology centers and by the adoption of a plan to strengthen the accessibility of remote cancer patients to ensure their transport [9].
Despite taking these measures, the proportion of patients who did not have an extension assessment increased significantly, thus reflecting the difficulty of these patients in carrying out the radiological assessment during the COVID-19 pandemic. Indeed, DABKEVICIENE. D, et al. in a retrospective study conducted in an oncology center in Lithuania had shown a reduction in diagnostic procedures including radiological assessment [15]. Also, the proportion of patients with lung cancer at a metastatic stage increased significantly, with a reduction in the percentage of patients diagnosed at early stages, these data are comparable to the study by PARK, et al. published in 2020 which showed that patients with advanced non-small cell lung carcinoma was higher during the COVID-19 pandemic compared to previous years [16].
As a result, nearly half of patients treated for lung cancer during the COVID-19 pandemic did not receive specific cancer-related treatment, which could translate into increased demand for palliative care services [17,18]. These services must cope with this increase by adopting new ways of working as resources are stretched beyond their normal capacities.
Nevertheless, measures have been taken in our center to minimize the negative effects on cancer patients and in particular those with lung cancer. Indeed, virtual or face-to-face multidisciplinary meetings have been maintained during the COVID-19 pandemic, which may be a factor in maintaining the quality of care [19]. In addition, the treatment time after admission to our center during and before COVID-19 was comparable with nearly three quarters (3/4) of patients receiving their treatments in less than fifteen (15) days after their admission.
Our data show that undiagnosed lung cancer cases, due to the suspension of cancer prevention programs and the limitation of visits to cancer centers, could be associated with a significant increase in newly diagnosed cancer cases at metastatic stages. In addition, late diagnosis often does not allow specific treatment related to cancer to be received, which is synonymous with a poor prognosis for these patients [4,20,21]. Indeed, several studies have shown high mortality from COVID-19 in cancer patients [8,22-25]. It is therefore necessary to evaluate the benefit/risk in the planning of visits and treatments.
This study was the first study in Morocco to examine the impact of the pandemic on the process of diagnosing lung cancer. But the monocentric aspect of the study calls for caution when interpreting and generalizing the results of this study.
This study found that the COVID-19 crisis could be involved in the changes observed in the process of managing lung cancer. Indeed, the proportion of patients with lung cancer at a metastatic stage increased significantly during the COVID-19 pandemic, resulting in a large number of patients who could not receive specific cancer treatment. Although the sanctuarization of oncology centers has minimized the negative impact of the COVID-19 pandemic, it is necessary to maintain these gains and develop other strategies to improve cancer services during pandemic outbreaks.
The authors declare no conflict of interest.
Not applicable.