Over one million people are smoking worldwide and the total numbers is expected to increase each year [1]. Several studies have shown a relation between smoking and heart problems, which highlight special consideration in smoking cessation awareness in heart disease patients with established vascular disease as a secondary prevention.
To evaluate the current awareness of smoking cessation products in heart disease patients at governmental hospitals in Jeddah.
Cohort structured questionnaire-based interview was held.
Tertiary governmental hospitals.
Heart disease patients who are following up in cardiology clinics in governmental hospitals in Jeddah.
Awareness of smoking cessation products and its usage.
150 patients were interviewed. 19% (n = 28) were smokers, 2% (n = 3) returned to smoke (31 are active smokers), 56% (n = 85) non-smoker and 23% (n = 34) quitted smoking. Their average age is 60 ± 5 years and 70% (n = 105) of the patients were males. Regarding the level of awareness of the availability of smoking cessation products 32.2% (n = 47) of the patients were aware of the nicotine patch, 30.2% (n = 44) of patients were aware of nicotine gum, 18.1% (n = 26) of patients were aware of nicotine lozenge, 7.4% (n = 11) of patients were aware of varenicline) Chantix®), 1.3% (n = 2) of the patients were aware of cystisine and only 0.7% (n = 1) were aware of bupropion HCl. The motivators for quitting smoking in 65 of the smokers (actively smoking and patients who quitted smoking) were 36% (n = 21) for self-motivation, 34% (n = 20) for physicians, 25% (n = 15) for family members and 5% (n = 3) for friends. And out of 65 patients (actively smoking and patients who quitted smoking) only 10.8% (n = 7) visited smoking cessation clinic.
The poor awareness of the smoking cessation products shown in this study, suggests that strategies of support and control are urgently needed especially in heart disease patients with underline high risk.
Smoking cessation, Heart disease, Quit, Awareness, Governmental hospitals
The World Health Organization described tobacco smoking as an epidemic, with an expectation of three million deaths yearly, worldwide, because of smoking. This figure is expected to rise to ten million a year by the years 2020s or early 2030s, if the current states of smoking continue. The developing countries will have seventy percent deaths due to smoking [2].
The World Health Organization described tobacco smoking as an epidemic, with an expectation of three million deaths yearly, worldwide, because of smoking. This figure is expected to rise to ten million a year by the years 2020s or early 2030s, if the current states of smoking continue. The developing countries will have seventy percent deaths due to smoking [2].
Smoking damages the lining of the arteries, leading to a buildup of fatty material (atheroma) which narrows the artery. This can cause angina, a heart attack or a stroke. The carbon monoxide in tobacco smoke reduces the amount of oxygen in the blood. Which highlight special consideration in smoking cessation awareness in heart disease patients with established vascular disease as a secondary prevention [5].
The Saudi Smoking Control Charitable Society, over the last fourteen years, has built 33 smoking cessation clinics all over the country. The visits rates of these clinics are limited, with a quitting rate of 13% [6]. However, this figure should be clarified with caution, since there is no accurate data on the duration of follow up and the relapse rate.
Consecutive attenders at a routine cardiac clinics in Jeddah of large governmental hospitals which are King Abdulaziz University Hospital, King Fahad Hospital and King Abdulaziz Medical City -Cardiology center- were approached, and interviewed whether they were current cigarette smokers or not. A structured questionnaire interview was held with 150 current patients attending cardiology clinics. Data collection included age, sex, type of heart disease, presence of hyperlipidemia, smoking status, their knowledge about the availability of the smoking cessation products which are varenicline (Chantix®), cystisine (Tabex®), nicotine lozenge, nicotine Patch (Quit4®, Equate®, Polacrilex®, Nicotinell®) and nicotine gum (Equate®, Polacrilex®, Nicorette®). They were all asked on a person-to-person basis, who filled in the appropriate answers on the form. More data were collected in smokers including number of cigarettes per day, duration of smoking, their willing to quit smoking, difficulty of smoking cessation, knowledge about the smoking cessation clinics around, methods used for quitting, reason of trying to quit and if the patient has used any medication to help quitting.
150 questionnaires were filled and the baseline characteristic of heart disease patients (Table 1) include 70% (n = 105) males and the average age of the patients were 60 ± 5 years, the type of heart diseases include 42% (n = 69) of patients had hypertension, 18% (n = 30) of patients had cardiovascular disease, 11% (n = 18) of patients had cardiomyopathy, 11% (n = 18) of patients had angina pectoris, 11% (n = 18) of patients had valvular heart disease, 5% (n = 8) of patients had arrhythmia, 1% (n = 2) of the patients had pericarditis presented and 1%(n = 2) of patients had myocarditis (Figure1).
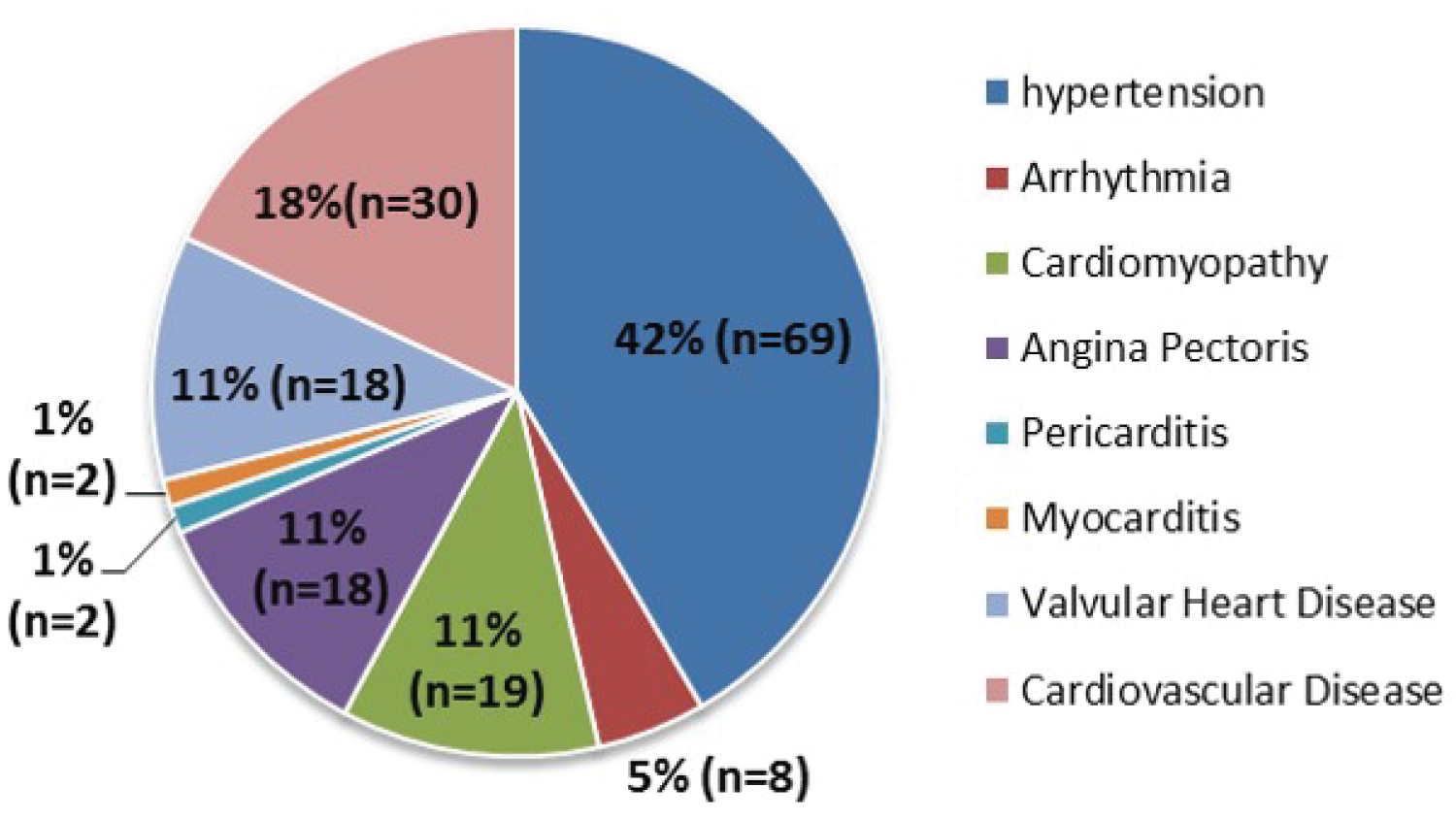 Figure 1: Type of heart disease.
View Figure 1
Figure 1: Type of heart disease.
View Figure 1
Table 1: The baseline characteristics. View Table 1
In 150 Cardiac patients 19% (n = 28) were smokers, 2% (n = 3) returned to smoke (31 are active smokers), 56% (n = 85) non-smoker and 23% (n = 34) quitted smoking (Figure 2). The Awareness of smoking risk on the heart was 89.3% (n = 134) in the heart disease patients.
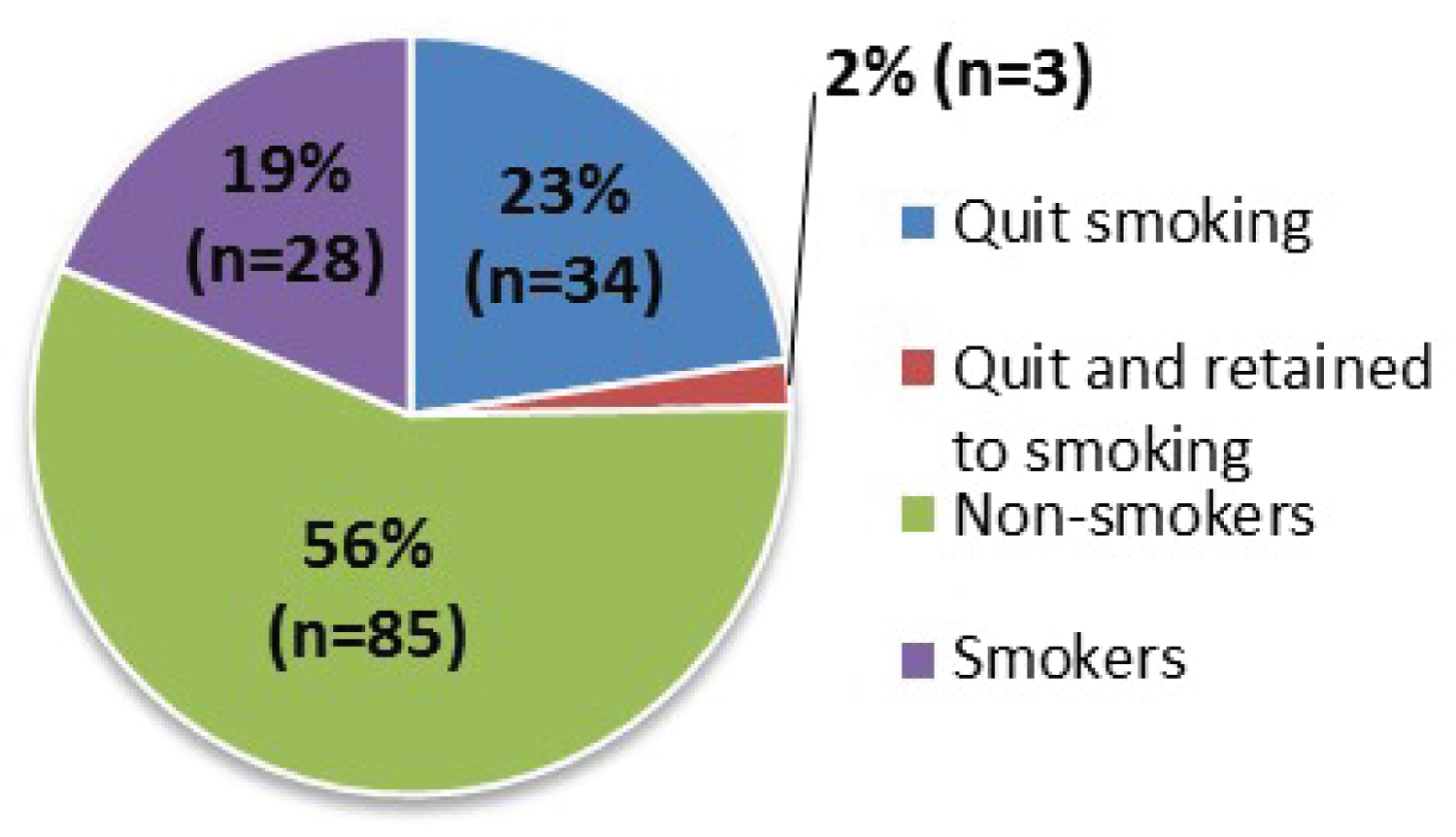 Figure 2: Status of the patients.
View Figure 2
Figure 2: Status of the patients.
View Figure 2
The consumption of cigarette in the 65 patients (actively smoking and patients who quitted smoking) showed that 57% (n = 37) of the patients consume packet or more per day which is the most consumed amount, 22% (n = 14) of the patients consume less than 5 cigarettes per day, 12% (n = 8) of the patients consume 16 ± 3 cigarettes per day and 9% (n = 6) of the patients consume 9 ± 3 cigarettes (Figure 3). Patients’ awareness of smoking risk on the heart was 89.33% (n = 134). The intention to quit smoking was in 76.9% (n = 50) of the smokers, though 52% (n = 34) of the patients succeeded in quitting, 25% (n = 16) returned to smoke and 23% (n = 15) of the patients were not willing to quit (Figure 4). The percentage of smokers who visited smoking cessation clinic was only 10.8% (n = 7).
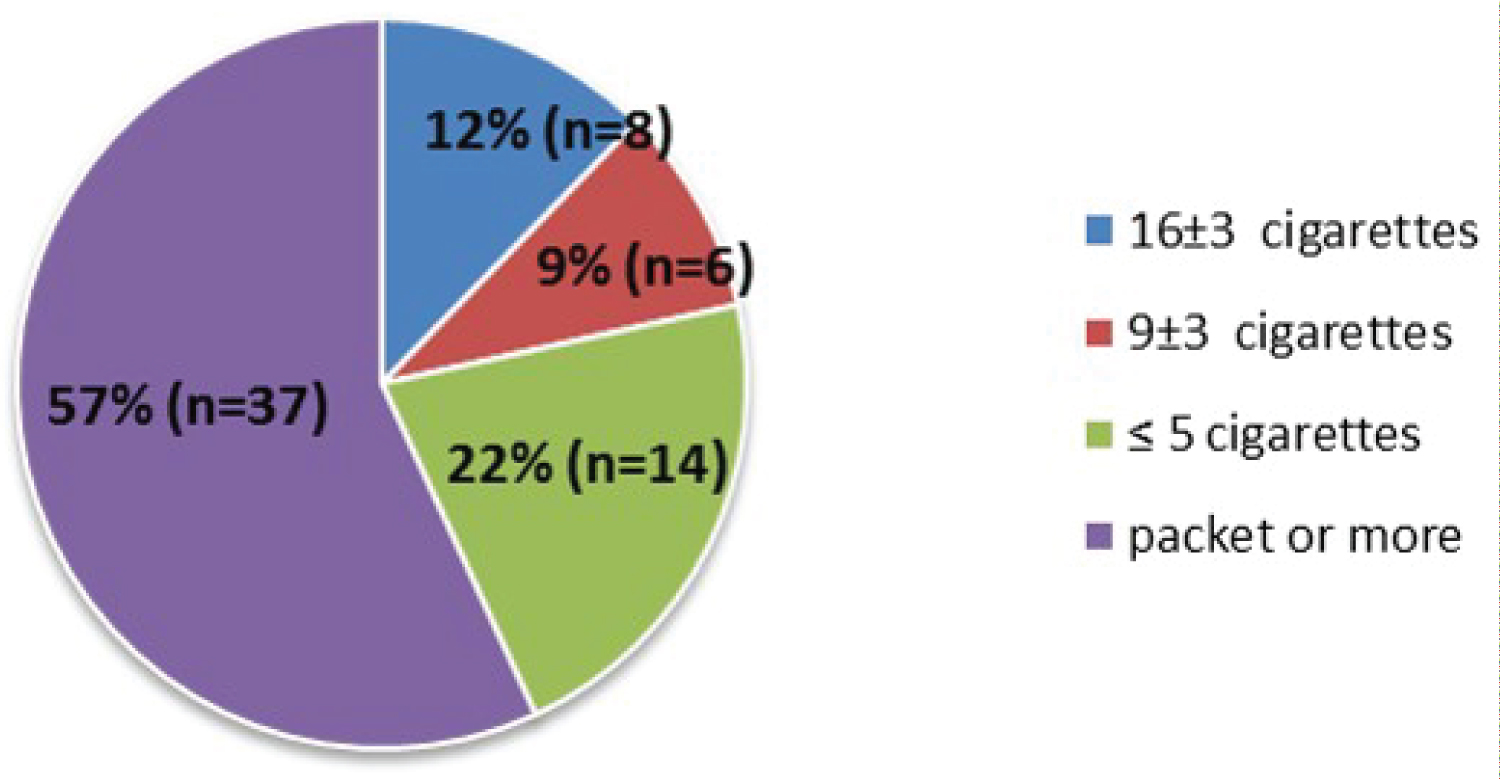 Figure 3: Amount of cigarettes smoked daily by the heart disease patients.
View Figure 3
Figure 3: Amount of cigarettes smoked daily by the heart disease patients.
View Figure 3
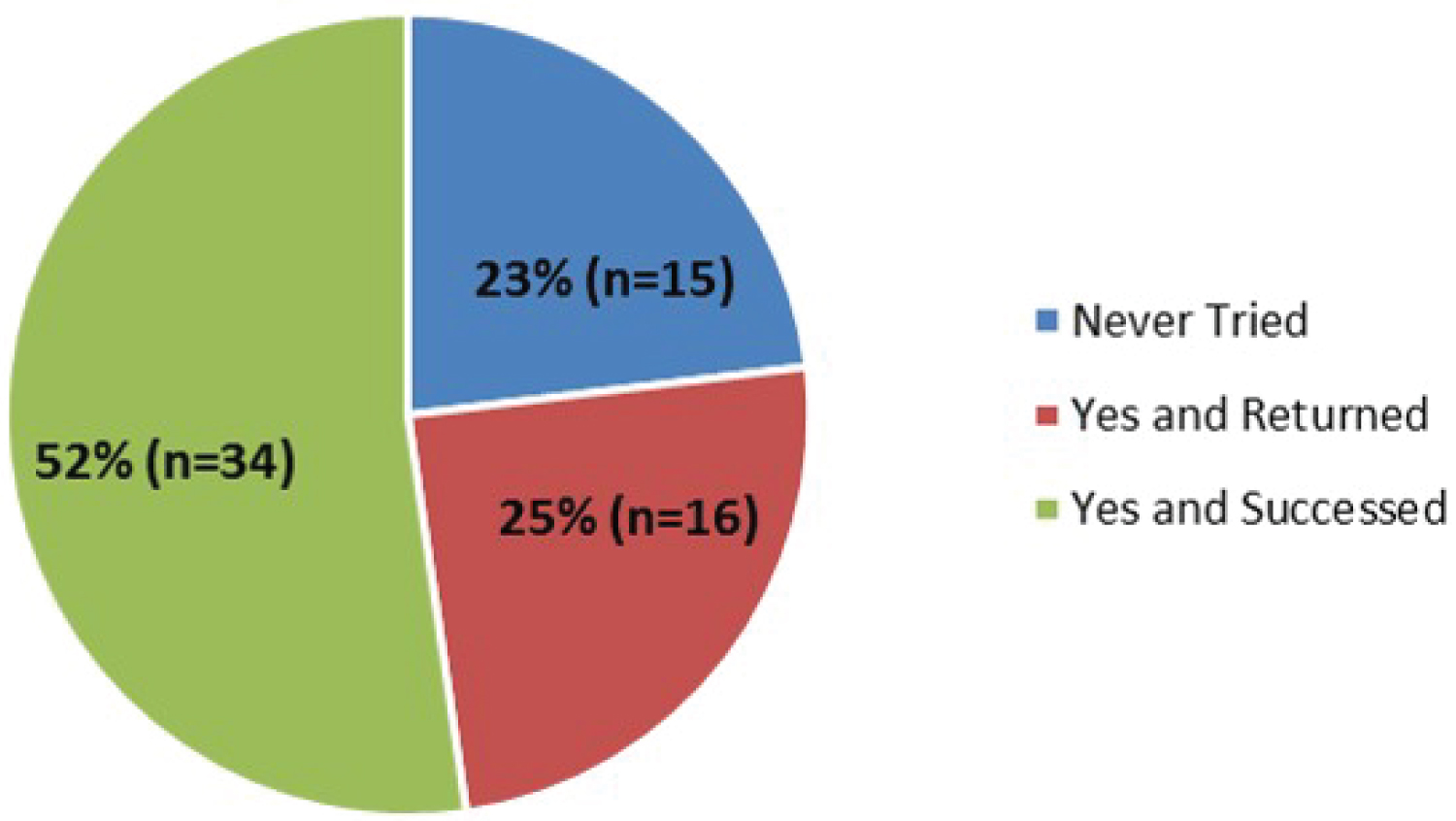 Figure 4: Willingness to quit smoking.
View Figure 4
Figure 4: Willingness to quit smoking.
View Figure 4
Regarding the patients who quit smoking (n = 34); the withdrawal symptoms during the quitting interval were, 25% (n = 22) of patients had anxiety which is the most prevalent symptom, 15% (n = 13) had headache, 13% (n = 11) had depression, 13% (n = 11) had sleep disturbance, 24% (n = 21) had not suffered from any problems and 11% (n = 10) had difficulty in quitting smoking due to environmental factors (Figure 5). Regarding the level of awareness of the availability of smoking cessation products 32.2% (n = 47) of the patients were aware of the nicotine patch, 30.2% (n = 44) of patients were aware of nicotine gum, 18.1% (n = 26) of patients were aware of nicotine lozenge, 7.4% (n = 11) of patients were aware of varIenicline) Chantix®), 1.3% (n = 2) of the patients were aware of cystisine and only 0.7% (n = 1) were aware of bupropion HCl. 10.8% (n = 4) of the quitters used smoking cessation products; where 4.6% (n = 3) used nicotine patch, 3% (n = 2) used nicotine lozenge, 1.5% (n = 1) used varenicline (Chantix®) and 1.5% (n = 1) nicotine gum (Table 2).
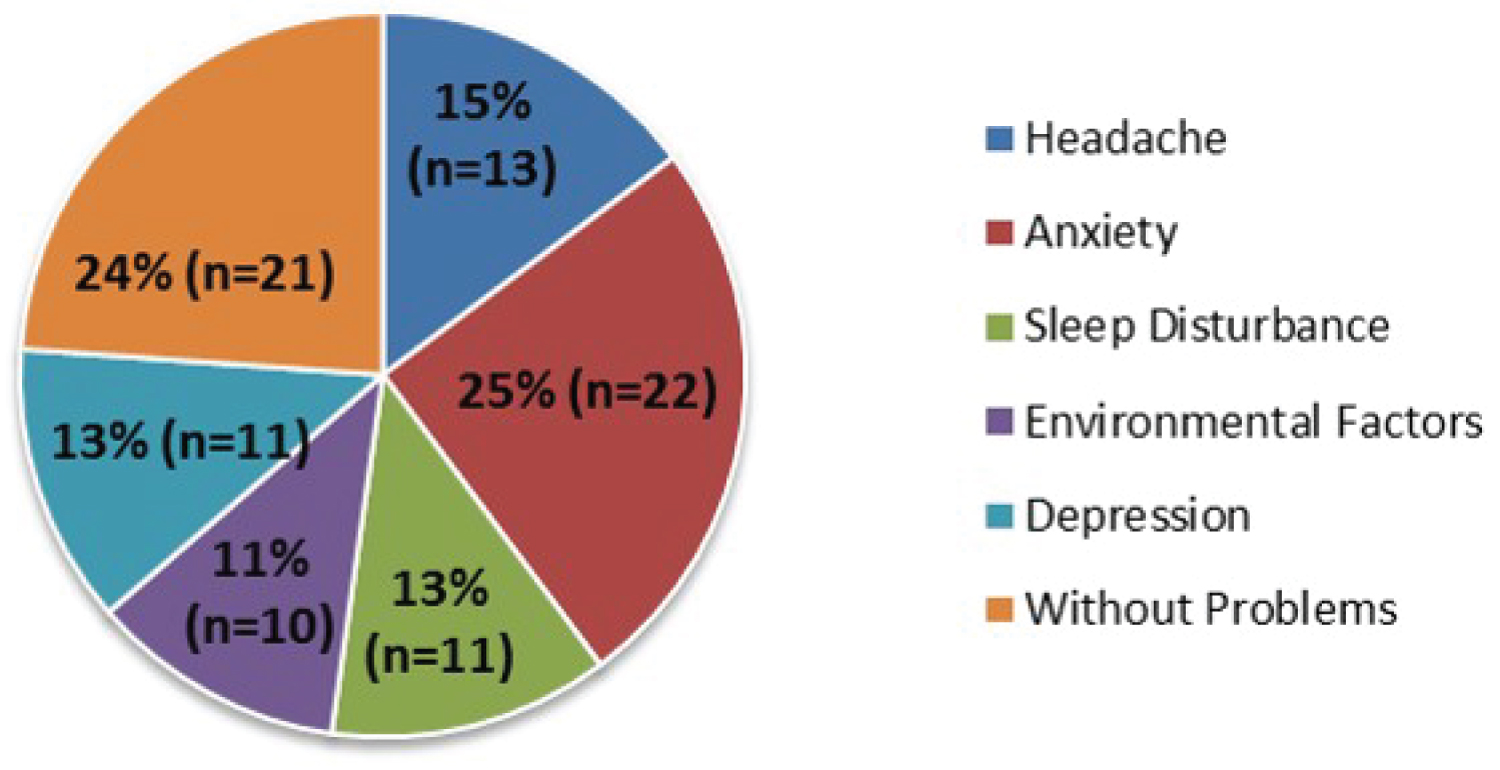 Figure 5: Withdrawal symptoms.
View Figure 5
Figure 5: Withdrawal symptoms.
View Figure 5
Table 2: The level of awareness of the availability and percentage of usage of smoking cessation aids. View Table 2
Regarding the time since they quit smoking 18% (n = 6) of the smokers quitted within 5 years ago, 61% (n = 20) quitted more than 5 years ago and 21% (n = 7) quitted in less than 1 year ago (Figure 6). The motivators for quitting smoking in 65 of the smokers (actively smoking and patients who quitted smoking) were 36% (n = 21) for self-motivation, 34% (n = 20) for physicians, 25% (n = 15) for family members and 5% (n = 3) for friends (Figure 7).
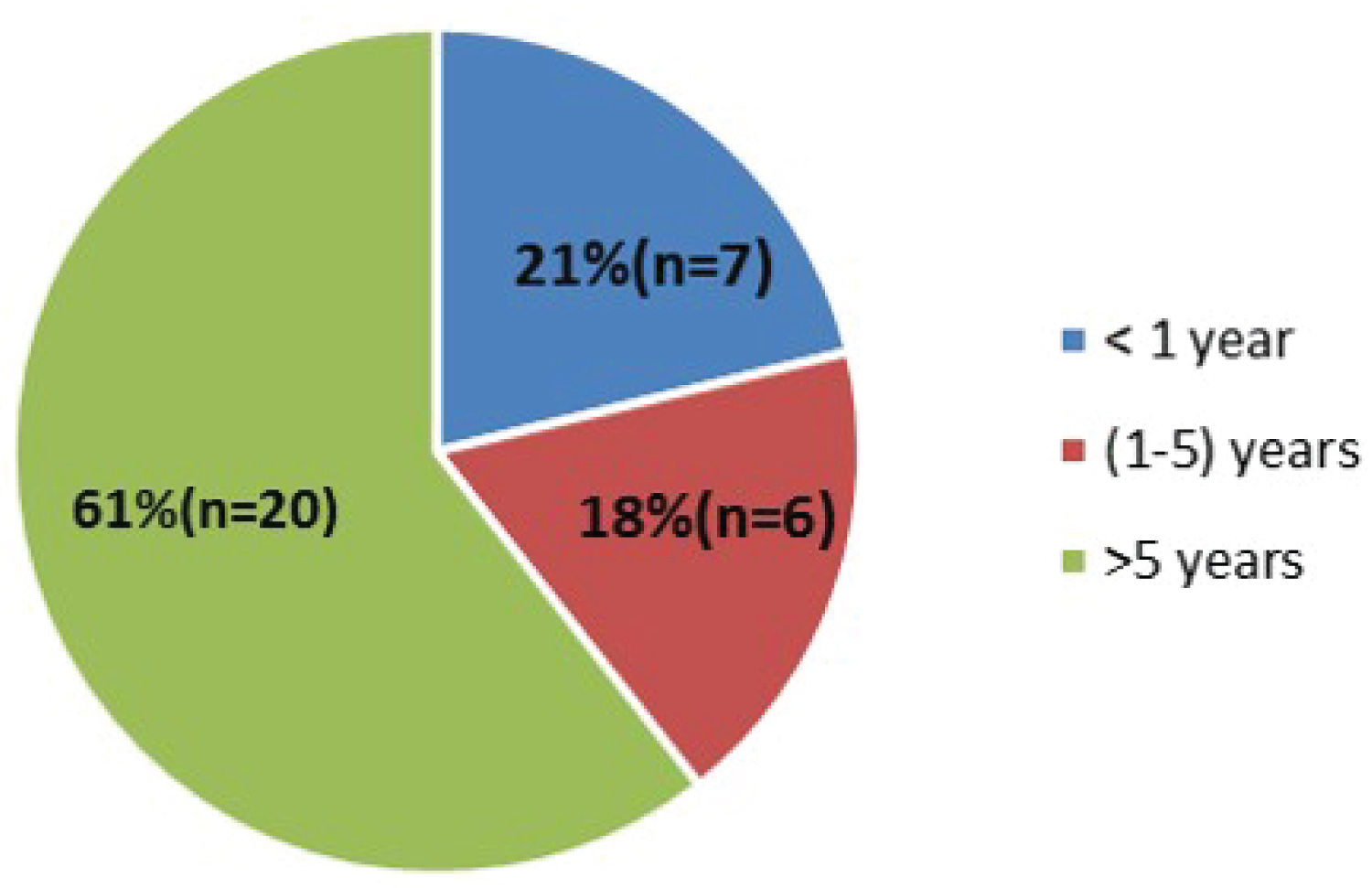 Figure 6: Time since quitting in years.
View Figure 6
Figure 6: Time since quitting in years.
View Figure 6
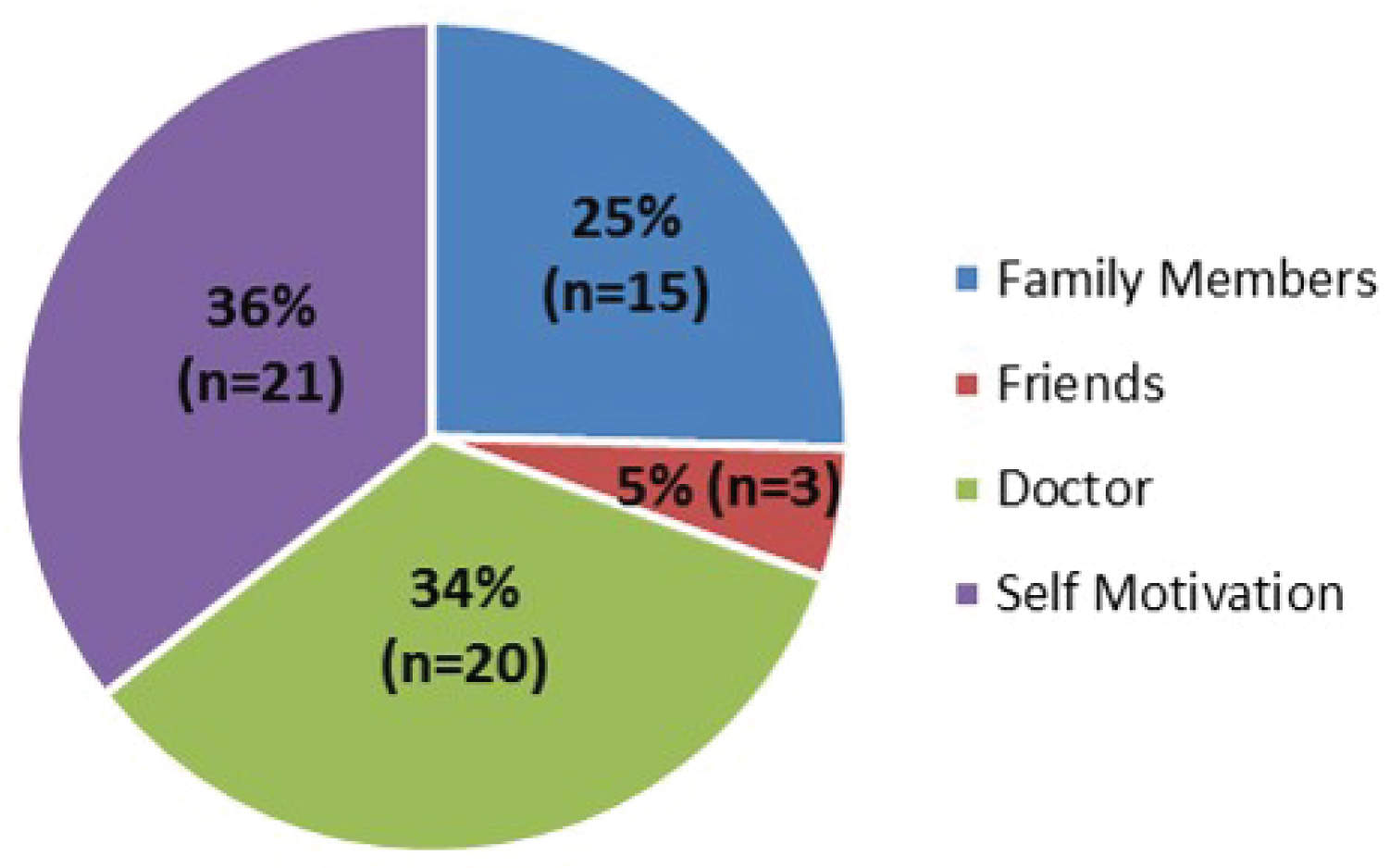 Figure 7: The motivators for quitting smoking in the 65 smokers.
View Figure 7
Figure 7: The motivators for quitting smoking in the 65 smokers.
View Figure 7
Our survey confirms some levels of unawareness of smoking cessation aids. Only 42.6% (n = 64) of the 150 heart disease patients are aware of the availability of smoking cessation pharmacotherapeutic products (Table 2).
The awareness of smoking cessation products reported in this study was compared with the results of GV Gill, et al. study about the awareness and use of smoking cessation treatments among diabetic patients (2004). The mean cigarette consumption per day was lower than our study which is 16/day.
Regarding the awareness of the medications used in smoking cessation in the GV Gill, et al. research 34% had never heard of the nicotine replacement therapy (NRT) which is Lower than our study which is 60.66% (n = 91). For bupropion; it was unknown to 46% of the patients while in our study 99.3% (n = 149) of the patients were unaware of this product. 8% of the diabetic patients had used the NHS Quitline services compared to the percentage of the heart disease smokers who visited smoking cessation clinic in our study which was 10.8% [7].
The limitations we faced during the research are limited time for data collection, small sample size and some patients refused the survey.
The poor awareness of the smoking cessation products shown in this study, suggests that strategies of support and control are urgently needed especially in heart disease patients with underline high risk.
None.
All authors have contributed to the work and manuscript writing equally.