A computed tomography scan of the chest in an 83-year-old male patient with a history of metastatic squamous cell lung cancer revealed a mass localized to the left ventricle. Subsequent imaging revealed this to be an incidental cardiac fibroma.
Echocardiographic, computed tomography and cardiac magnetic resonance images and a review of the literature is presented.
Primary Cardiac tumors are extremely rare. Cardiac fibromas are neoplasms of fibroblasts found within the myocardium [1]. More common in children than adults [2], the clinical presentation of these benign tumors can vary and range from completely asymptomatic to heart failure and significant life-threatening arrhythmias [3]. In this case report, we describe an octogenarian male patient suffering from multiple comorbidities in which a 3 cm fibroma of the anterolateral free left ventricular wall was discovered incidentally on computed tomography (CT) scan of chest.
An 83-year-old white male presenting with a past medical history of Type 2 diabetes mellitus, mixed hyperlipidemia, metastatic squamous cell carcinoma of the left lung, pulmonary emphysema, chronic obstructive pulmonary disease, paroxysmal atrial fibrillation, hypertensive heart disease with compensated NYHA Class 2 chronic diastolic congestive heart failure, coronary artery disease and abdominal aortic aneurysm received a CT scan of the chest for restaging of the squamous cell lung carcinoma.
This study reported a 3 cm mass in the mid and distal anterolateral wall of the left ventricle (Figure 1). Aside from the patients preexisting well-compensated chronic diastolic heart failure, the mass was felt to be clinically asymptomatic. Physical exam findings showed a well appearing patient in no acute distress. There was no jugular venous distention and cardiac auscultation demonstrated a regular rate and rhythm without murmurs or gallops. Pulmonary exam revealed diffusely decreased breath sounds with no obvious rales or rhonchi. Radial and pedal pulses were palpable bilaterally. There was no peripheral edema.
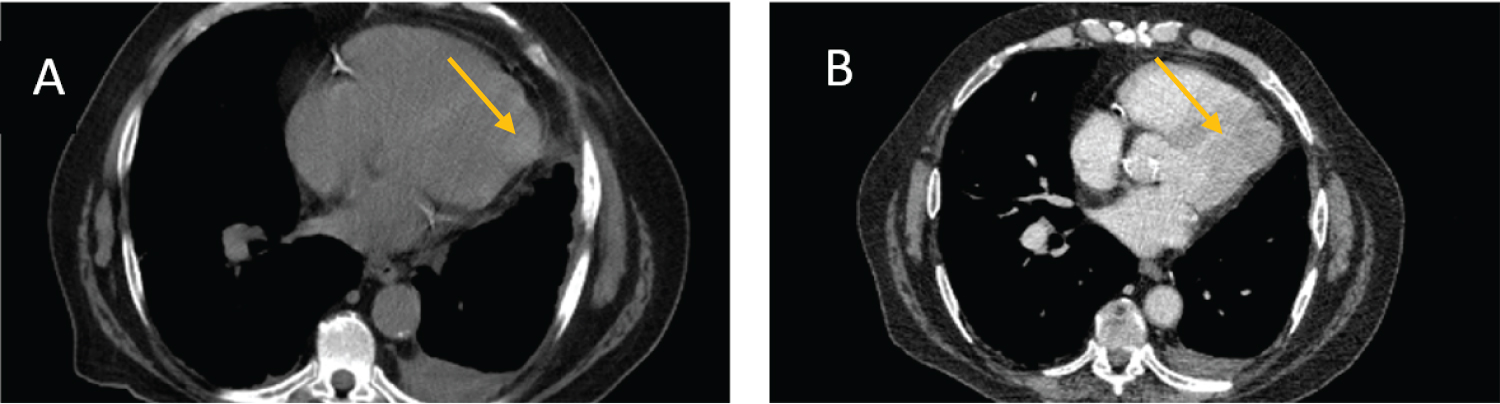 Figure 1: Staging CT for patient's known squamous cell carcinoma. A) Noncontrast and B) contrast enhanced CT chest showing mass in the mid to distal anterolateral wall of left ventricle.
View Figure 1
Figure 1: Staging CT for patient's known squamous cell carcinoma. A) Noncontrast and B) contrast enhanced CT chest showing mass in the mid to distal anterolateral wall of left ventricle.
View Figure 1
Cardiac MRI (Figure 2) demonstrated a mass in the anterolateral wall measuring 19.7 × 32.8 × 39 mm. The mass was described as hypointense on T2 weighted images with isointense to slightly hypointense on T1 weighted imaging sequences. For the mass, there was limited first pass perfusion and profound, extensive late gadolinium uptake. These findings supported a diagnosis of a large cardiac fibroma. The calculated LV ejection fraction was estimated at 50%. There was "possible compression of the apical anterolateral wall from the mass that may impact diastolic relaxation". The calculated RV ejection fraction was 44%. On late gadolinium imaging, there was no myocardial infarction noted.
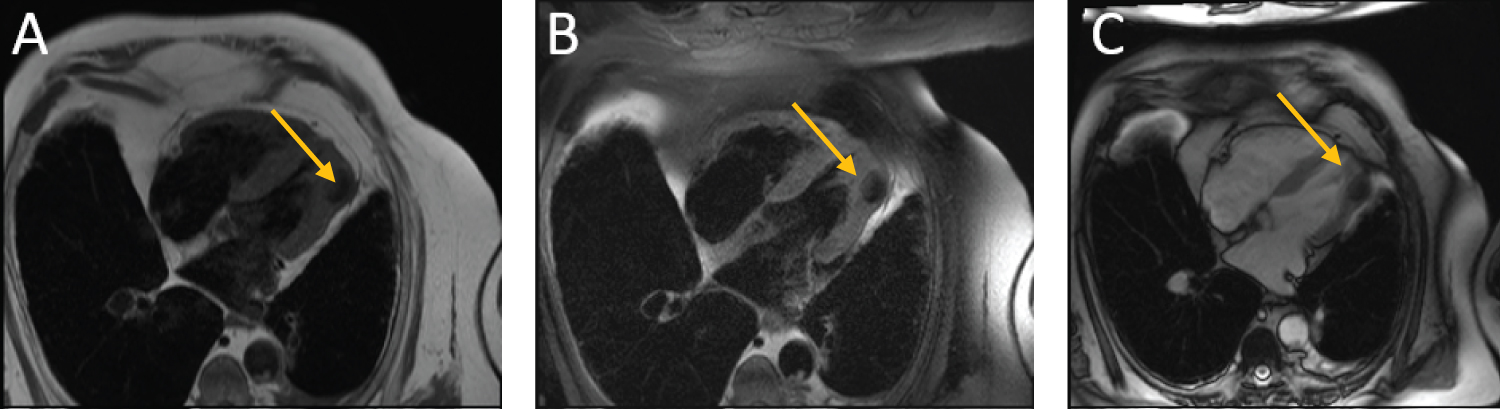 Figure 2: Magnetic Resonance Imaging portraying the cardiac fibroma. A) T1; B) fat saturated T1 and C) T2 are depicted.
View Figure 2
Figure 2: Magnetic Resonance Imaging portraying the cardiac fibroma. A) T1; B) fat saturated T1 and C) T2 are depicted.
View Figure 2
In view of the patient's metastatic lung cancer, advanced age, multiple comorbidities, and lack of refractory symptoms referable to the cardiac fibroma, the cardiology team decided it was best to treat the patient medically with clinical observation & repeat imaging as needed.
Cardiac tumors are rare and vary greatly in location, size, and clinical manifestations. In adults, cardiac tumors are most commonly due to metastasis but can also arise as a primary lesion in the heart. In our patient presented with metastatic lung cancer, the initial consideration was that the lesion detected was a metastatic tumor.
Comprehensive cardiac imaging confirmed the mass was an incidental, benign cardiac fibroma.
Primary cardiac tumors are extremely rare and range in incidence from 0.0017 to 0.019% [4-6]. In adults, metastatic, secondary, cardiac tumors are 100-fold more frequent than primary tumors, with metastatic tumors typically arising from melanomas, lymphomas and from lung, breast or renal cancers [7,8]. The symptoms can range from completely asymptomatic to heart failure to life threatening arrhythmias.
The finding of a cardiac fibroma in our patient at 83 years of age is highly unusual as the mean age of patients with cardiac fibroma is 13 years [2]. Cardiac fibromas are benign growths of fibroblasts located in the myocardium. In 57% of cases, they localize to the left ventricle [5,9]. The second most common location for growth is the right ventricles at 27.5% [1,5]. Histology is not needed to make a definitive diagnosis but can demonstrate some histological differences such as older patients tending to have more collagen present in the tumor [5].
Clinical manifestations of a cardiac fibroma vary greatly and mostly depend on the size and location of the tumor. About 75% of primary benign cardiac tumors [4-6] and one- third of cardiac fibromas are asymptomatic and are found incidentally on imaging or in autopsy [1]. When symptoms do arise, they are usually with a triad of blood flow obstruction leading to heart failure, tumor embolization and/or constitutional symptoms [7]. Given their location, cardiac fibromas have the potential to disrupt normal electrical pathways in the heart leading to conduction defects and possibly, sudden cardiac death due to ventricular arrhythmias [1,4]. Echocardiogram and magnetic resonance imaging should be performed to describe the tumor and a treatment plan should be formulated in order to avoid potential lethal complications [3].
Treatment options considered when managing cardiac fibromas include surgical and pharmacological approaches. Due to the rarity of the condition, an optimal treatment strategy has not been standardized, and indications for timing of surgery are not well defined [5]. Surgical options include complete excision, incomplete resection, or orthotropic heart transplant [1,8]. When resectable, cardiac fibromas tend to have a good prognosis. Arrhythmias can be managed with beta-blockers, amiodarone, and possibly surgical interventions [5]. Given our patient's multiple comorbid conditions, advanced age, and stable cardiac symptomatology, it was elected to avoid surgical treatment and follow the patient medically.
We report a unique case of an 83-year-old male presenting with metastatic lung cancer with an incidental finding of a cardiac tumor on staging CT scan. Given the patient's age and known metastatic lung cancer, the working differential diagnosis focused on metastatic cardiac etiology. With proper use of cardiac imaging, a correct diagnosis of cardiac fibroma was made and a proper therapeutic plan for this patient could be instituted. As thoracic and cardiac imaging techniques evolve, the findings of cardiac tumors, such as fibromas, may become more common in adults and further study should help us understand the natural history and appropriate management of these rare tumors.
Steven J Grampp and Christopher D Manko contributed equally to the work.