The 7 essential elements for successful single immediate implant placement with TERUPLUG®collagen include 1 treatment-planning, 4 surgical, and 2 prosthetic keys, aiming to minimize soft- and hard-tissue complications for an optimal implant restoration both in the anterior and the posterior zone. All those keys are summarized to aid clinicians in the treatment planning of immediate implant placement cases. Based on the 7 essential elements, the management of an immediate implant with TERUPLUG® requires careful patient selection and reasonable treatment planning, along with precise execution by skillful clinicians in order to achieve successful results.
TERUPLUG ® , Dental implants, Immediate implant placement, Immediate provisionalization, Collagen
Several classifications have been proposed to define the terms used in implant placement and loading [1-3]. At the very beginning, terms such as immediate, delayed-immediate, delayed, recent, early, mature, late and many other non-standard definitions were applied by clinicians, making it difficult to interpret the data in the available literatures and to make clinical decision.
Hammerle, et al. proposed a classification of 4 categories (Type I-IV) [4], and later in the 3 rd volume of the ITI Treatment Guide series, for clarity reasons, Chen & Buser amended them by adding a descriptive terminology [2,5]. This classification system has been widely adopted until today (Figure 1). And all 4 options can be applied according to the pre operation clinical and radiographic assessment of the patients.
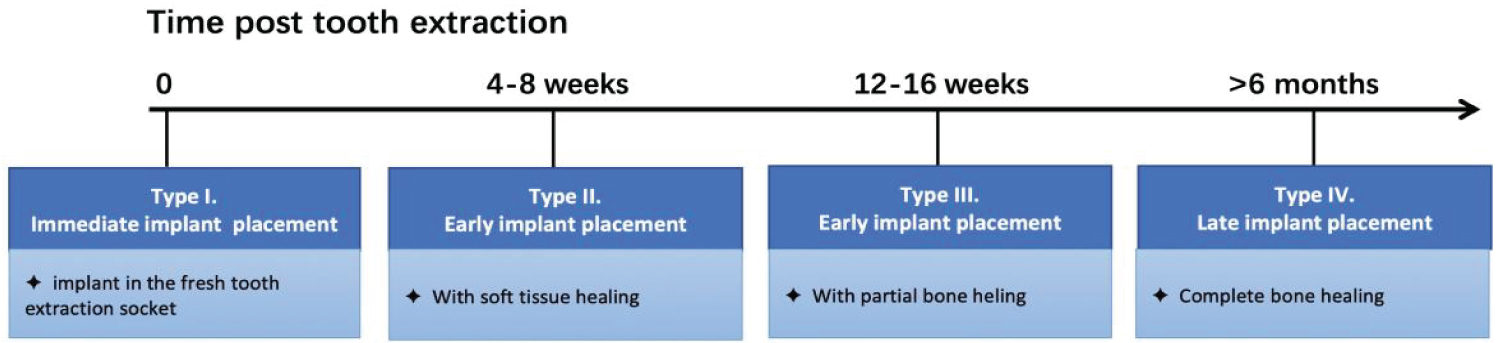 Figure 1:
View Figure 1
Figure 1:
View Figure 1
Besides, Gallucci, et al. classified implant-supported fixed dental prostheses (IFDPs) in partially edentulous patients into 9 types, among them, type 1A represents immediate implant placement + immediate restoration/loading; while Type 1B/C represents immediate implant placement + early loading/conventional loading [6]. Different implant placement and loading options can be clinically applied depending on patients’ specific condition.
Implant placement into healed sites has completely lost its dominance, because the dimensional ridge alterations post extraction often make the therapy approach to be complicated [7,8] and a healing period of at least 4-6 months post extraction prior to implant placement is not attractive to patients.
Thus, in the past 20 years, the timing of implant placement has become an important issue in the dental community [9,10]. Consequently, immediate implant placement after tooth extraction has become a viable surgical approach and widely accepted in clinical practice. It can reduce the number of surgeries needed and has the advantage of a shorter time to rehabilitate function and aesthetic, which provided an impetus to studies on this treatment modality.
In Atieh’s review, 10 studies with 629 implants were included [11]. Immediate single implant restoration/loading in extraction sockets in the aesthetic zone was associated with significantly higher risk of implant failure (risk ratio of 3.62, 95% confidence interval 1.15-11.45, P = 0.03) when compared with immediate restoration/loading in healed ridges. However, the bimodal approach showed favorable marginal bone changes after 1 year [1].
Although more tissue loss over time was observed in the overall mesial marginal bone level, distal marginal bone level and facial gingival level, less tissue loss over time was observed in the overall mesial papilla level and distal papilla level. The benefit of immediate implant placement and provisionalization (IIPP) on the maintenance of anterior single implant papillae has been well documented [12].
For immediate implant placement treatment, we can place an implant into a fresh tooth extraction socket with or without the use of filling materials or membranes, which is depending on the soft and hard tissue condition. A review by Chen & Buser analyzed 91 studies and concluded that bone augmentation procedures were effective in promoting bone fill and defect resolution at implants in post-extraction sites, especially for immediate and early implant placement [13].
Hom-Lay Wang validated a classification system for extraction sockets immediately after tooth removal based on soft and hard tissue conditions [14]. As this classification, extraction sockets can be graded as adequate (Type I), compromised (Type II) and deficient (Type III) according to soft and hard tissue variables. This classification system can guide clinicians to achieve predictable esthetic outcomes, especially in the anterior maxillary region. Most of type I extraction sockets can be treated using immediate implantation without bone graft. For type II sockets, only part of the cases can be treated with immediate implantation in conjunction with GBR and/or sub epithelial connective tissue grafting, while most of them can be treated using delayed implantation with GBR and/or sub epithelial connective tissue grafting. And for type III sockets, soft and hard tissues should be augmented first, and implants can be placed 5-6 months later.
Dennis P. Tarnow divided molar extraction sockets into three categories: Type A, B and C [15]. A type a molar socket has adequate septal bone to circumferentially contain the coronal portion of the implant within the bone completely, thus it is not necessary to graft these spaces. However, the sockets of the buccal roots of maxillary molars may be grafted to help reduce ridge remodeling and to achieve better esthetics and prosthetic contours. If a type A socket misses some or all of its buccal bone, an immediate implant may still be placed, with the buccal defect be grafted simultaneously. For type B socket, in which the implant is not fully contained by the septal bone, bone grafting in the gap is controversial. Even so, grafting the gap on the buccal of an immediate implant without primary closure is helpful to preserve the dimensions of the ridge. For type C, no septal bone is available for implant stabilization, as a result a very wide implant is required to engage the buccal and lingual walls at their thickest points, and graft is not necessary in this situation. If a type B or type C socket misses some or all of its buccal bone, a delayed placement protocol should be employed. For a single-rooted tooth socket, it is similar to make the final decision whether to graft or not.
Recently, various materials for soft and hard tissue regeneration in immediate implant placement have been reported. The ideal material should exhibit biocompatibility, shapeability, osteoconduction ability, bioresorbability and supportability. However, most of the graft materials applied in recent days are not that perfect. One potential candidate is collagen, which is proved effective for socket preservation and oro-antral fistula closure by many scholars [16-20]. As collagen is resorbable and shapeability, and is the main component of the bone, it has been widely applied into clinical practice.
Absorbable atelo-collagen sponges (TERUPLUG ® ;OLYMPUS TERUMO BIOMATERIALS, Tokyo, Japan) is consisted of type I and III collagen, and it is specially designed for soft and hard tissue regeneration. TERUPLUG ® were widely applied as filling materials in our immediate implant patients in the past few years. TERUPLUG ® is highly biocompatible. The product is in a sponge block configuration, and we can easily adapt it to any bone defect shape [21]. Thus we summed up 7 essential elements for successful single immediate implant placement with TERUPLUG ® based on our actual clinical experience.
How to minimize the risk of implant failure in immediate implant placement and loading? How to simplify the surgical procedure? How to gain a long-term, successful outcome without too much soft- and hard-tissue complications?
The purpose of this article is to identify 7 essential elements for performing immediate single-tooth replacement with TERUPLUG ® in both the anterior and posterior zone in adult patients with long-term, successful outcomes.
The 7 essential elements are as follows:
For immediate implant placement, as ITI consensus report in 2018, the presence of sufficient apical bone, intact extraction socket, thick gingival biotype and no acute infection at the extraction site is recommended. Furthermore, good patient compliance, adequate primary implant stability (implant torque 25-40 Ncm) and reasonable occlusal scheme (clear all centric and eccentric contacts) are crucial for immediate restoration. Clinicians should confirm these points before making the decision.
Minimally invasive tooth extraction, avoiding flap release, followed by immediate implant placement have been considered appropriate treatment for maintaining the architecture of hard and soft tissues, not only in the esthetic zone but also in the posterior area. And the regenerative material, TERUPLUG ® , should be left exposed during healing without elevation or advancement of full-thickness flap.
Tapered implant with a conical connection can maintain the level of the bone at the level of the implant, consequently extending the longevity of the implant. And among them, those implants with the final drill-implant diameter discrepancy (FD-IDD) ≥ 0.5 mm and those with deep threads minimized the incidence of rotational implant instability for the IIPP procedure.
The guideline for positioning an implant in IIPP procedure is the prof. Rojas-Vizcaya principle (3 mm apical and 2 mm buccal-principle 3A-2B) [22] (Figure 2). Surgical guide template can be applied if necessary in order to get an ideal implant location to ensure good available bone around.
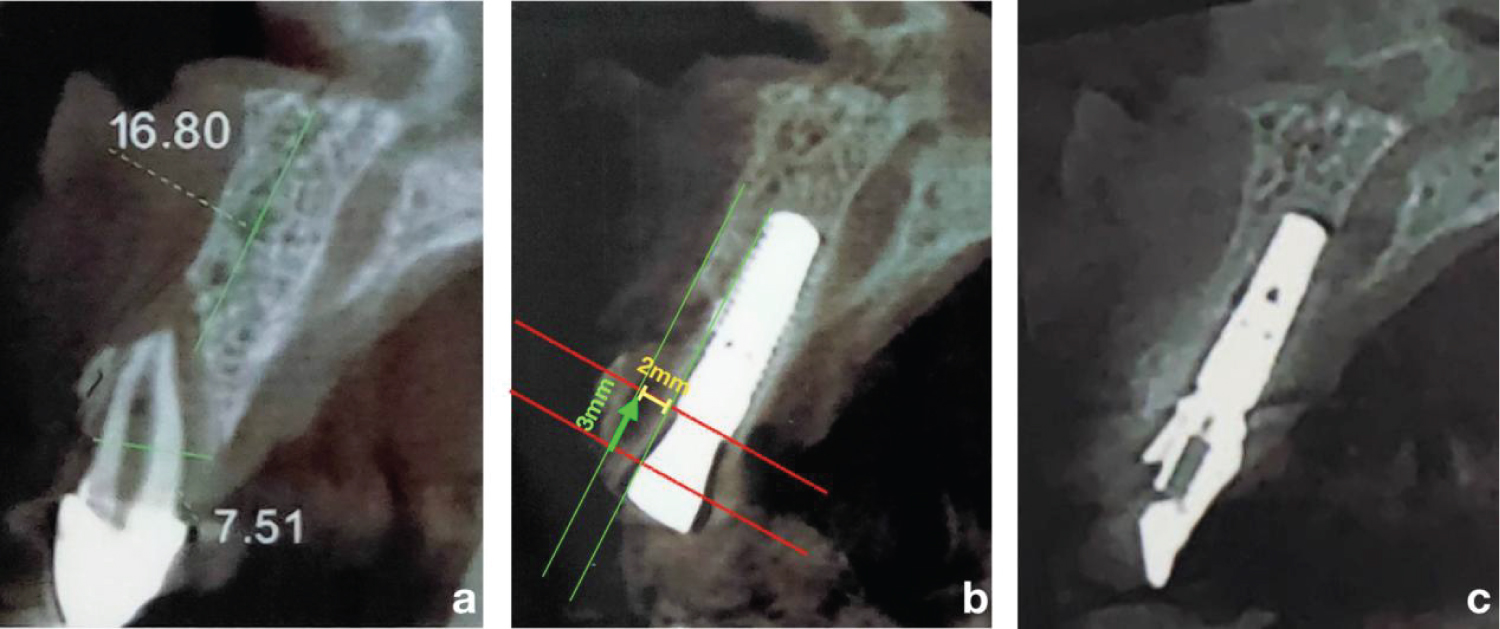 Figure 2:
View Figure 2
Figure 2:
View Figure 2
When an implant is placed into the fresh socket and a good primary stability is achieved, we should applied a healing abutment onto the implant. TERUPLUG ® should be folded into a “U” shape and stuffed into the gap at the buccal side and the interproximal side of the abutment subsequently, and vertically keep it out of contact with the threads of the implants if possible (Figure 3). Only in this way can clinicians exert TERUPLUG ® perfectly for soft- and hard-tissue augmentation.
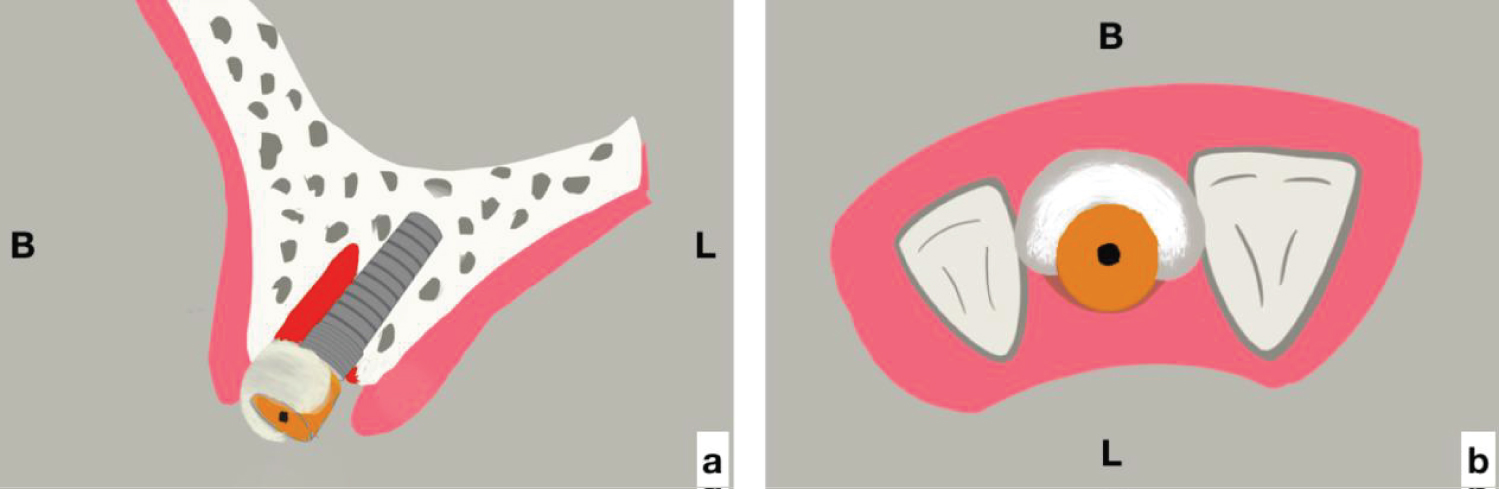 Figure 3:
View Figure 3
Figure 3:
View Figure 3
For the anterior site, a screw-retained immediate provisionalization is recommended unless for some special reasons, for the sake of maintenance of anterior single implant papillae and supporting the bone graft materials, such as TERUPLUG ® . Nevertheless, if the primary stability cannot be obtained, embedded implant healing might be a better choice.
For the posterior site, immediate restoration of the implant make little sense, on the contrary, it will increase the rate of failure because the bite force is complex in this area. Clinicians can apply a healing abutment as wide as possible, customizable healing abutment is also preferred. The best healing abutment to be considered should be that with platform transfer effect, in other words, clinicians should choose healing abutment with funnel-shaped contact area with the shoulder of the implant, and with columnar superstructure (Figure 4).
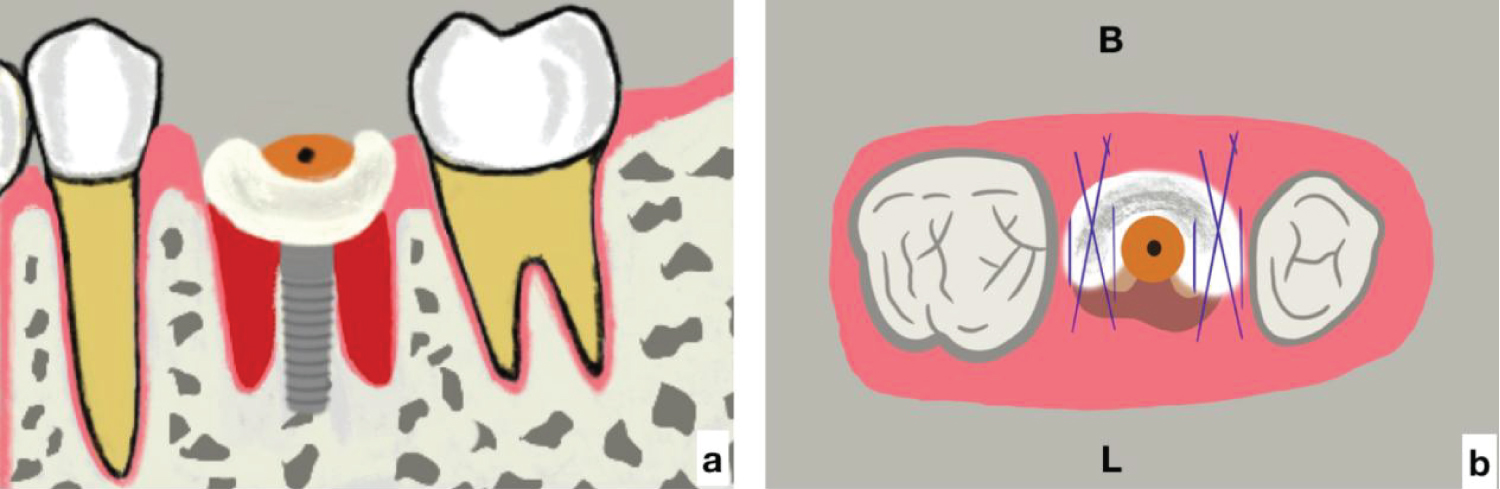 Figure 4:
View Figure 4
Figure 4:
View Figure 4
For the classification of the tooth extraction socket, Tarnow, et al. divided them into 3 groups, among which Type 1 represented extraction socket with intact facial bony wall and normal soft-tissue [23]. When the aforementioned conditions are present, the risk for recession of the facial mucosa or even the bone depressive can be greatly reduced, especially in the anterior maxilla.
As the clinical recommendations in Group 3 ITI Consensus Report in 2018 [24], immediate provisional restoration following immediate implant placement (Type 1A) in single edentulous spaces is a complex surgery and prosthodontics procedure, careful case selection criteria is recommended.
Although clinicians’ preferences, expertise, specific case- and patient-related factors are all taken into account, patient-centered advantage is a crucial prerequisite. Gallucci, et al. demonstrated that for immediate implant placement, the presence of sufficient apical bone, intact buccal plate, thick gingival biotype, absence of acute infection at the extraction site are predominant [6], while good patient compliance, adequate primary implant stability (implant torque 25-40 Ncm) and reasonable occlusal scheme (clear all centric and eccentric contacts) are crucial for immediate restoration [24].
Nevertheless, according to our experience, and also revealed in several recent studies, a thick wall phenotype is rarely present in the anterior maxilla [25,26], and most of the maxillary anterior teeth represent a thin soft tissue biotype. As a result, the facial bone wall is often not intact after the tooth extraction, making it impossible for patients scheduled for immediate single tooth implants to be treated with the planned procedure.
Clinicians should confirm these points according to the radiograph data and the clinical examination before making the decision, and reconfirm them throughout the operation, aiming at minimizing the risk of implant failure in immediate implant placement and loading, simplifying the surgical procedure, and gaining a long-term, successful outcome without too much soft- and hard-tissue complications.
Surgical trauma (sulcus incisions, rubber dam application, flap elevation) in implant surgery is a double-edged sword in immediate implant surgery. On one hand, it enables tooth extraction or implant placement to be easier and visible, thus make the operation simplify for clinicians. But on the other hand, as the blood supply to the residual facial bony wall is interrupted, the wound heal gets more slowly, and the facial bone is more easily to be resorbed. Consequently, the soft tissue complex can no longer be stabilized and will collapse into the newly formed space. As the buccal soft tissue occupies the place of the former buccal bone plate, the room for bone regeneration is reduced, leading to the observed major bucco-oral shrinkage.
Consistent with the above conclusions, Raes reported that flapless implant placement represented less recession of the mid-facial mucosa compared with open-flap immediate implant placement [27]. Fickl, et al. also concluded that the exposure of the buccal bone had a detrimental effect on the resorption process occurring after tooth extraction. In their study on beagle dogs [28], they found that leaving the periosteum in place decreased the resorption rate of the extraction socket, 0.7 mm additional volumetric shrinkage could be observed in flap surgery group. And treatment of the extraction socket with Bio-Oss Collagen seemed beneficial in limiting the resorption process after tooth extraction.
Does a flapless implant procedure make the surgical process to be simple? Of course not. It requires a skilled implant surgeon with talent and experience, for one thing, the implant bed preparation into the sloping anatomy of the palatal bone become difficult due to limited visual access during surgery, especially in the anterior region; for another, the risk of an unnoticed apical perforation on the facial bone wall increased if the preparation axis is incorrect [5].
Additionally
In DE Sanctis’s study, bone healing of immediate implants with four implant systems were analyzed, and no differences were demonstrated [29]. In those four implant systems, Astra Tech, 3i and Thommen were cylindrical-shaped two-piece implant designs, although the latter presented a 1 mm machined collar. Straumann was a cylindrical- shaped one-piece design with a 1.8 mm machined collar. The study indicates that different implant surfaces and different geometries did not influence the process of bone remodeling that occurs in the socket after tooth extraction.
Nevertheless, a predictable esthetic result is proved difficult to achieve when an immediately implant procedure is delivered in the anterior maxilla. Many scholars and clinicians have investigated the soft and hard tissue response in cases where the abutment diameter was smaller than the implant plateform, which is defined as platform switching. Canullo found that implant systems with platform switching can improve and maintain both osseous and soft tissue levels when immediately placed in extraction sockets [30]. The reason might be explained by the biologic width formed near the implant-abutment interface. When platform switching protocol is applied, the biologic width extends 1 mm horizontally form the abutment to the edge of the collar of the implant, and the remainder extends apically to this region, both facilitate bone preservation in immediately implant cases [31].
Additionally, Kan, et al. found that the implant morphology (cylindric vs. tapered) and the final drill-implant diameter discrepancy (FD-IDD) affect the primary implant stability, which is critical to achieving implant success, especially in a situation with immediate implant placement [32]. They found that tapered implant with an FD-IDD of ≥ 0.5 mm minimized the incidence of rotational implant instability for the IIPP procedure.
Simon, et al. proved that immediately placing tapered, roughened-surfaced implants with a novel 12°-angled prosthodontic platform in fresh extraction sockets can obtain a good peri-implant aesthetic outcome [33].
According to our experience for IIPP procedure, a tapered implant with a conical connection can maintain the level of the bone at the level of the implant, consequently extending the longevity of the implant. And among them, those implants with the final drill-implant diameter discrepancy (FD-IDD) ≥ 0.5 mm and with deep threads are better choice.
The 3D position of the implant affects the restoration and soft tissue directly, which is essential for both esthetically and functionally successful. Whether the implant treatment is successful or not depends on the reproducibility of pink and white esthetics. Bone needs to remain stable to support the soft tissue.
The classic guideline for positioning an implant in IIPP procedure is the prof. Rojas-Vizcaya principle (3 mm apical and 2 mm buccal-principle, 3A-2B rule). According to this principle, the implant should be positioned 3 mm in the apical direction of the cervical contour of the planned crown to achieve appropriate biological width; and 2.0 mm in the palatal or lingual direction from the cervical contour to maintain 1.8-2.0 mm of buccal bone [22].
How to best use the 3A-2B rule? First, clinicians should determine the occlusal plane or incisal edge; and then, the cervical contour of the planned restoration should be confirmed; finally, surgeons should measure the distance between the cervical contour and the level of the remaining bone. Only in this way, can clinicians place an implant in an ideal 3D position and obtain a satisfactory restoration effect. In other words, the restoration design needs to be the first step in treatment planning. This is coincide with restoration-oriented implant placement concept.
We always use the 3A-2B rule as a guideline for immediate implant placement, especially in esthetic zone (Figure 2). Coron-apically, the implant shoulder should be placed 3 mm in the apical direction from the cervical contour. If the facial bone of the fresh extraction socket is less than 3 mm from the cervical contour, we will place the implant below the bone without any reduction of the bone. And if the distance is more than 3 mm, guided bone regeneration is recommended in the esthetic zone. Buccolingually, maintain a gap of at least 2 mm between the implant and the internal surface of the facial bone wall. Only in this way, can sufficient space be provided for the formation of a blood clot which can subsequently reorganized into a provisional connective tissue matrix and support the formation of newly formed woven bone. Additionally, this gap can also provide a space for an appropriate bone filler, such as TERUPLUG ® .
A facial mal position of the implant for immediate implant procedure is proved a common risk factor for mucosal recession. Hence surgical guide template can be applied if necessary in order to get an ideal implant location to ensure good available bone around.
Marked dimensional alterations with immediate implants was a common observation during the first 8 weeks post tooth extraction in different studies [7,27,34-36], in which a risk of 20-30% for mid-facial mucosal recession of more than 1 mm were reported. In those studies, the authors identified risk factors for mucosal recession, including a thin tissue bio-type, a facial mal position of the implant, and a thin or damaged facial bone wall at extraction. Among them, the thickness of the facial bone wall is extremely important. The deficiency of blood supply, which is derived from the loss of periodontal ligaments and the application of surgical trauma, result in alveolar bone resorption and labial bone plate reduction follow teeth extraction.
Some recent reports proved that the immediate implant placement into extraction socket with an intact buccal wall allows healing and osteointegration despite a large gap distance (2 mm or less) and without primary flap closure, a bone graft, or a barrier membrane [37], and the clinical outcome and degree of osteointegration does not differ from implants placed in healed, mature bone [1].
Nevertheless, Akimoto, et al. evaluated the effect of gap width on bone healing around implants placed into simulated extraction socket defects of varying widths (0 mm, 0.5 mm, 1.0 mm, 1.4 mm) in mongrel dogs. Histologically, as the gap widened, the amount of bone-to-implant contact decreased, and the point of the highest bone-to-implant contact shifted apically [38].
Additionally, as the conclusion in the review by Chen & Buser, bone augmentation procedures were effective in promoting bone fill and defect resolution for immediate implant placement [13]. Additionally, the esthetic outcomes were also favored by the development of esthetic indices, such as the Pink Esthetic Score and White Esthetic Score [39].
Actually, for clinicians, the main focus of treating the extraction socket is to preserve the tissue volume to a certain extent and improve the soft tissue conditions for implant placement. Since resorption of buccal bundle bone can pose a significant complication with very negative cosmetic impacts, how to compensate the resorption and remodeling of the buccal bone? The following procedures can be considered: a) Bone graft with regeneration materials; b) Connective tissue graft if necessary before, during , or after implant placement [23]; c) Flapless implant placement is recommended; d) At the anterior zone, immediate restoration is recommended if possible, yet for the posterior zone, wide healing abutment should be applied. Furthermore, when the buccal bundle bone is very thin, socket shield technique can also be applied to preserve the periodontal ligaments related perfusion [40,41]. Point c has been discussed above, we will discuss point A and B hereon and point d will be analyzed in detail later.
Based on scientific evidence, for both soft and hard tissue volume augmentation, autogenous grafts are considered to be the “gold standard”. However, major limitations and disadvantages associated with the use of autogenous grafts are variations in quality and quantity of tissue that is available for grafting and the harvesting procedure, patients often complain about pain and numbness especially in the donor site for several weeks post operation [42,43]. To overcome therefore mentioned issue of autogenous grafts, scholars have focused on the development of soft and hard tissue substitutes of various origins and for various clinical indications.
As to bone graft with regeneration materials, many scholars presented effective and practical solutions by practice. Daniel Buser suggested using Bio-Oss and Bio-Guide to achieve the goal [36], Dennis Tarnow advocated “dual zone augmentation technique” [44,45], Hom-Lay Wang proposed “sandwich bone graft” [46], while Toshiro Kodama put forward a concept called “Pile-Up technique”, that means apply TERUPLUG ® and TERUDERMIS together, all aiming at compensating for the resorption of the buccal bone.
The dual zone is divided into two regions: The soft tissue zone and the bone zone. The soft tissue zone is defined as the tissue coronal to the implant-abutment interface, while the bone zone is defined as the tissue apical to the interface. After tooth extraction and implant placement, the contour of the ridge will change, our goal is to minimize this contour change, only in this way, can we obtain a predictable esthetic treatment outcome [45].
Since 2018, our teams have attempted to apply TERUPLUG ® in immediate implant placement procedure, aiming at obtaining an excellent buccolingual volume that is coincident with the contour of the tooth either in the anterior region or in the posterior region.
In our experience, when the implant is placed to the palatal aspect of the fresh tooth extraction socket, a buccal residual gap distance of about 2 mm will be left there. Then, place a wide flat contoured healing abutment, and adapt a suitable size TERUPLUG ® into U-shape and insert it against the abutment into the gap at the facial and interproximal side, filling the bone and soft tissue zones, to reserve the space for peri-implant hard- and soft-tissue [45]. Make sure that the TERUPLUG ® occupies the soft tissue zone to the height of the free gingival margin (FGM) and keep it out of contact with the threads of the implants, only in this way can TERUPLUG ® act as a scaffold to support the ridge contour profile (Figure 3). At the anterior zone, immediate restoration can be considered, acting both as the prosthetic seal and as the biomaterial protection and supporter during initial healing.
In conventional implant, clinicians can choose submerged healing or unsubmerged healing according to the actual condition of the implant surgery. Submerged healing is a conservative approach, in which cover screw is placed to protect the screw channel access of the implant before suture, and a second stage surgery is needed for soft tissue remodeling after 3-6 months healing phase. For unsubmerged healing, clinicians can place a healing abutment or manufacture an immediate provisionalization in order to create an ideal soft tissue contour, avoiding a second surgical stage.
However, for immediate implant placement, IIPP have been considered an appropriate treatment procedure for maintaining the architecture of hard and soft tissue, as well as avoiding a second surgical stage.
De Rouck, et al. compared the soft tissue outline at immediate implants following immediate connection of a temporary crown and that following submerged healing during which a removable partial denture was used. They found that delayed restoration resulted in initial papilla loss take up to 1 year to attain comparable height as for immediate restoration [47]. Mid facial recession was systematically 2.5-3 times higher following delayed restoration pointing to a 0.75 mm additional loss compared to immediate restoration after 1 year. As a result, if the primary implant stability permits, immediate single-tooth implants should be instantly provisionalized in the interest of optimal mid facial esthetics [48].
We conclude that: (i) For immediate single-tooth implant with thick-gingival biotype and the primary implant stability higher than 35 N.cm or implant stability quotient (ISQ) above 70, implant-supported instant provisionalization is recommended in order to optimize esthetic treatment outcome. (ii) If the conditions do not permit, connective tissue graft is needed at the subsequent surgery if necessary. (iii) For delayed implant surgery, implant-supported immediate restoration makes little sense.
When the secondary implant stability is obtained after 3-6 months healing period, the provisionalization is removed, and the matured soft tissue contour is presented, a provisional prosthesis copying the maintained emergence profile is placed and then the final contour is transferred with a custom impression transfer technique. Finally we can obtain a restoration simulating the natural tooth emergence, thus guaranteeing more predictable results and simplifying the next stages of treatment (Figure 5).
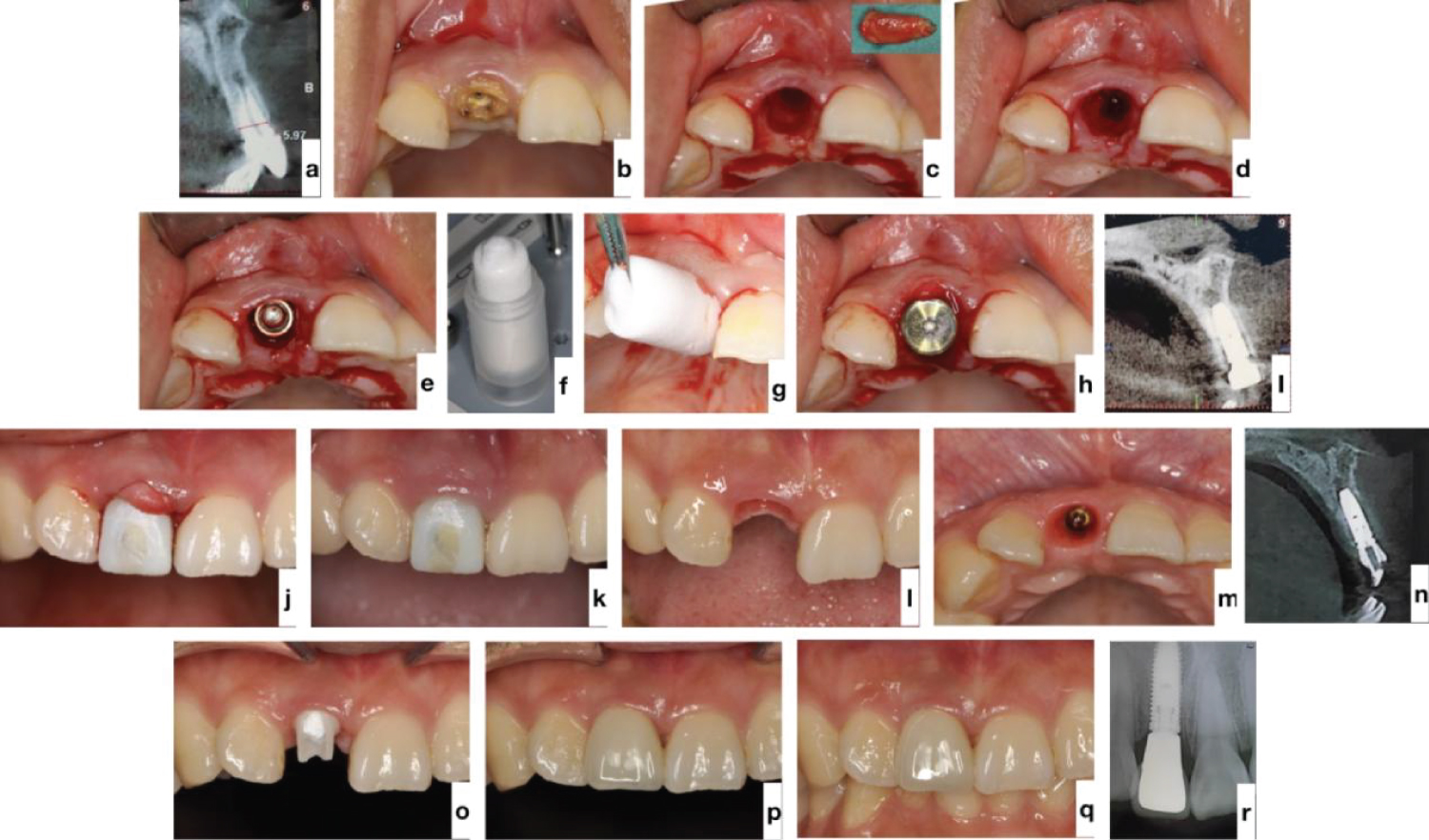 Figure 5:
View Figure 5
Figure 5:
View Figure 5
Although IIPP procedure is recommended in esthetic zone, immediate prosthesis is not a common procedure in the posterior zone, as aesthetics is not that important and the masticatory forces are capable of preventing osteointegration of the implant during the healing period.
As the growing demand of the patients for less invasive procedures, healing abutment is considered most of the time if the situation permits in the posterior scenarios. Although the diameter and height of the prefabricated standard healing abutment of different implant systems vary widely, their morphology have little difference-most of them have a circular cross-section. The round cross-section allows it to be suitable to the implant in any position, and can prevent food impaction, eliminate the need for a second reopening surgery.
However, as the shape of the tooth, the morphology of the alveolar ridge and the quality and quantity of keratinized gingiva differ in thousands of ways, wide healing abutments are recommended because they can protect and contain the bone substitute during healing, preserving the alveolar and the gingival contours for provisional restorations. But most standard healing abutments are not wide enough.
An ideal healing abutment should have the three-dimensional shape of the reconstructed tooth, which is called the emergence profile. As a result, if wide healing abutment is not available, we can manufacture customized healing abutment made of polyether-ether-ketone (PEEK) or zirconium for this purpose [49,50].
Sanz-Esporrin, et al. evaluated the rate of bone loss progression during experimentally-induced peri-implantitis using two different implant-abutment connections [51]. Finally they found that a platform switching connection resulted in a more benign development of peri-implantitis in the peri-implantitis induction phase. However, once the ligatures were removed, these differences disappeared. Consequently, platform switching abutment is recommended.
In conclusion, for immediate implant placement in the posterior zone, we should apply a healing abutment as wide as possible, customizable healing abutment is also preferred. And the best healing abutment to be considered should be those with funnel-shaped contact area with the shoulder of the implant, and with columnar superstructure (Figure 6).
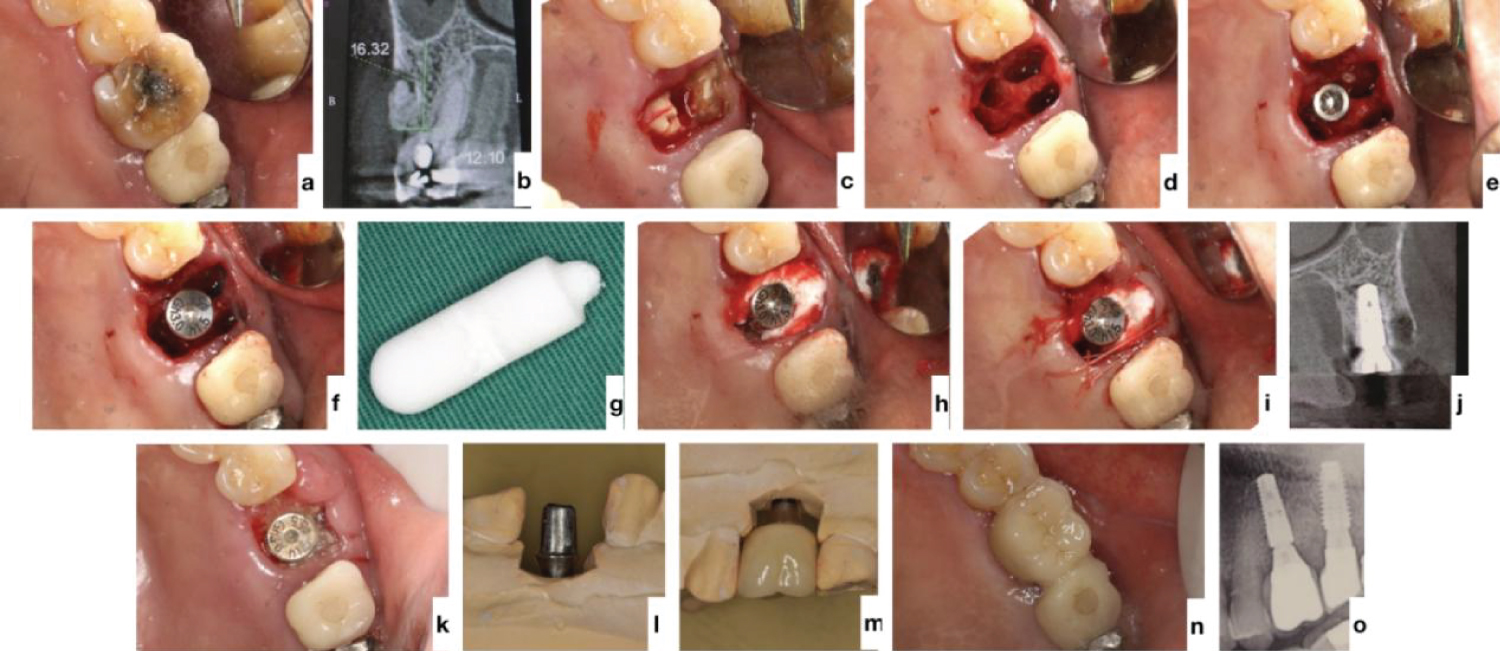 Figure 6:
View Figure 6
Figure 6:
View Figure 6
The 7 essential elements for successful hard- and soft-tissue regeneration in immediate implants with TERUPLUG ® are intended to be a guide for clinicians and aid them in making treatment plan and in concrete clinical application of TERUPLUG ® . Each element can be critical in achieving the final, predictable long-term outcome. Treatment for immediate implant placement at the time of extraction is a complex procedure for clinicians.
Short- and medium-term studies now show equivalent results between immediate placement and provisionalization with TERUPLUG ® compared with those with other low-substitution mineralized bone materials when the 7 essential elements are followed. Long-term studies are needed because contour changes of the soft- and hard-tissues may continue for many years post-implant placement.
Our group also investigated the changes of alveolar bone 5 months after immediate implantation with TERUPLUG ® in the posterior area. 45 patients attended in our hospital from July 2019 to October 2021 and met the indications for immediate posterior tooth implantations were selected. All patients underwent immediately implant placement following these 7 essential elements mentioned above TERUPLUG ® was placed between the shoulder of the implant and the keratinized gingiva. Immediately after surgical intervention, a CBCT was taken. Five months after the surgery, a second CBCT was taken and marginal bone loss (MBL) was calculated on CBCT to evaluate the reconstruction of alveolar bone around the implant [52], and to evaluate the implant retention rate and postoperative complications. During the 5-month-follow-up period, the mean bone resorption of proximal and distal alveolar bone was (-0.487 ± 1.093) mm and (-0.935 ± 2.452) mm. No implant loss or loosening occurred in all 45 patients (the retention rate was 100%), and no other complications occurred in all patients. Thus we conclude that after 5 months of immediate implants with TERUPLUG ® in the posterior dental region, the mesial and distal alveolar bone increased to a certain degree, suggesting that TERUPLUG ® has a positive effect on promoting osteogenesis after immediate implantation in the posterior dental region.
Long-term studies are needed to investigate the changes of alveolar bone after immediate implantation with TERUPLUG ® both in the anterior and in the posterior area.
The authors reported no conflicts of interest related to this study.