The pericardial space is defined as the cavity between the visceral and parietal pericardium and it normally contains 10-50 mL of fluid. A pericardial effusion exists when the intrapericardial volume exceeds these limits. Any process that causes inflammation, injury, or decreased lymphatic drainage can cause a pericardial effusion. We present a rare case of recurrent pericardial effusion due to inflammation from recent diaphragmatic hernia repair.
A 52-year-old female with history of paroxysmal atrial fibrillation, hypothyroidism, depression, and gastroesophageal reflux disease was evaluated for lightheadedness and dizziness following recent diaphragmatic hernia repair. Imaging studies revealed postoperative pericardial effusion requiring pericardiocentesis and a pericardial window due to reaccumulation of pericardial fluid. Over the next several months patient had multiple hospital admission for recurrent pericardial effusion. With every hospitalization it was more evident that her pericardial effusions could be due to inflammation from her recent diaphragmatic hernia repair.
The most severe complication following diaphragmatic hernia repair is cardiac tamponade. The small distance between the diaphragm and pericardium increases risk of injury during diaphragmatic hernia repair. Increased awareness can help prevent serious complications associated with diaphragmatic hernia repair.
The pericardial space is defined as the cavity between the visceral and parietal pericardium and it normally contains 10-50 mL of fluid [1]. A pericardial effusion exists when the intra-pericardial volume exceeds these limits [1]. Pericardial effusion can be classified by pericardial separation during diastole as small (< 10 mm), moderate (10-20 mm), and severe (> 20 mm) [1,2]. Pericardial disease can develop from any pericardial disease such as pericarditis or from severe systemic disorders such as malignancies, pulmonary tuberculosis, chronic renal failure, thyroid diseases, and autoimmune disease [2]. The clinical severity of pericardial effusion can range from asymptomatic to cardiac tamponade [1]. Cardiac tamponade is a life-threatening syndrome which presents as dyspnea, tachycardia, distant heart sounds, and pulsus paradoxus [1]. The diagnosis of pericardial effusion can be made with echocardiography, computed tomography (CT), and magnetic resonance imaging (MRI), or a combination of the three. The initial treatment option is pericardiocentesis for symptomatic relief or cardiac tamponade [1]. We present a rare case of recurrent pericardial effusion following diaphragmatic hernia repair with mesh.
A 52-year-old female recently underwent symptomatic anterior diaphragmatic hernia repair due to majority of her stomach being found within her thoracic cavity at a nearby hospital. After evaluating the patient and imaging the surgeon preferred an abdominal approach compared to a thoracic approach because of his experience with the approach. The hernia repair required 0 silk suture placed in a figure eight fashion through the anterior diaphragm on each side of the hernia to the anterior abdominal wall. A Ventzio ST hernia (8 × 12) patch, an uncoated monofilament polypropylene mesh, was placed and it was fixed in place using the Ethicon secure strap in a double crown technique. Postoperatively patient developed lightheadedness and dizziness and was found to have a moderate pericardial effusion on transthoracic echocardiogram (TTE). Patient had a pericardiocentesis and 350-400 cc of dark brown pericardial fluid which was drained by vascular surgery team. The pericardial fluid analysis was nonspecific and the cultures were negative. She had reaccumulation of the pericardial fluid and a new left pleural effusion which required placement of a pericardial window. Patient presented to our emergency room three weeks later with palpitations, lightheadedness, and chest pain. She gave a past medical history of paroxysmal atrial fibrillation, hypothyroidism, depression, and gastroesophageal reflux disease. Her symptoms were similar to her previous hospitalization for pericardial effusion. Electrocardiogram (EKG) demonstrated atrial fibrillation with rapid ventricular rate. TTE and demonstrated moderate to large pericardial effusion. CT chest angiography demonstrated a large pericardial effusion (Figure 1). Patient was evaluated by both cardiothoracic surgery and vascular surgery due to recurrent pericardial effusion, she was not a candidate for reintervention due to the loculated posterior location of the effusion. Since this was a recurrent episode, within three weeks, it was recommended to transfer patient to a tertiary center for further evaluation. At the tertiary facility she was evaluated by a cardiothoracic surgeon who did not recommend any further intervention due to limited pericardial fluid to drain. Patient presented to the ER for shortness of breath and palpitations two weeks after being transferred from our facility. EKG demonstrated atrial fibrillation with rapid ventricular response. TTE demonstrated pericardial effusion and left sided pleural effusion. Patient required a diltiazem drip and was switched from home medication sotalol to flecainide to achieve rate control. Patient was reevaluated by vascular surgery who had no further recommendations on management. She was also evaluated by general surgery because her recurrent pericardial effusion started following her diaphragmatic hernia repair. It was determined that her recurrent pericardial effusion is due to reactive inflammation from tackers used to secure the mesh and it will improve as the inflammation resolves. Patient returned to the ER two weeks later complaining of chest pain, headache, and shortness of breath. Vitals were temperature: 98.2 F, blood pressure: 101/63 mmHg, heart rate: 117 beats per minute, respiratory rate: 24 breaths per minute, oxygen saturation: 97%. Patient appeared in no acute distress. EKG demonstrated atrial fibrillation with rapid ventricular rate. She was started on diltiazem drip and her flecainide was stopped due to side effects. Patient’s allergies to beta blocker and amiodarone made it challenging to achieve rate control. She converted to sinus rhythm with rate control and was switched from intravenous to oral diltiazem. Digoxin was added to maintain rate control. CT chest with contrast demonstrated a left sided pericardial effusion (Figure 2). Patient was evaluated by vascular surgery and general surgery again. They decided the patient would require a pericardial window and removal of the mesh if she continued to have recurrent pericardial effusions. Cardiothoracic surgery recommended that patient be evaluated at a larger facility for repeat pericardial window. Patient was transferred to a tertiary facility and was evaluated for a CT-guided pericardiocentesis. Due to improvement of her symptoms, the CT-guided percardiocentesis was not performed and she was discharged home. Patient was advised to follow up with cardiology outpatient.
 Figure 1: CT chest angiography, large pericardial effusion measuring up to 3 cm thickness.
View Figure 1
Figure 1: CT chest angiography, large pericardial effusion measuring up to 3 cm thickness.
View Figure 1
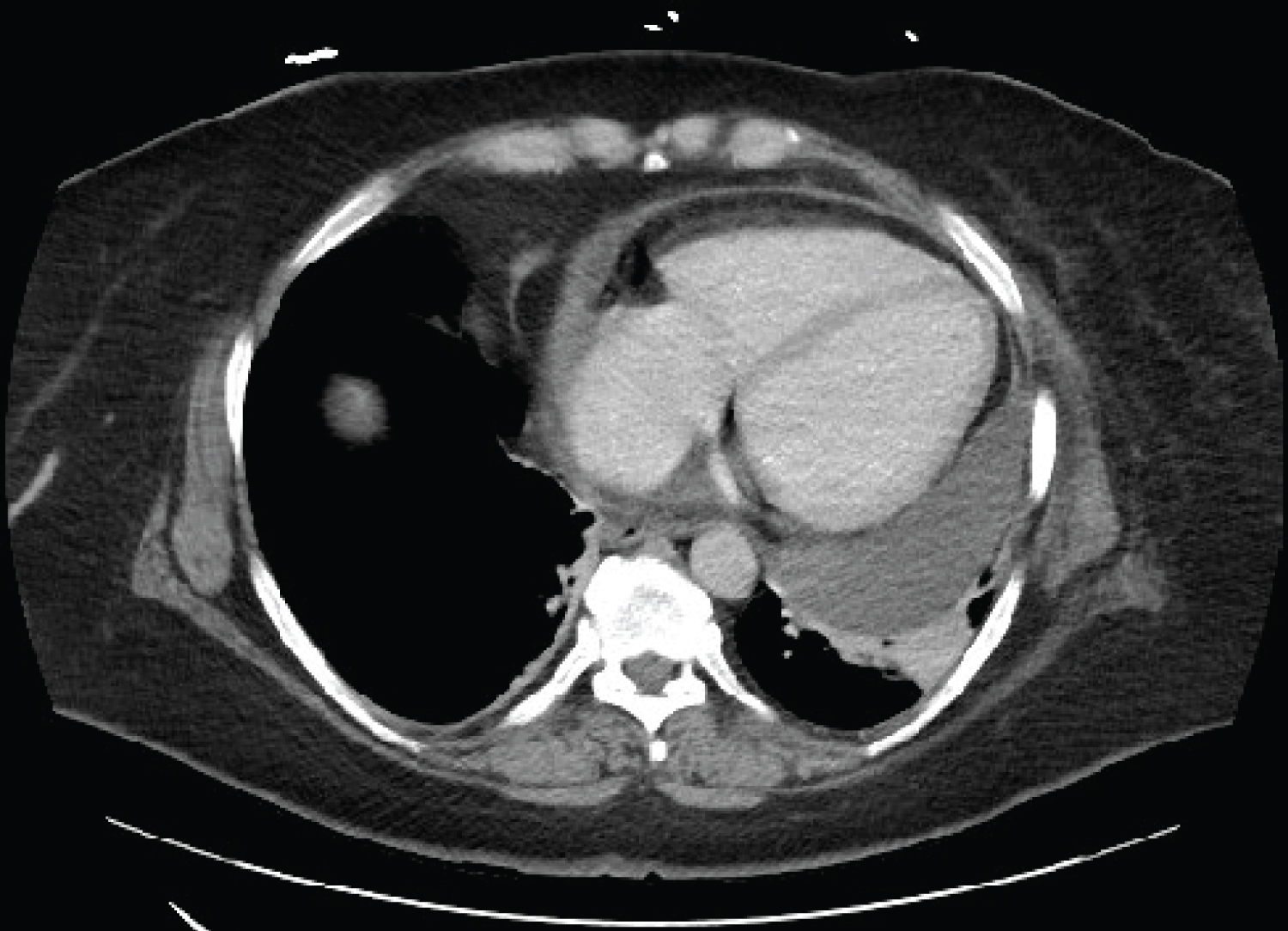 Figure 2: CT chest with contrast, large left-sided pericardial effusion measuring up to 3.2 cm thickness.
View Figure 2
Figure 2: CT chest with contrast, large left-sided pericardial effusion measuring up to 3.2 cm thickness.
View Figure 2
Pericardial effusion can be an incidental finding or a life threatening emergency such as cardiac tamponade. It is a common clinical finding with an incidence and prevalence in a tertiary echocardiography lab as high as 3-9% [1,3]. Echocardiography is recommended in patients suspected of pericardial effusion because it is sensitive, specific, noninvasive, and available at bedside [2,3]. Our patient had recurrent pericardial effusions due to inflammation from diaphragmatic hernia repair. The inflammation was caused by tackers used to hold the surgical mesh in place. The type of mesh used and silk sutures may have contributed to the recurrent pericardial effusion but the tackers were the main cause. We believe the tackers were responsible because the pericardial effusions stopped after they were possibly absorbed without any surgical intervention. A previous study discussed how the small distance between the diaphragm and pericardium increases the risk of injury from sutures or staples placed below the diaphragm [4]. Literature review shows cardiac complications commonly occurring after fundoplication surgery and even more frequently after diaphragmatic hernia repair, cardiac tamponade being the most serious complication [5]. Iatrogenic cardiac tamponade (ICT) has been reported following open and laparoscopic approach. Caliko, et al. identified 30 ICT cases with 10 deaths (overall mortality rate of 33%) following peri-hiatal hernia repair [6]. They reported mortality rates due to ICT following an anti-reflux/hiatoplasty (27.3%), diaphragmatic hernia (33.3%), and ventral hernia (75%) [5]. Graft fixation and helical tacks were the main offenders of ICT [6]. Majority of the ICT are caused by injury to the diaphragmatic dome, anterior to hiatus [6]. It is best to avoid graft fixation around the anterior-hiatal diaphragmatic dome and if absolutely necessary meticulous stitching is preferred over fixators [6]. Tackers manufacturers in 2004 and 2011 discouraged use on surfaces > 4 mm and contraindicated their use on the diaphragm near the pericardium [6-9]. Despite manufacturers recommendations it can be very tempting to use tackers in complex hernia repairs to prevent recurrence. Our patient had a severe diaphragmatic hernia with majority of her stomach being located within the thoracic cavity. The severity of the hernia may have led to the surgeon using a more aggressive approach to prevent recurrence. Persistent hypotension during or following a peri-hiatal repair is the most common and alarming sign of ICT [6]. In majority of the cases the pericardial effusion or cardiac tamponade resolved following pericardiocentesis or surgical intervention. Our patient continued to have recurrent pericardial effusions after her surgery despite multiple interventions. The presentation of the pericardial effusions following the surgery made chronic medical conditions such as atrial fibrillation or hypothyroidism very unlikely as the cause of the recurrent pericardial effusion. Our analysis of the pericardial effusion was nonspecific but previous studies have suggested that parameters such as protein, LDH, glucose, WBC, RBC rarely help in identifying the etiology of the pericardial effusion; Light’s criteria is not very reliable in differentiating exudative from transudative pericardial effusions [10,11]. Management of our patient became more challenging due to her recurrent atrial fibrillation with rapid ventricular rate. Her recurrent atrial fibrillation with rapid ventricular rate was most likely secondary to her recurrent pericardial effusion. Acute inflammation from the tacks can lead to atrial fibrillation, which can be exacerbated by the pericardial effusion. Patient’s allergies to rate control medication along with her recurrent pericardial effusion and atrial fibrillation with rapid ventricular rate provided a unique challenge in her management.
Pericardial effusion and cardiac tamponade are rare complications of diaphragmatic hernia repair with the risk further reduced with proper surgical technique. The increased number of incidents and risk of extreme mortality in a low risk procedure such as hernia repair makes prevention very important. Increased awareness of physicians is important to prevent complications and improve mortality after peri-hiatal hernia repair.
N/A.
No conflict of interest to report.
No funding to report.
The patient provided informed consent.
This research was supported in part by HCA Healthcare and/or an HCA Healthcare affiliated entity. The views expressed in this publication represent those of the author(s) and do not necessarily represent the official views of HCA Healthcare or any of its affiliated entities.