Cardiogenic shock (CS) occurs up to 10% of patients with acute myocardial infarction (AMI) and is associated with a high (> 50%) in-hospital mortality. Mechanical circulatory support (MCS) devices, such as Impella CP, are increasingly being used in patients with AMI complicated by CS. Recent data highlighted the issue of vascular complication and bleeding events in cardiogenic shock patients treated with Impella. In this setting, the "Single-access for High-risk PCI" (SHiP) technique and the use of safe and effective vascular closure devices (VCD) could be useful to reduce the vascular complication rate. We report a case of AMI-related CS in which a single femoral access, used for both Impella CP and percutaneous coronary intervention (PCI) of critical left main stenosis, was successfully closed by the MANTA VCD using a depth locator tool. This strategy allows to limit the number of arterial access sites and to reduce the profile of interventional tools through femoral and iliac artery. Furthermore, the use of MANTA VCD is an important innovation to achieve hemostasis after removal of large-bore sheath needed to MCS in AMI complicated by CS, reducing vascular complication and arterial access site bleeding.
Cardiogenic shock, Acute myocardial infarction, Mechanical circulatory support, Vascular closure device, Vascular access site, High-risk percutaneous coronary intervention, Case report
CS: Cardiogenic Shock; AMI: Acute Myocardial Infarction; MCS: Mechanical Circulatory Support; SHiP: Single-Access for High Risk PCI; VCD: Vascular Closure Device; PCI: Percutaneous Coronary Intervention; STEMI: ST-Elevation Myocardial Infarction; LVED: LV Ejection Fraction; SCAI: Society for Cardiovascular Angiography and Interventions
Cardiogenic shock (CS) occurs in 5 to 10% of patients with acute myocardial infarction (AMI) and is associated with a high (> 50%) in-hospital mortality [1]. Mechanical circulatory support (MCS) devices are increasingly being used in patients with AMI complicated by CS, although their clinical advantage is still controversial [2]. The Impella CP (Abiomed, Danvers, MA) is a continuous-flow MCS device with a microaxial pump that decompresses the left ventricle and delivers a maximum flow of 4.0 L/min into the ascending aorta. In the setting of CS, the Impella device unloads the ventricle, reduces ventricular end- diastolic pressure, increases mean arterial pressure and decreases myocardial oxygen consumption. In April 2016, the US Food and Drug Administration approved the Impella device for use in AMI-related CS based on circulatory support effect, not based on improved clinical outcomes [2]. Though, recent data highlighted the issue of vascular complication and bleeding events in cardiogenic shock patients treated with Impella, occurring respectively in 7.4% and 15.2% of the cases [3]. In this setting, the "Single-access for High-risk PCI" (SHiP) technique and the use of safe and effective vascular closure devices (VCD) could be useful to reduce the vascular complication rate [4,5]. We report a case of AMI-related CS in which a single femoral access, used for both Impella CP and percutaneous coronary intervention (PCI), was successfully closed by the MANTA VCD.
A 72-year-old female without known risk factors nor previous cardiac history was admitted to the emergency department of a spoke centre for relapsing chest pain episodes over the last 24 h. On the 12-lead electrocardiogram a diagnosis of sub-acute anterior ST-elevation myocardial infarction (STEMI) was made and the patient was transferred to our catheterization laboratory to undergo invasive treatment. At presentation, systolic blood pressure was 85 mmHg, heart rate was 105 beats/min, arterial oxygen saturation was 92%, and lactate level was 1.4 mmol/L. The echocardiographic assessment performed at baseline revealed severe left ventricular dysfunction (LV ejection fraction [LVEF] = 25%) and preserved right ventricular function (tricuspid annular plane systolic excursion = 21 mm; fractional area change = 36%). According to the high-risk features that frame the clinical case as stage B cardiogenic shock ("Beginning" CS or pre-shock/compensated shock) according to Society for Cardiovascular Angiography and Interventions (SCAI) consensus, we chose to perform elective LV unloading before reperfusion by using Impella CP device [2,6].
The Impella 14F sheath was advanced into the right common femoral artery under fluoroscopic guidance, and the Impella CP device was placed in the left ventricle according to the recommendations. Subsequently, a micropuncture access needle was used to pierce the hemostasis valve in the superior portion of the Impella sheath (with care to avoid piercing the Impella catheter) and a 6F sheath was advanced through a 0.035" guidewire, according to the ShiP technique [5], in order to perform coronary angiography and eventual PCI (Figure 1). A tight (> 80%) distal left main stenosis involving the ostium of left anterior descending in a left dominance system was documented. We therefore performed an Impella-assisted PCI. Using a 6F extra back-up 4 Launcher guide catheter (Medtronic, Minneapolis, MN), a provisional stenting of left main and proximal left anterior descending was performed with final kissing balloon to optimize stent apposition. The final angiographic result was good (residual stenosis < 10% and TIMI 3 antegrade flow). The procedure was carried out without complications. Hemodynamic conditions were stable during the entire procedure and vasopressors were not required. MCS was maintained for 24 hours. Hemostasis of the right femoral arterial access was achieved using a 14F MANTA VCD (Teleflex, Wayne, PA): After removing the 14F Impella sheath over a 0.035" guidewire, we used the 14F puncture location dilator (depth locator) to measure the length of the subcutaneous track from the skin to the endovascular lumen (Video 1). A 2D-color Doppler exam of the right femoral access site showed effective access site closure (Figure 2). The patient was discharged after 5 days with an almost complete recovery of left ventricle function.
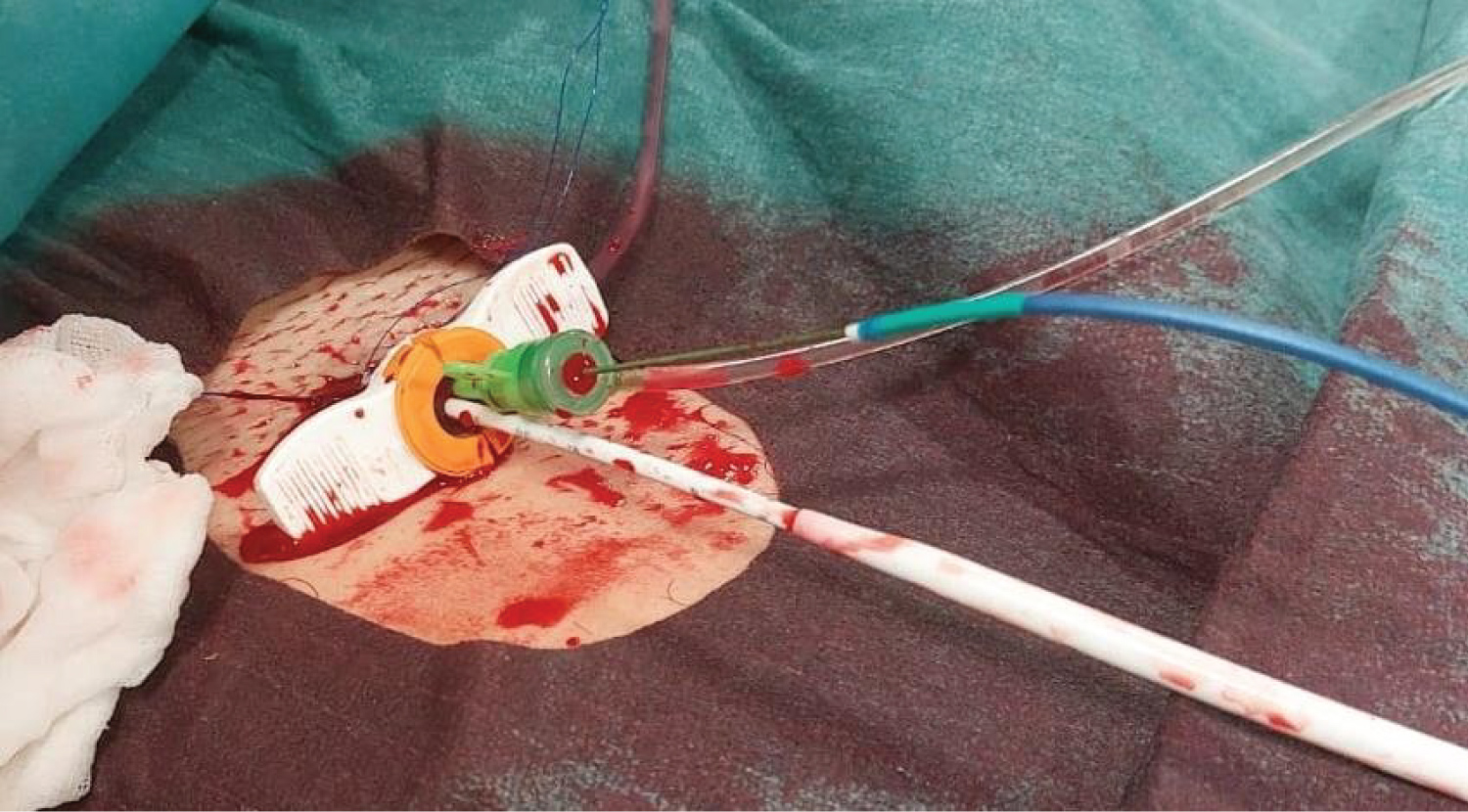 Figure 1: Single-access technique. The Impella 14 F sheath was advanced into the right common femoral artery. Two catheters were introduced into the 14F sheath: a) The Impella CP catheter (white catheter) and b) a 6F sheath (green) through which perform coronary angiography and percutaneous coronary intervention.
View Figure 1
Figure 1: Single-access technique. The Impella 14 F sheath was advanced into the right common femoral artery. Two catheters were introduced into the 14F sheath: a) The Impella CP catheter (white catheter) and b) a 6F sheath (green) through which perform coronary angiography and percutaneous coronary intervention.
View Figure 1
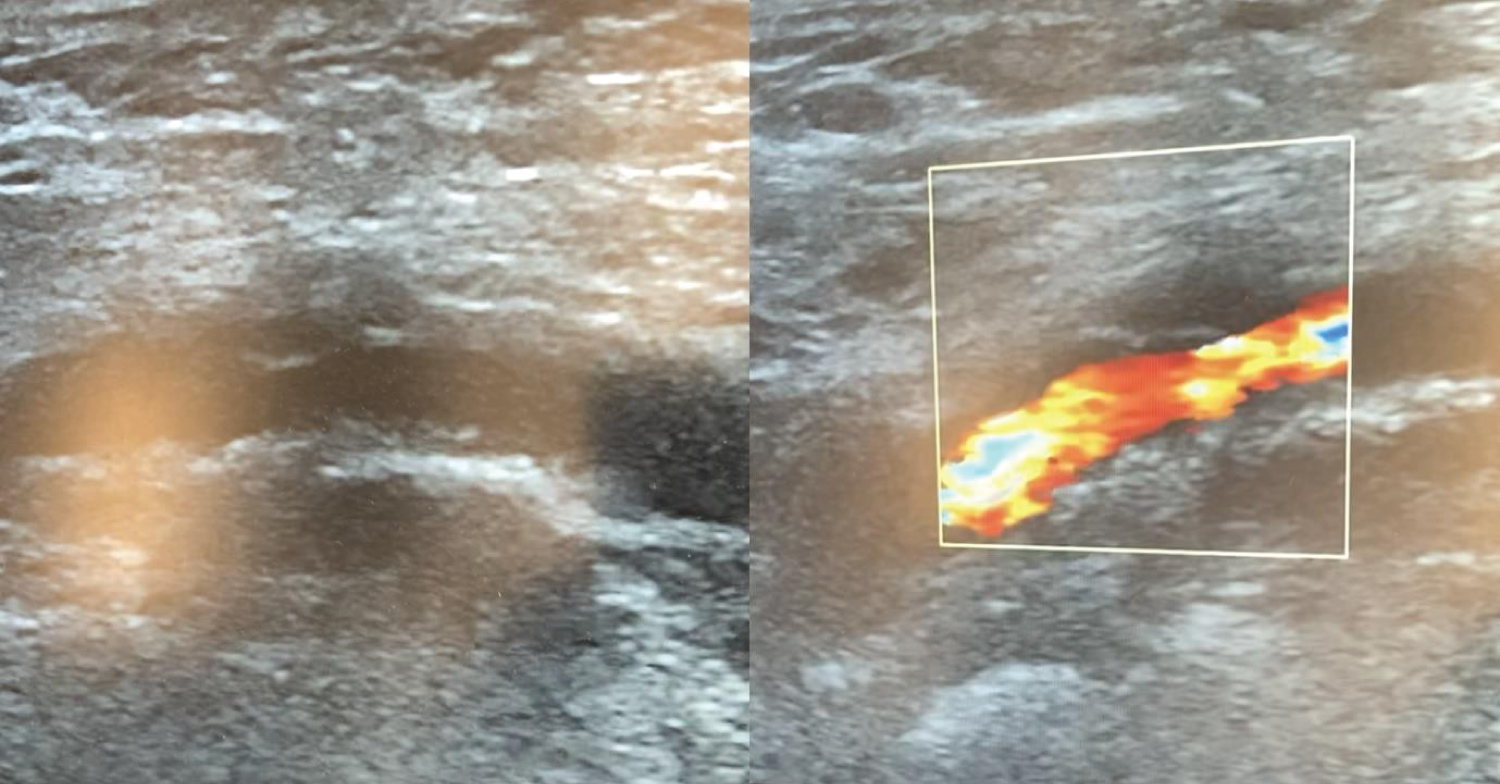 Figure 2: Ultrasound examination. Effective sealing of the access site in the right common femoral artery assessed by two-dimensional and Color-Doppler examination.
View Figure 2
Figure 2: Ultrasound examination. Effective sealing of the access site in the right common femoral artery assessed by two-dimensional and Color-Doppler examination.
View Figure 2
Video 1: A) The 14F puncture location dilator (depth locator) is advanced to measure the distance (in centimeters) from the arteriotomy to the skin level. Pulsatile blood emerges when the location dilator tip is in the arterial vessel. The operator pulls back the dilator until the blood flow ceases and the depth of the vessel lumen can be read from the metric ruler; B) Following assessment of the artery puncture site depth, the dedicated MANTA sheath is advanced and access closure is obtained with the MANTA closure unit. View Video 1
To the best of our knowledge, this is the first description of an Impella-assisted PCI in an AMI-related CS patient using a single arterial access which was successfully managed with a 14F MANTA VCD and the new 14F puncture location dilator.
Cardiogenic shock is still a clinical setting weighed on by a high rate of in-hospital mortality although MCS could play an important role favoring left ventricular unloading and systemic effective perfusion [2]. Unfortunately, bleeding and vascular major complication are quite frequent and correlated to large sheath needed to place mechanical circulatory support devices [7].
Strategies to reduce bleeding and vascular complications include: 1) limiting the number of arterial access sites; 2) optimize artery puncture technique; 3) use of effective and safe VCD. SHiP technique has been proposed to allow for rapid and safer single access utilizing only the Impella access site [5]. The Impella 14F sheath is labeled to be used as access for 6F and 7F femoral sheath, in order to reduce the number of puncture sites and to reduce the profile of interventional tools through femoral and iliac artery; sheathless guiding in the Impella 14F sheath has been described [8].
Current approach to achieve hemostasis after large-bore sheath removal includes a suture- based "Preclose" technique, where one (or two) suture device is used at the beginning, before large-bore access sheath positioning [9]. This approach however is time consuming. Indeed, compared to patients undergoing elective or scheduled procedures, in emergency setting such as cardiogenic shock, a dedicated, meticulous access approach may be precluded and associated with a significant failure rate.
An alternative approach is the use of the 14F MANTA VCD. This implies the initial assessment of the artery puncture site depth by the 8 Fr puncture location dilator provided by the MANTA VCD. This approach, however, requires 1) The availability of a separate sterile package of the location dilator, under penalty of wasting a MANTA device; 2) The risk of inaccuracy due to the presence of hematoma developed after femoral artery puncture; 3) The need to remember or keep the value of puncture site depth for several hours or days. Indeed, the median duration of support with Impella device in studies focusing on AMI complicated by CS ranged from 38 to 49 hours [10].
The new 14F puncture location dilator allows to assess artery puncture site depth when the mechanical support is suspended. The availability of the 14F puncture location dilator therefore obviates to all the above issues and represents an important innovation to achieve hemostasis after removal of large-bore sheath needed to MCS in AMI complicated by CS.
In AMI-related CS an Impella-assisted PCI may be carried out through a single arterial access which may be successfully managed with a 14F MANTA VCD and the new 14F puncture location dilator.
All authors listed have made a substantial, direct and intellectual contribution to the work, and approved it for publication.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.