The humble chest X ray (CXR) is an important factor in the assessment of the patient with traumatic injury. The Advanced Trauma Life Support (ATLS) programme [1] recommends performing a CXR as part of the secondary survey, and this is widely used in Singapore. All general hospitals that receive trauma patients in Singapore have resuscitation bays capable of rapidly obtaining a CXR film using either a fixed radiology machine or a portable machine kept within the Emergency Department itself.
A CXR is capable of accurately allowing diagnosis of a wide range of traumatic injuries in the chest, ranging from bony (rib, scapular or clavicular fractures) to pulmonary contusions or haemo-pneumothoraces [2]. Other subtler signs of underlying injuries such as subcutaneous emphysema, mediastinal emphysema and aortic injuries may be detected depending on the quality of the film and the experience of the reading physician. While the diagnostic yield of rib, lung and pleural injuries has been previously described [2], the role of chest X ray in identifying patients with mediastinal injuries is less clear. In an era of increasing resource constraints, it would be helpful to know how a widened mediastinum seen on CXR correlates to great vessel injuries so that unnecessary CT thorax scans can be safely avoided.
We aimed to compare the rate of detection of mediastinal injuries using widened mediastinum on CXR and eventual findings on CT thorax by means of a retrospective review of the imaging results and radiologists' reports of all trauma patients captured in our electronic health records system.
A database search was performed on our hospital trauma registry to retrieve all patients with a diagnosis associated with trauma who received a CT thorax, and their unique National Registration Identification Card number was recorded. Their electronic health records were then extracted; the radiologist's report was then compared for both the initial CXR as well as the CT thorax. Statistical analysis was carried out by Microsoft Excel 2010 Ver 14.0. As this was a retrospective database study, no informed consent was deemed necessary from the included patients.
A total of 710 patients' records were retrieved from our trauma database. Of these, a total of 66 patients were excluded from analysis, 22 patients due to inappropriate diagnosis and 44 patients due to missing radiological data. The demographic data of the remaining 644 patients is shown in Table 1. The majority were males (77.6%), and their ethnic distribution was roughly similar to that of Singapore's general population with Chinese forming the majority (423 patients), followed by Malays (91 patients), Indians (84 patients) and Others (7%) as shown in Figure 1.
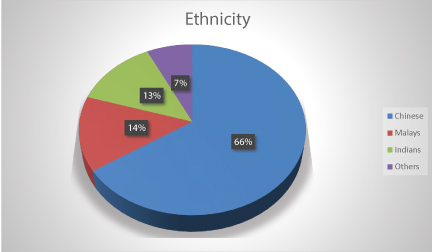 Figure 1: Breakdown of patient cohort by ethnicity. View Figure 1
Figure 1: Breakdown of patient cohort by ethnicity. View Figure 1
Table 1: Overall demographics. View Table 1
Almost all the patients (96.1%) had a blunt mechanism of injury, and the most common cause was road traffic accident - 56.8% (see Figure 2) followed by falls (34.6%). The median Injury Severity Score (ISS) of the cohort was 17, and the Revised Trauma Score (RTS) was 7.841 with a Probability of Survival (PS) of 96.8%. A total of 74 patients (11.4%) from the overall group of patients had demised at the time of data collection, of whom 30 patients (4.5%) had a recorded cause of death directly related to trauma.
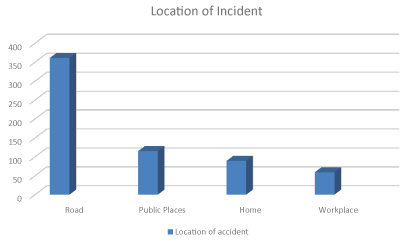 Figure 2: Breakdown of location where incident leading to injury occurred. View Figure 2
Figure 2: Breakdown of location where incident leading to injury occurred. View Figure 2
A total of 52 patients (8.1%) had positive mediastinal findings suggesting injury on CT thorax. 42 of these patients (80.8%) did not demonstrate any signs of a mediastinal injury on CXR while only 10 patients (19.2%) had a correlating widened mediastinum noted. Another 14 patients who had widened mediastinum reported on their CXR had no signs of mediastinal injury on CT thorax, of which 6 of these patients had other non-mediastinal injuries on CT thorax. There was therefore an overall sensitivity of 19.2% and specificity of 97.6% for detection of mediastinal injuries on CXR. 8 patients had widened mediastinum reported on their CXR but did not have any signs of mediastinal injury on CT thorax.
Out of 433 patients with non-mediastinal injuries on CT thorax, 130 patients (30.0%) had a normal CXR. The sensitivity of detecting a non-mediastinal injury on CXR was 70.0% while the specificity was 90.0%.
The multiply injured patient poses a significant diagnostic and management dilemma as available history is limited and physical examination may be compromised by distractions such as other injuries or stress from deteriorating patient vital signs. This can result in missed or delayed diagnosis of injuries. To a large extent, this is mitigated by protocols such as the American College of Surgeons ATLS [1]. This is widely used in our hospital by both ED physicians and the general surgical trauma team in our hospital; we therefore set out to explore if this leads to missed injuries or unnecessary imaging due to mediastinal widening seen on CXR.
The use of helical CT imaging has allowed the detection of mediastinal injuries accurately without having to subject patients to invasive aortography [3]. Given the differences in trauma population globally due to cultural, political and geographic factors; as well as different economics within each healthcare system, there is no global consensus on the use of computed tomography in trauma patients. The Eastern Association for Surgery in Trauma (EAST) guideline [4] strongly recommends the use of CT thorax with intravenous contrast when there is any concern of blunt thoracic aortic injury. We therefore used CT thorax findings as the gold standard to assess for presence of mediastinal injury in our study.
Our findings are similar to the published literature on the sensitivity and specificity of CXR in detection of mediastinal injuries. Both Agladioglu [5] and Traub [6] looked at the role of CXR in evaluation of patients with blunt traumatic injuries and found a sensitivity of 11.8% and 8.5% respectively. Both these studies also reported a significant number of patients with thoracic injuries seen on CT thorax that were not detected on CXR. Our data appears to concur with their conclusions that CT thorax is superior to CXR in the detection of thoracic injuries and should be strongly considered if there is any suspicion of such injuries due to history, physical examination findings (such as reduced air entry, chest wall tenderness or abnormal respiratory effort).
While CT is a rapid, accurate modality of imaging, profligate use of CT scans can lead to increased healthcare costs, delays in treatment and over-diagnosis of clinically insignificant lesions. CT scans also carry the risk of renal impairment from iodinated contrast (which may be exacerbated by other risk factors of renal injury resulting from trauma such as hypovolaemia and renal parenchymal injury). The American College of Surgeons thus listed avoidance of whole-body trauma CT as one of its five Choosing Wisely recommendations in 2014. A large multicenter randomized controlled trial [7] looked at over 11000 patients to compare the detection rate of injuries on CT versus CXR and developed a tool to assist in the decision-making process. This instrument (shown in Figure 3) resulted in more than 25% of patients being spared an unnecessary CT scan.
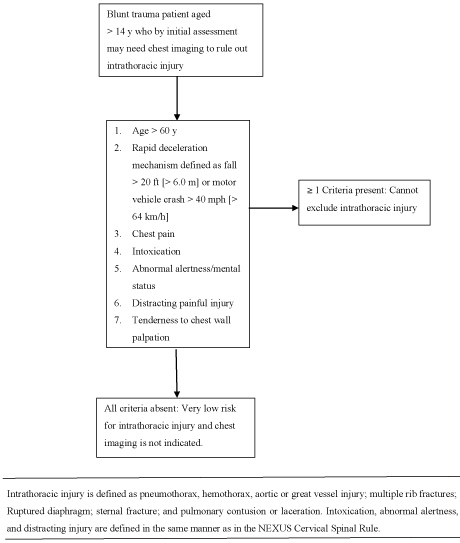 Figure 3: NEXUS chest decision instrument. View Figure 3
Figure 3: NEXUS chest decision instrument. View Figure 3
CXR still plays a major role in detecting other thoracic injuries. Previous authors [3-5] have found that CXR still has good sensitivity in diagnosing clavicle fractures, rib fractures and lung injury such as contusion and haemo- or pneumothoraces. CXR also has excellent specificity (exceeding 98%) and remains a fast, safe investigation that is available in many trauma resuscitation bays. It also allows for comparison with serial films in the case of indeterminate findings.
This study is one of the largest available series that focuses on comparing of detection of mediastinal injuries between CXR and CT thorax. The main limitation of our study is its retrospective nature and inability to comment on the clinical significance of the missed mediastinal injuries on CXR and whether they resulted in significant delays in treatment. This should be borne in mind when drawing conclusions from this data.
This large retrospective comparison of CXR to CT thorax findings in our trauma patients found that mediastinal injury was a rare entity that did not commonly manifest as widened mediastinum on CXR. There were also some patients who appeared to have widened mediastinum on CXR but did not have any injuries seen on CT thorax. We therefore recommend that while CXR has an invaluable role in the detection of bony or pulmonary injuries, widened mediastinum does not appear to play a major role in the decision process of whether a CT thorax is necessary. Other factors such as the mechanism of injury, presence of chest wall tenderness or abnormal respiratory function may be considered instead [7]. As such, widened mediastinum on CXR may soon become a relic of the past.
All the authors (Sunder Balasubramaniam, Chen Yanlin Rachel, Deng Tianshu and Teo Li Tserng) declare that they have no conflict of interest in this study.