Cardiac resynchronization therapy, Side helix, Biventricular pacemaker, Atrioventricular block, Active fixation lead
Cardiac resynchronization therapy (CRT) has become an established treatment for heart failure patients with conduction disorders and a significantly reduced ejection fraction [1]. Nevertheless, CRT is limited by several complications, many of which are associated with the insertion of the left ventricular (LV) lead [2]. The LV lead should be placed at the most delayed site in the left ventricle [1]. However, placing the LV lead on the coronary sinus (CS) branch at the target delay site is difficult during CRT. This led to the development of a more stable lead for the pacing of the LV at the most suitable site. The design of the Medtronic Attain Stability Quad 4798 (ASQ; Medtronic, Dublin, Ireland) lead is based on the Attain Performa family of steroid-eluting quadrupole LV leads. The new design features an electrically inert side-helix placed between the 3rd and 4th pacing electrodes (Figure 1). We report the successful implantation of LV leads in a series of processes to date without changing the procedure of CRT using a new method that uses ASQ to target CS branches with difficult anatomy.
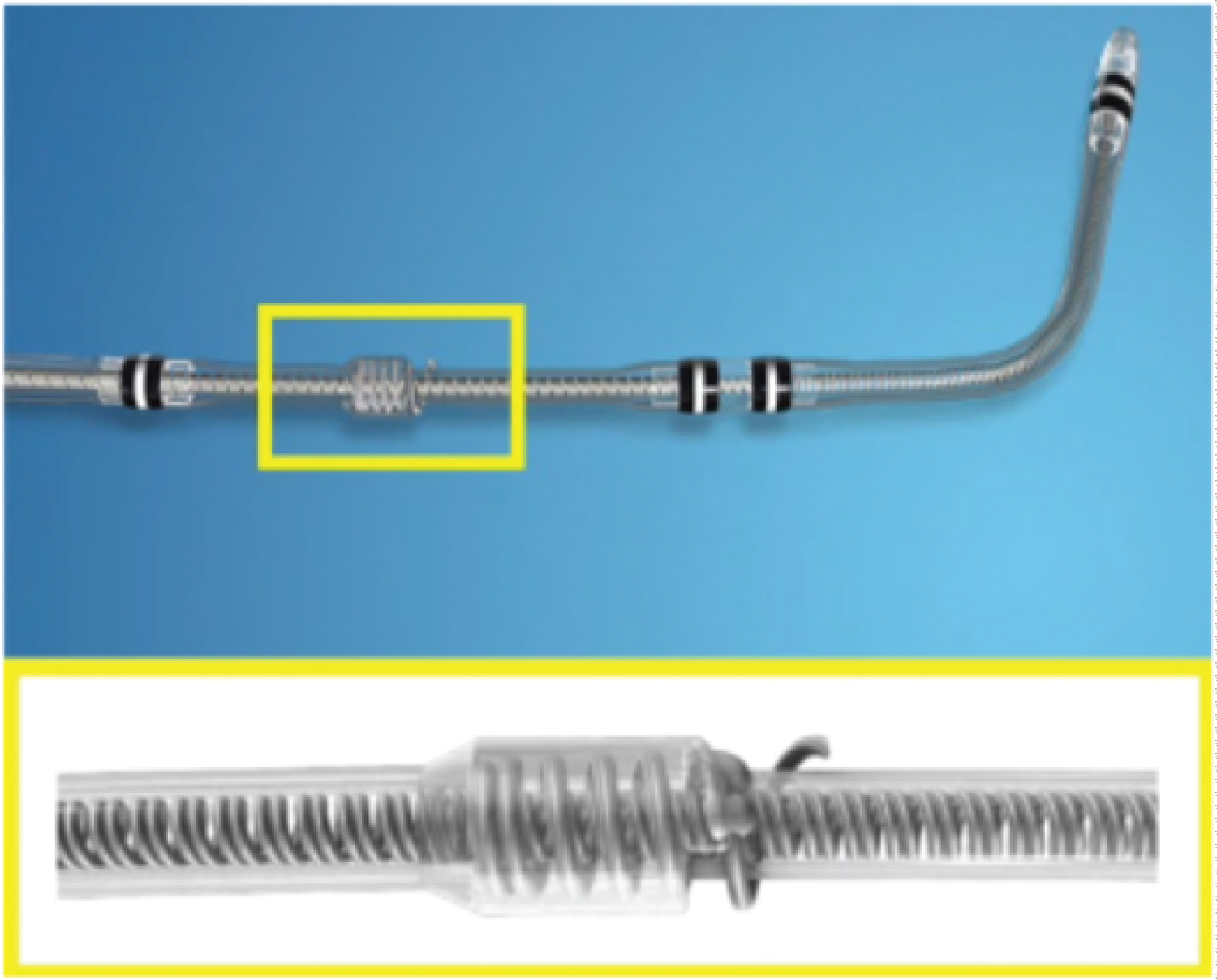 Figure 1: The Attain Stability Quad 4798. This left ventricular lead was released by Medtronic in Japan in 2020. Shown here is the side-helix for active fixation into the target vein.
View Figure 1
Figure 1: The Attain Stability Quad 4798. This left ventricular lead was released by Medtronic in Japan in 2020. Shown here is the side-helix for active fixation into the target vein.
View Figure 1
A 75-year-old man presented with non-ischemic cardiomyopathy with no other comorbidities, dyspnea, or optimal heart failure medications. Electrocardiography showed an advanced atrioventricular block (Figure 2A). He had heart failure with a reduced LV ejection fraction (EF) of 20% on echocardiography. Computed tomography (CT) coronary angiography revealed coronary artery stenosis and the presence of a lateral branch (Figure 3).
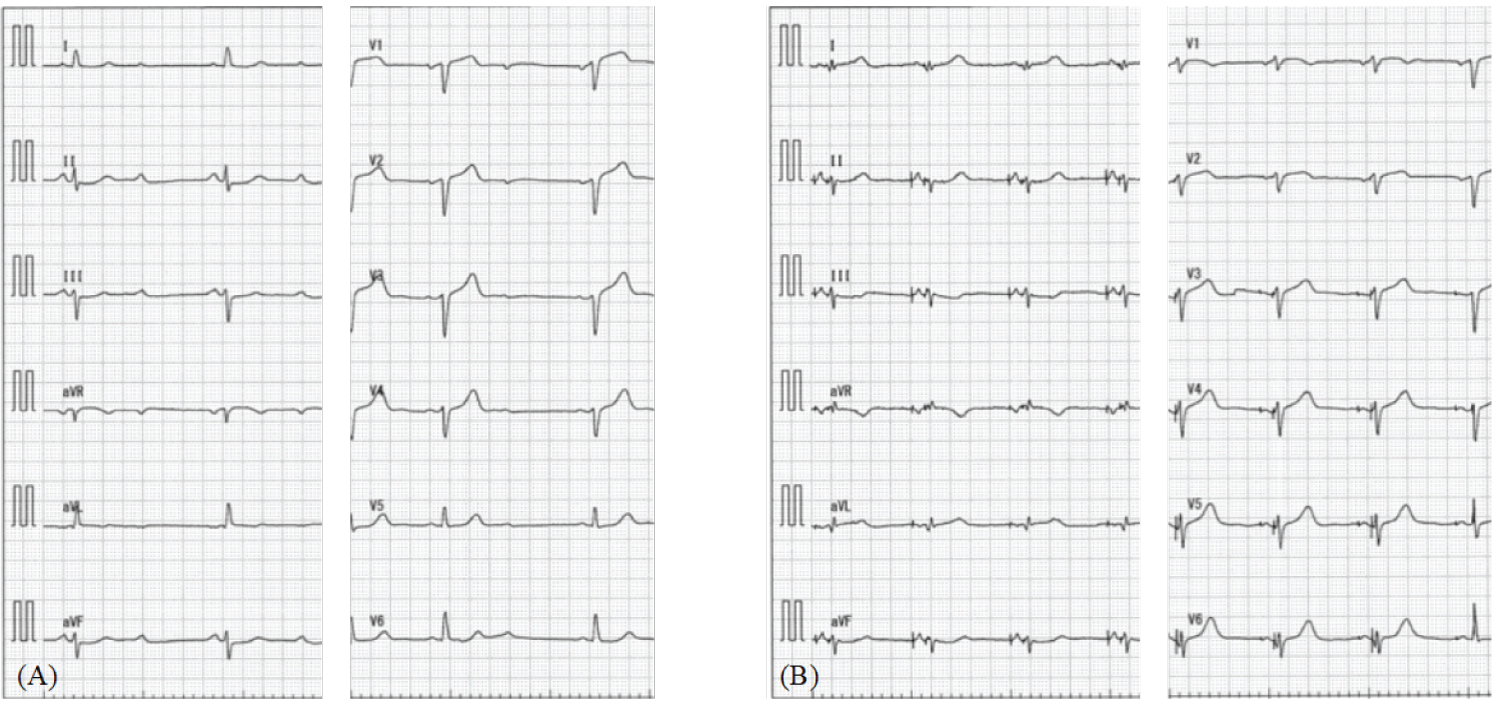 Figure 2: A) Electrocardiogram (ECG) showed advanced atrioventricular block; B) Post implantation ECG showed QRS duration of 104 ms.
View Figure 2
Figure 2: A) Electrocardiogram (ECG) showed advanced atrioventricular block; B) Post implantation ECG showed QRS duration of 104 ms.
View Figure 2
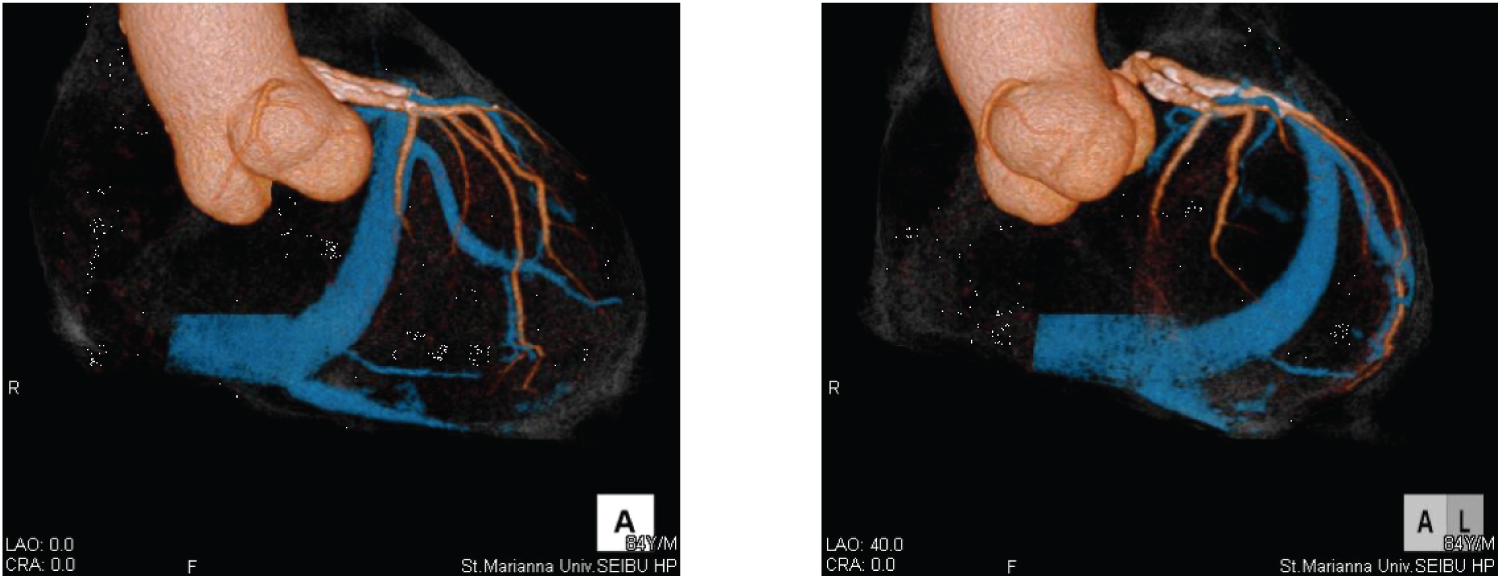 Figure 3: Computed tomography coronary angiography revealed the existence of a lateral branch.
View Figure 3
Figure 3: Computed tomography coronary angiography revealed the existence of a lateral branch.
View Figure 3
The patient was a CRT-adapted patient and further CRT was performed upon admission. The leads were punctured in the left subclavian vein after creating a left pocket. The CS was cannulated successfully using a CS guiding catheter (Attain Command™ + SureValve™ integrated valve, Medtronic). After inserting the guide catheter into the CS, venography was performed to confirm the same lateral branch of the CS as in the CT. Using a Runthrough NS 0.014-inch peripheral angioplasty wire (TERUMO, Tokyo, Japan) was difficult. We attempted to advance a 90° microcatheter (Attain Select II™ + SureValve™ sub-selection catheter, Medtronic) along with the ASQ lead; however, the microcatheter did not advance over the lateral branch owing to venous tortuosity (Figure 4A, Figure 4B and Figure 4C). We applied a technique using active fixed LV leads, which has already been reported as an anchoring technique [3]. The ASQ lead screw was in the distal segment of the lateral branch (Figure 4D). Next, we attempted to advance a microcatheter by pulling the ASQ lead, and the microcatheter was advanced over the tortuous lateral branch (Figure 4E). Because the ASQ leads are fixed, they do not shift when the ASQ leads are pulled. The ASQ lead was screwed out and led to passing the tortuous lateral branch, and the ASQ lead was finally implanted through it (Figure 4F). Good pacing parameters were obtained without phrenic nerve stimulation. We successfully placed the right ventricular (RV) lead (Sprint Quattro 6935M-55, Medtronic) at the apex of the RV and the right atrial (RA) lead (CapSure Sense 4574-45, Medtronic) in the RA appendage. We connected all leads to the generator (Cobalt XT HF Quad, Medtronic) and closed the pocket. The electrocardiogram after implantation had QRS duration of 104 ms (Figure 2B). Patient follow-up at 6 months postoperatively showed NYHA class 2 with an improvement in EF of 35%, and CRT was continued.
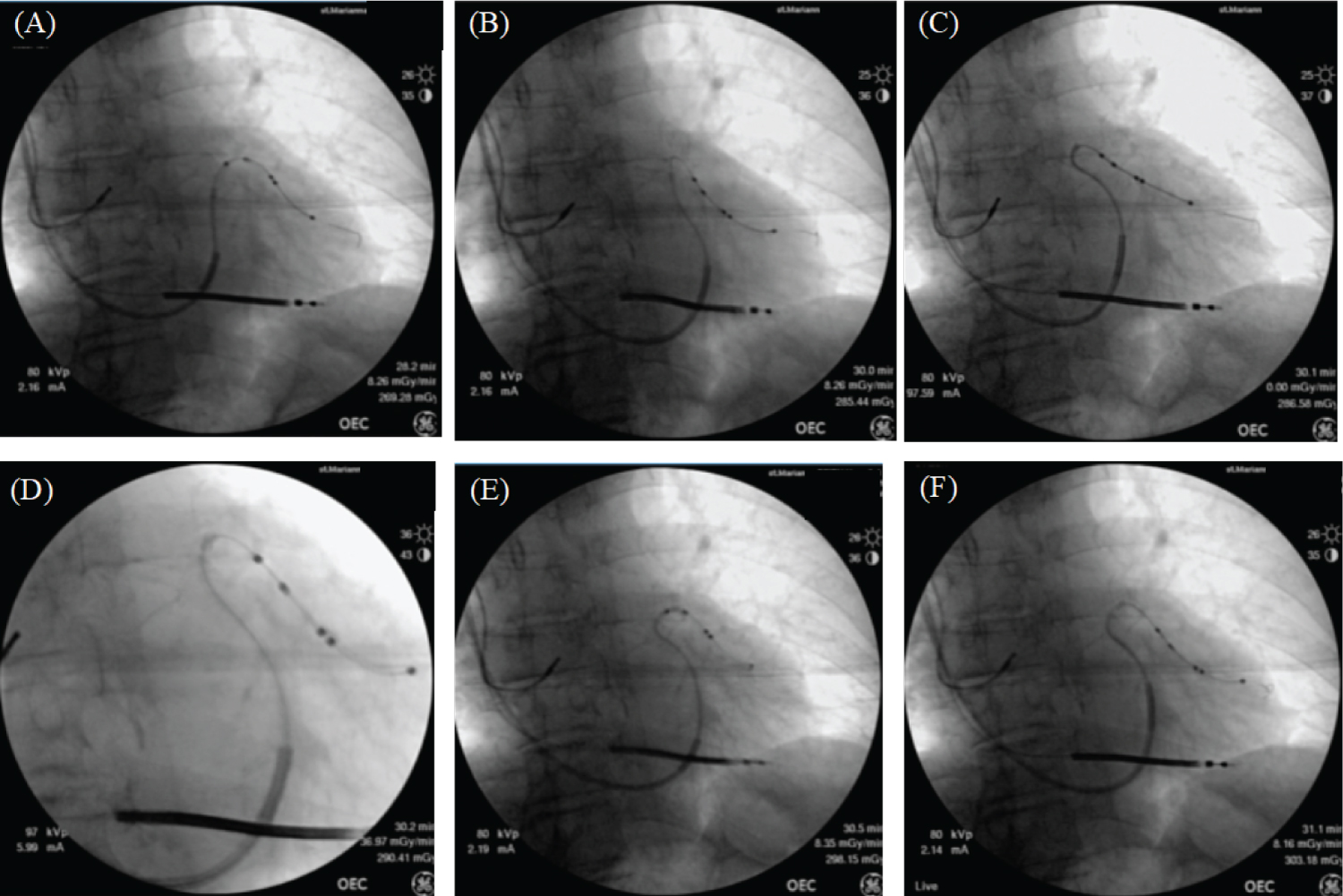 Figure 4: A deeper left ventricular (LV) lead results in deeper positioning of the cannula insertion catheter. Deep engagement of the cannula insertion catheter is obtained without the LV lead coming off. The leads rotate counterclockwise, releasing the fixation mechanism from the venous wall, advancing the LV leads, and helping the LV leads to cross the target site.
View Figure 4
Figure 4: A deeper left ventricular (LV) lead results in deeper positioning of the cannula insertion catheter. Deep engagement of the cannula insertion catheter is obtained without the LV lead coming off. The leads rotate counterclockwise, releasing the fixation mechanism from the venous wall, advancing the LV leads, and helping the LV leads to cross the target site.
View Figure 4
The anatomy of the branches of the CS is diverse and includes the arrangement, hardness, and size of the branches and the presence of branches at suitable sites. Most CS variability is fine, but it is one of the most important factors in clinical outcomes at the location of LV leads. There are several methods for LV lead placement. One method is to advance the vein selector to the CS using hardwire. While maintaining the CS selector, this wire is replaced with a long, hardwire that acts as a more robust rail for advancing the CS sheath throughout the CS. The small branches of the CS are canalized to provide additional stability to the CS outer sheath during lead positioning [4]. Another method is to use a successfully executed anchor balloon for winding the CS branch. This improves the success rate of LV lead placement in CRT [5]. Similar procedures have been described for anchor technology in the past [3]. This report provides an interesting example of LV lead placement due to lateral branch flexion. In this case, the interesting point is the same procedure as the LV injection of LV leads, without the use of other devices or techniques. The sharp angles and tortuosity of the CS branches hinder the implantation of the LV leads. Our method succeeded in the procedure in a series of LV lead implantations without causing damage to the CS and without changing many procedures. Therefore, in patients with winding CS bifurcations, ASQ leads may improve the success rate of LV lead placement compared to other LV leads.
In conclusion, LV lead positioning during CRT remains the most difficult and important determinant for predicting response to CRT. The ASQ lead overcame the anatomical disorder of the CS, enabling LV pacing from a more optimal site. Using the ASQ lead is a viable and easily applicable method that can overcome the tortuosity of the target venous branches with sharp angles.
We would like to thank Editage (www.editage.com) for English language editing.
We would like to thank Y. Izaki for technical assistance.
The authors declare no conflict of interest for this article.
The case report was approved by the Institutional Committee on Human Resource at St. Marianna University School of Medicine (No. 4673), and written informed consent was obtained from all patients (via the opt-out method) at our institution.
There is no funding.
Not applicable.