Acute Kidney Injury (AKI) is a Health problem that occurs with considerable frequency in our environment, often affecting people in an age range in which they are economically active or start the formation of a family. There are no records of the incidence of this condition in our environment, as well as no record of the impact on people of working age.
To establish the incidence of AKI, determine the Incidence of the Economically active population that develops AKI, as well as to identify the main diagnoses that lead to AKI in previously healthy young adults who are admitted to the emergency observation service of the General Hospital of Zone Number 50 of the IMSS.
We carried out an observational, descriptive, analytical, cross-sectional, prospective study in patients of the Emergency Service of the HGZ 50 of the IMSS San Luis Potosí between 18 and 45-years-old previously healthy, from January 1 to December 31, 2019.
We included a total of 3714 patients who met the inclusion criteria, 1609 female and 2105 male, 3089 are economically active and 625 are not. Of the 3714 patients, 73 presented AKI, with an incidence rate of 19.6 cases per thousand patients. Of the patients who presented AKI, 20 were female and 53 were male. Of the 73 patients who presented AKI, 55 were economically active. We found that urinary tract obstruction is the most frequent associated factor, followed by other diagnoses presented in frequently that collectively obtain second place as the cause of it, in third place are patients with trauma and hipovolemia.
AKI is a pathology that occurs frequently in our environment, expected in a certain group of patients and put a side in some others. The purpose of this study was to establish the incidence of AKI in an age group in which we assume it is not frequent to find it within the emergency department, so that, on occasions, it is not taken into account or the necessary measures are not taken for its management, alerting the medical staff not to underestimate the presentation of this entity in young patients, especially in those with urinary obstructive pathologies.
Incidence, Acute Kidney Injury, Economically Active, Young Adult
ADQI: Acute Dialysis Quality Initiative; AKI: Acute Kidney Injury; AKIN: Acute Kidney Injury Network; ATP: Adenosine Triphosphate; IMSS: Instituto Mexicano del Seguro Social; RIFLE: Risk, Injury, Failure, Loss, End-stage kidney disease
Acute kidney injury (AKI) is and will continue to be one of the most important causes of admission and death in intensive care units and nephrology services in our country, afflicting 1 to 25% of patients in the aforementioned services, a fact that motivates Dr. Aristondo, et al., to carry out a meta-analysis with literature from 1965 and 1980, reporting sepsis and shock as the main causes of AKI. Obtaining a mortality of 16 to 18.7% when the kidney injury was treated as the only failure, but in the presence of multiple organ failure syndrome it rose to 46.7%.
Mortality from AKI is unacceptably high. It is possible that even a mild episode of AKI can lead to permanent organ failure in the long term and greater morbidity and mortality in those who suffer from it. Therefore, this pathology must be prevented, adequately cared for and never ignored even in its mild presentations [1].
At the General Hospital of Zona 50 of the IMSS in San Luis Potosí, there is no real registry of patients who develop this pathology, which is why a study was carried out in which the underdiagnosis of AKI in the service of emergencies [2]. Knowing the current incidence of AKI in our environment, as well as the most frequent causes that trigger it, will allow the emergency physician to be alerted to this diagnosis, which, if ignored, can have consequences ranging from sequelae to death, with high social and economic impact, especially since they are young adult patients.
According to data from the General Directorate of Health Information, in 2015 there were 655,689 deaths in the country, of which 2,021 cases were attributable to some type of AKI, of which 1,046 cases corresponded to men and 975 to women, 210 in the age group from 21 to 50 years. In the State of San Luis Potosí, 14,181 deaths are reported, of which 37 correspond to some type of AKI, 19 occurred in men and 19 in women, of which only 4 correspond to an age group under 60 years [3].
We carried out an observational, descriptive, analytical, cross-sectional, prospective study in patients of the Emergency Service of the HGZ 50 of the IMSS San Luis Potosí between 18 and 45 years previously healthy, without pharmacological treatments for at least the last week, who agreed to participate through the signing of an informed consent or with determination of creatinine upon admission to the emergency room. It was carried out from January 1 to December 31, 2019. Taking as a case of AKI the patients who presented creatinine with 0.3 mg/dL above the normal high limit level of the HGZ 50 laboratory (1.2 mg/dL).
The data collected will be integrated into an Excel spreadsheet for coding the variables, and will be analyzed using the IMB SPSS Statistics 24 statistical package in Spanish, using measures of central tendency for descriptive analysis.
The analysis of patients admitted for observation at the emergency service of the HGZ 50 of San Luis Potosí during the period from January 1 to December 31, 2019, including a total of 3714 patients who met the inclusion criteria, of which 1609 are female and 2105 male, as can be seen in (Graph 1).
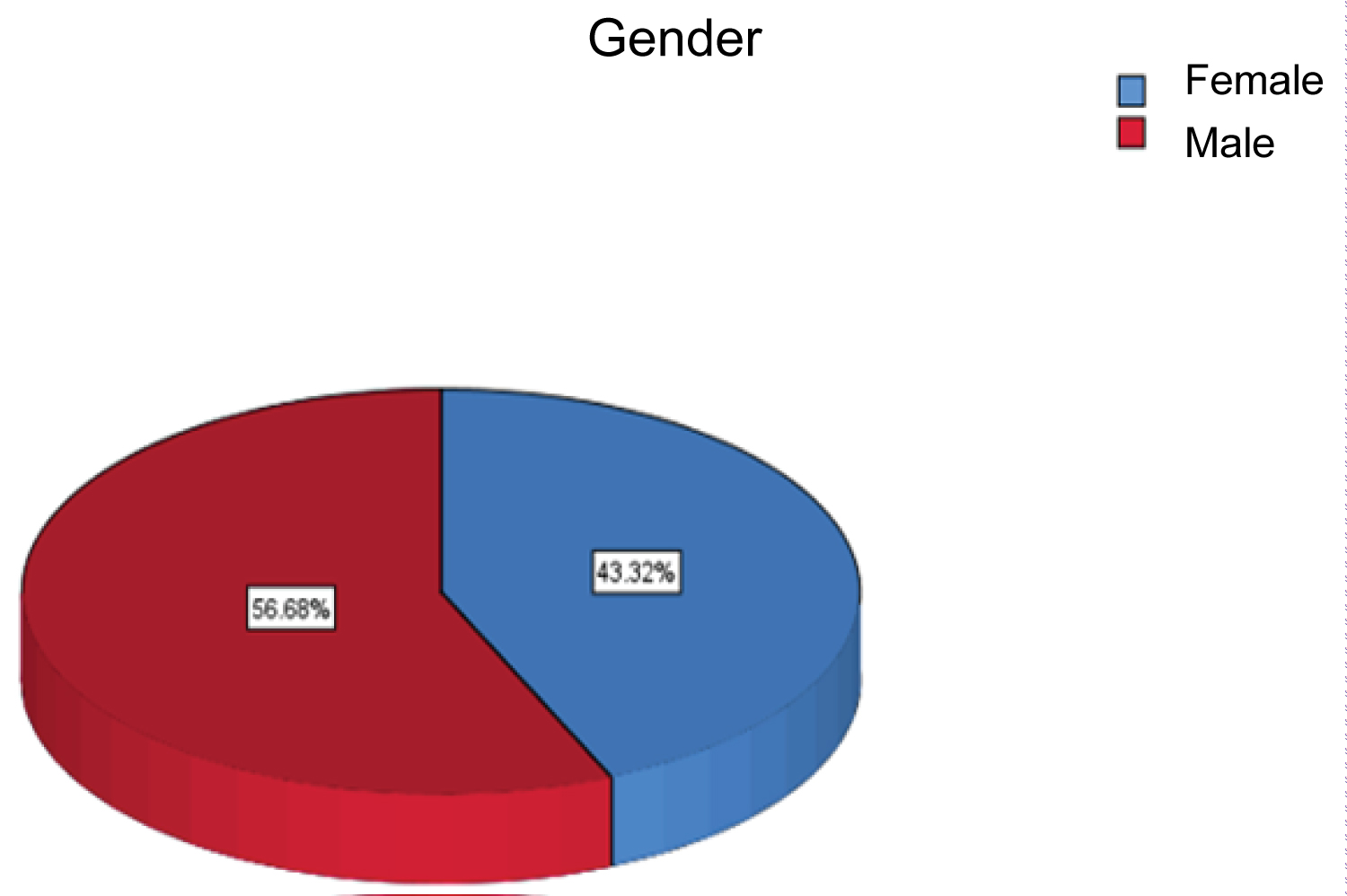 Graph 1: Percentage by gender.
View Graph 1
Graph 1: Percentage by gender.
View Graph 1
Of the 3714 patients, 73 presented AKI, with an incidence rate of 19.6 cases per thousand patients (Graph 2) shows the percentage of patients with AKI.
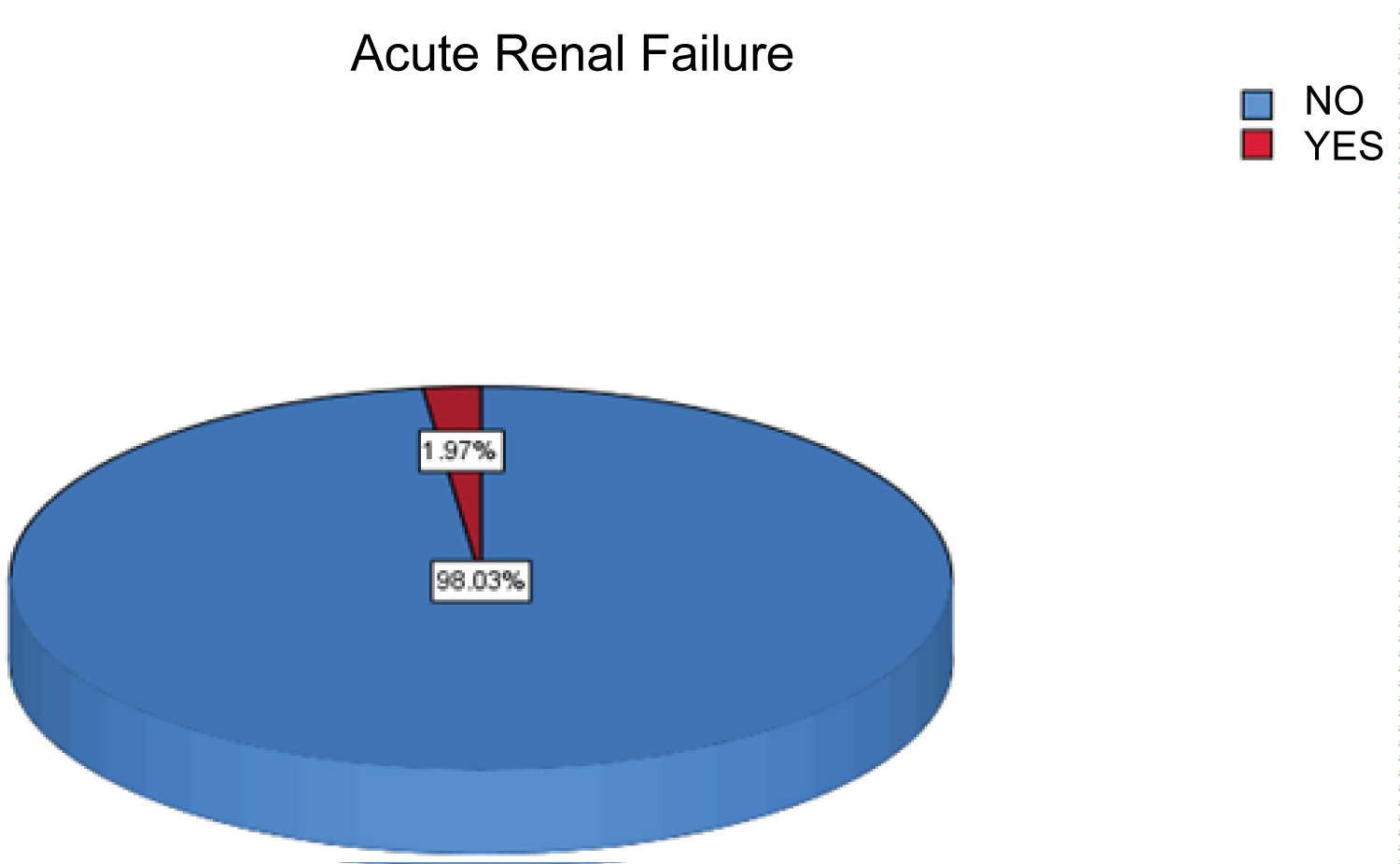 Graph 2: Percentage of patients who presented AKI in one year.
View Graph 2
Graph 2: Percentage of patients who presented AKI in one year.
View Graph 2
Of the 3714 patients included in the study, 3089 are economically active and 625 are not, as shown in (Graph 3) in percentage.
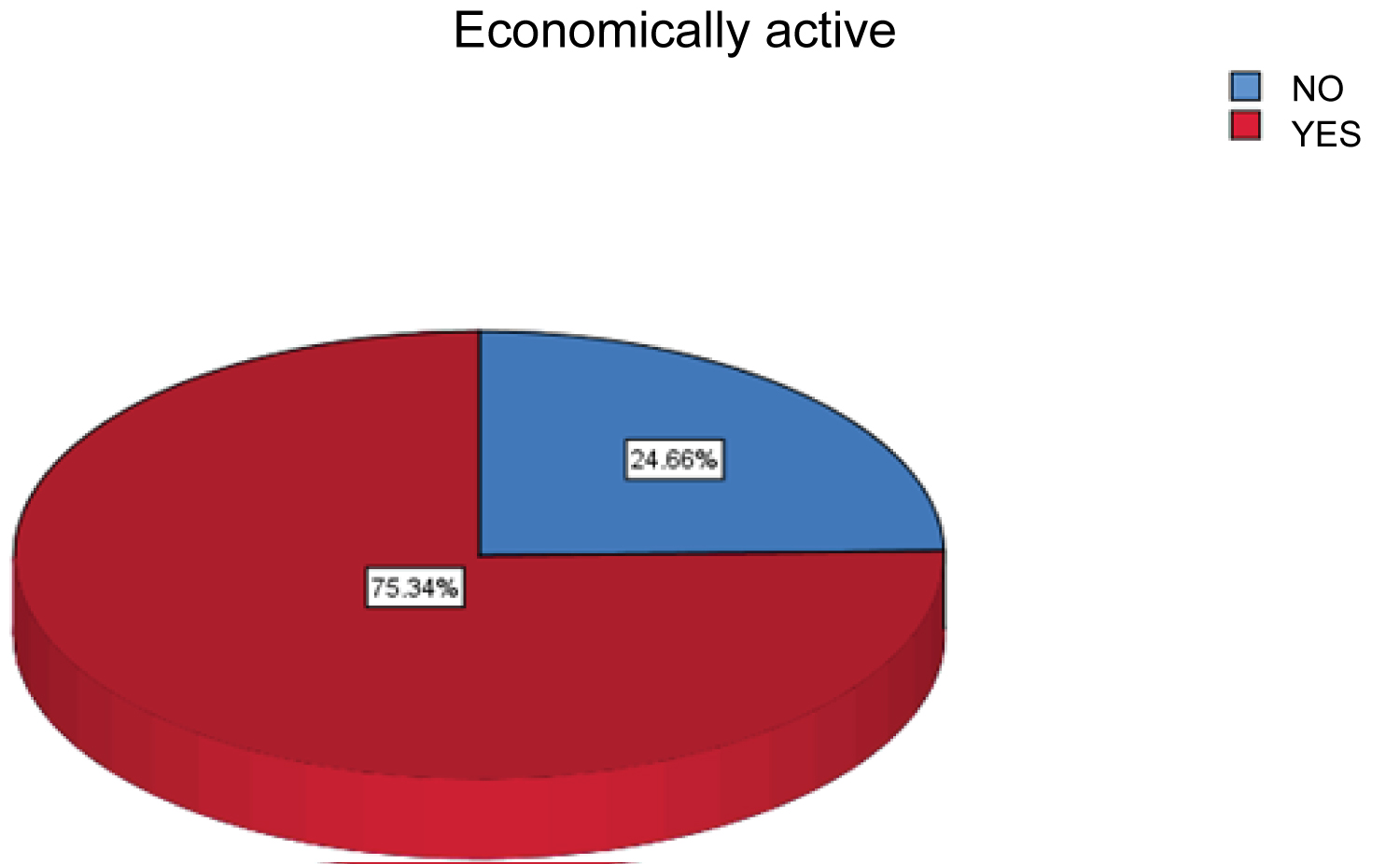 Graph 3: Percentage of economically active patients.
View Graph 3
Graph 3: Percentage of economically active patients.
View Graph 3
Of the 73 patients who presented AKI, 20 were female and 53 male, as shown in (Graph 4).
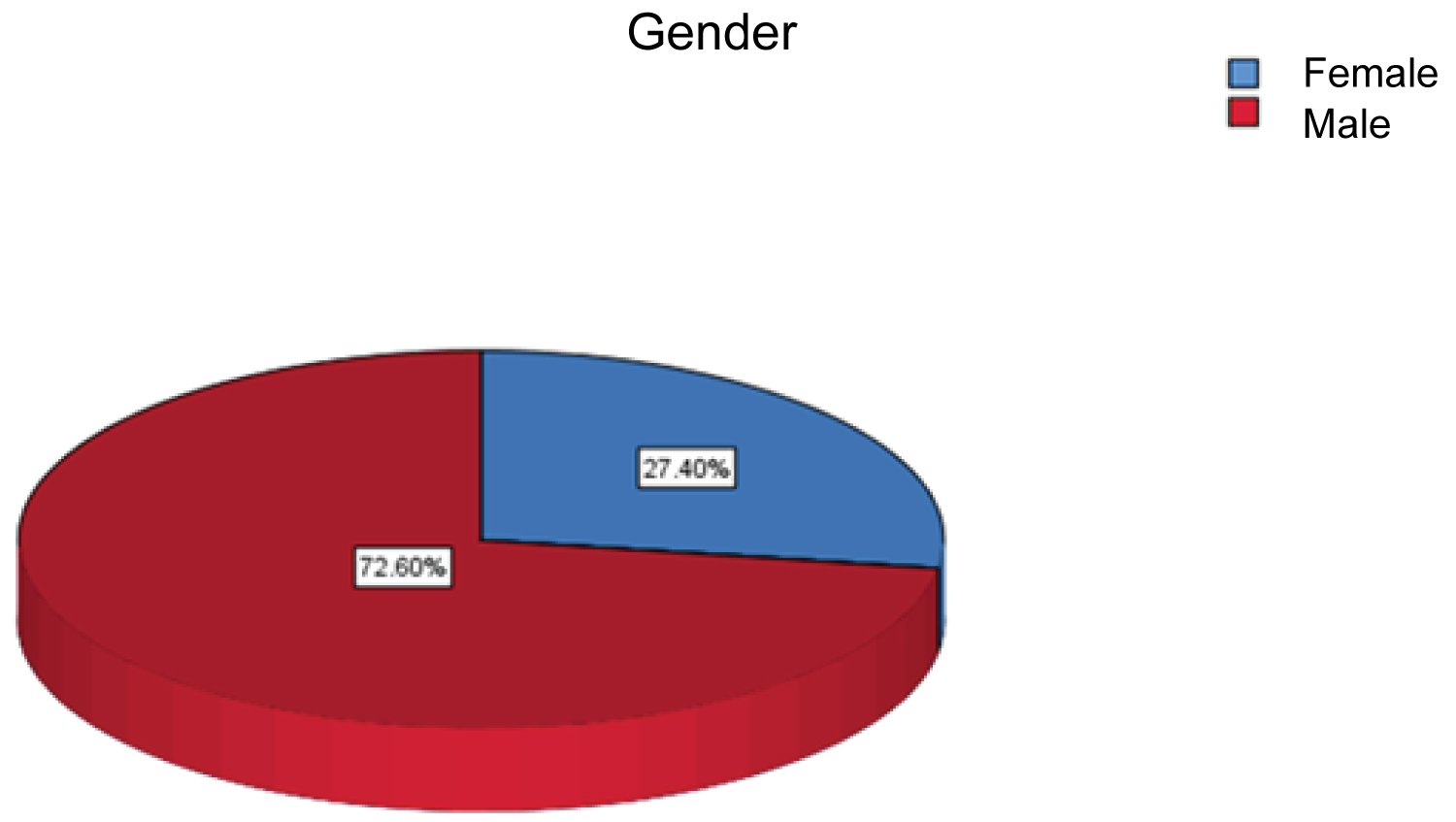 Graph 4: Percentage by gender of patients with AKI.
View Graph 4
Graph 4: Percentage by gender of patients with AKI.
View Graph 4
Regarding the factors associated with Acute Kidney Injury, it was found that urinary tract obstruction is the most frequent associated factor, followed by other diagnoses presented infrequently that together obtain second place as the cause of it, in third place Patients with trauma and hypovolemia are found as subsequent causes in frequency as observed in (Table 1).
Table 1: Percentage of frequency of risk factors. View Table 1
Regarding the patients who developed AKI, an average age of 31.6 years was found, with a median of 30 years, a mode of 27 years, and a range of 27 years, with an age distribution by percentages as shown in the (Graph 5).
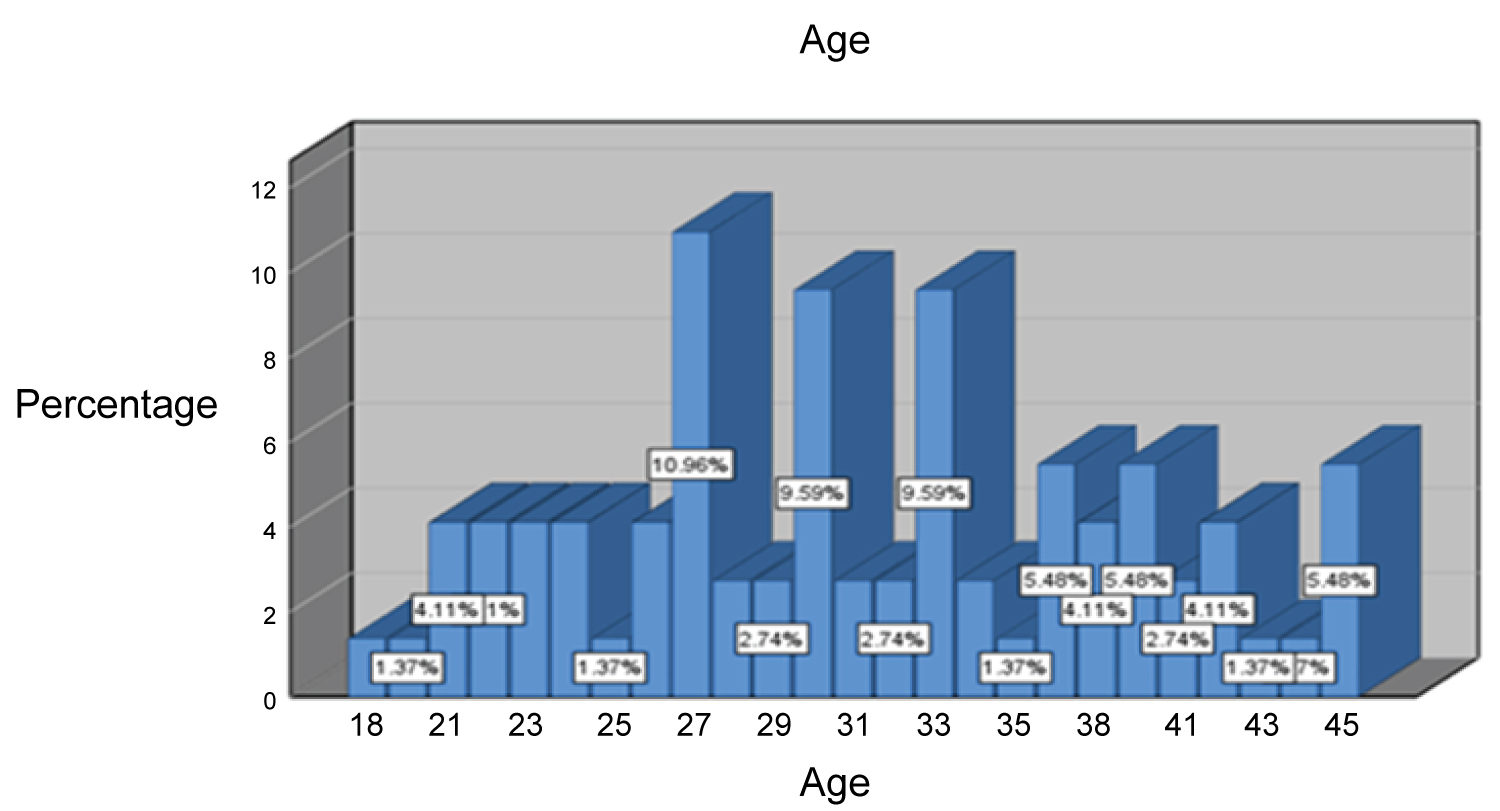 Graph 5: Age percentage in patients with AKI.
View Graph 5
Graph 5: Age percentage in patients with AKI.
View Graph 5
Of the patients who presented AKI, 55 were economically active and 18 were not economically active, as shown in (Graph 6).
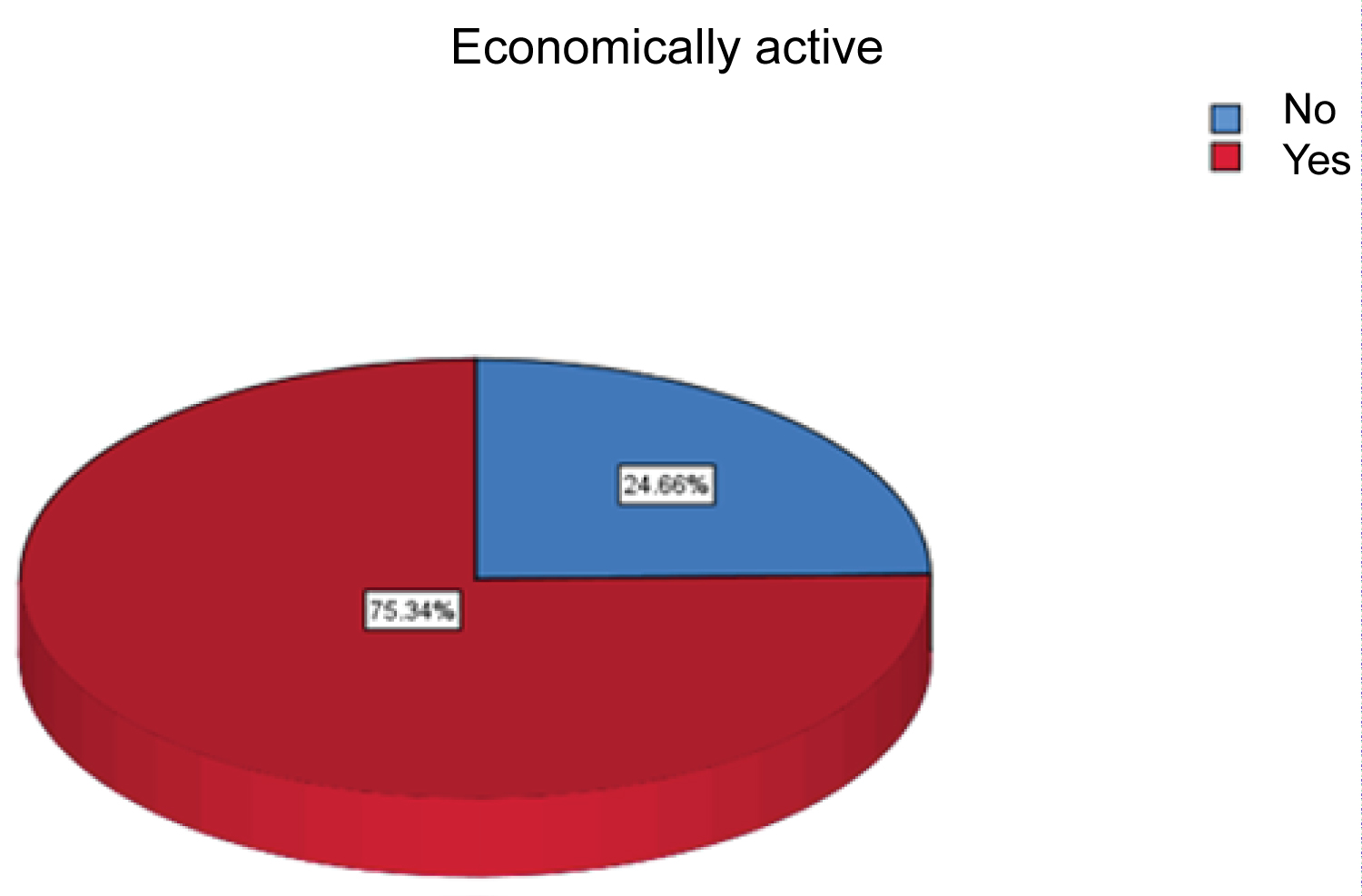 Graph 6: Percentage of economically active patients with AKI.
View Graph 6
Graph 6: Percentage of economically active patients with AKI.
View Graph 6
The objective of our study was to establish the incidence of AKI and associated factors in previously healthy young adults who were admitted to the Emergency Observation Service of the General Hospital of Zone 50 of the IMSS.
AKI is a pathology that occurs secondarily in several conditions that afflict patients treated in the emergency services, which, if not diagnosed and treated effectively and in a timely manner, can bring catastrophic complications for the health of the people who suffer it ,because it significantly alters the lives of patients not only in the personal and family aspects, but also in the economic one, in addition, it translates into a high cost to treat the complications that it generates and in many occasions it prevents those who suffers from activities that pay him, altering his way of life in all aspects. Little information is available in medical publications about AKI in young people as well as in previously healthy people who develop it due to accidental illnesses.
In our study, which included a total of 3714 subjects, we found an incidence of AKI in previously healthy young adult patients of 19.6 per 1000 patients.
Chávez and Sánchez in 2010 with the RIFLE classification diagnosed 4,888 patients with AKI, in a study called Natural history of acute renal failure (ARF) in Mexican Intensive Care Units, which was descriptive, comparative, observational, longitudinal, multicenter, inter-institutional, with cohort directionality and with prolective collection of information on patients admitted to hospital in a period of 6 years in the intensive care units that participated in the study considering inclusion criteria: Age 15 years or older, any gender, with stay in the intensive care unit of 24 hours or more, in whom baseline creatinine had been recorded upon admission.The incidence rates for AKI were 138 episodes per 1,000 patients [4].
In 2015, San Juan Martín and Collaborators found a prospective cohort study that included patients with a diagnosis of trauma who were admitted to the Intensive Care Unit in which 41 patients were studied where acute kidney injury was observed in the study group. 20 patients, although it was not specified in the study whether the patients were healthy prior to the trauma event [5].
Ortuno-Andériz, et al. Found in 2014 in a prospective series of 50 patients admitted to an intensive care unit with septic shock and plasma creatinine < 2 mg/dl with clinical follow-up that 20 patients (40% of the sample) developed AKI, based on in determinations of cystatin C urea and creatinine [6].
Piccinni, et al. Found in 2011 in Italy, in a prospective, observational and multicenter study that included 576 patients admitted to 10 intensive care units with a mean age of 66 years, of which 246 patients, 42.7% presented AKI in the In the first 24 hours of their stay, some of these patients had comorbidities such as hypertension and diabetes mellitus [7].
The aforementioned authors, although they report incidences of the development of AKI, do not take into account only young patients and describe the development of AKI in certain groups as well as in intensive care; In our study, a lower incidence was found than what was stated by the authors; however, the detection of AKI from the emergency room, as was our study, has not been studied in the published literature, which highlights the importance of this protocol. Just as no literature was found that took into account only young patients.
With regard to factors associated with the appearance of AKI in the patients in our study, we found urinary tract obstruction as the main cause, followed in second place by a set of conditions that occur in a lesser proportion that are not included in a category because it occurs on rare occasions, thirdly traumatic causes and fourth hypovolemia.
Carpio-Deheza, et al. Found in 2010, through a Descriptive, Retrospective and Cross-sectional study carried out in the Internal Medicine service of a Hospital in Bolivia, that of a total of 36 patients who presented AKI in terms of the triggering cause of AKI, observed: 1st place: 41.67%, Hypovolemia. 2nd place: 30.56%, arterial hypertension. 3rd place: 11.11%, Heart failure [8].
Lluncor, et al. Found in 2013 a case-control study in which 50 cases and 100 controls of incident patients were included in an emergency at a III-B hospital in Lima. The risk factors found were the severity of the patient, the presence of an infectious condition as a diagnosis on admission, the existence of sepsis and being in septic shock [9].
Durán, et al. Found in 2000 in a case-control study carried out in an intensive care unit in a hospital in Mérida, Yucatán, that male gender and the severity of the disease were the most important risk factors for the disease. Development of ARF in this study [10].
Regarding risk factors, the aforementioned literature reports hypovolemia and infections that led the participants to states of shock, it is even commented that studies that the severity of the disease and gender become risk factors, which contrasts with the A result of our study where we found urinary tract obstruction as the main cause of AKI followed by trauma, probably because our interest group was young and previously healthy patients.
Carpio-Deheza, et al. Report in their 2010 study that of a total of 36 patients who presented AKI in terms of age groups, the largest number was found between 60-69 years, with 25% (9 patients) in second, the group formed between 40-49 years with 19.44% (7 patients) and thirdly, the groups formed between 15-19 years and 50-59 years, both with 13.89% (5 patients) each [8].
In their 2015 study, San Juan Martín and Collaborators found the mean age of the patients of 35.4 years with a range of 15 to 67, where AKI was found in 20 patients [5].
Ramírez and collaborators found in 2019 in a retrospective, cross-sectional and analytical study, carried out in the emergency service of the HGZ 24 Poza Rica, Veracruz; In patients over 18 years of age who presented a diagnosis of sepsis, 18% of the patients who presented AKI were between 36 and 58 years of age [11].
Durán, et al. Found in their study in 2000 within the population studied that the average age of the cases was 43 ± 19.5 years [10].
Regarding age, in our study we found a peak of incidence between 27 and 33 years, the literature reports age groups older than those found in our study, probably due to the characteristics of the population studied, since, in the The commented studies took patients with comorbidities such as chronic degenerative diseases and were not focused on a healthy or young population.
Carpio-Deheza, et al. Found in their 2010 study that of a total of 36 patients who presented AKI in terms of sex, 58.34% were men (21 patients) and 41.66% were women (15 patients) [8].
Ramírez, et al. Found in their 2019 study that 60% of the patients who presented AKI corresponded to the male gender and gender is described as a risk factor for presenting AKI [11].
Durán, et al. Found in their study of the year 2000 that within the population studied, 22% were male cases against 5% female. By performing Fisher's exact test, they determined that the female gender is a "protector" against AKI [10].
Regarding gender, our study showed a predominance in male patients, similar to that found in most of the literature that reports a higher frequency of patients of this gender in any age group and even in the case of young or old patients with or no chronic history.
Regarding whether the patients are economically active, no bibliography was found in which the implication of this variable was studied in the context of a cute kidney disease, so we limit ourselves to stating the result of our study that shows that regardless of gender and within the age range included in the study, most of the patients with AKI are economically active.
Hurtado, et al. Found in 2004 in a retrospective and analytical study that the causes of AKI were: Hypoperfusion 52.3%, preeclampsia 17%, and nephrotoxic 9.4% [12].
Chávez Pérez, et al. Found in their study that the most common etiologies were multiple organ dysfunction syndrome in 1,676 cases (34.4%), ischemia in 1,496 (30.7%), two or more simultaneous etiologies in 1,394 (28.6%), nephrotoxicity in 175 (3.6%) and uncertain at 147 (3.0%) [4].
Lluncor, et al. In their 2013 study report that the presence of an infectious condition as a diagnosis on admission, sepsis, and the state of septic shock were conditioning factors for AKI [9].
The most frequent diagnoses found in our study refer to obstructive urinary tract pathology, represented by urinary tract lithiasis followed by traumatic pathology, in contrast to what is found in the literature where it is mentioned that hypoperfusion (state of shock), Multiple organ dysfunction syndrome and sepsis are the diagnoses most found in the studies consulted, probably due to the characteristics of the groups studied, since older patients were taken as well as those with pre-existing comorbidities.
To the nursing staff of the General Hospital of Zone Number 50 of the Mexican Institute of Social Security of San Luis Potosí, for their support in the collection of patient data for this protocol as well as for the undergraduate interns who rotated in the service emergency departments of the same hospital in the data collection period.