Meticulous documentation in clinical records has been shown to improve patient care and clinician performance. Conversely, poor documentation is associated with an increased risk of adverse events. The Royal College of Surgeons (RCS) issues guidance on the contents of surgical admissions documentation.
Audit highlighted frequent omission of key criteria set out by RCS with freehand documentation. We set out to design, implement, and evaluate an orthopaedic admission proforma for our trauma patient population.
Retrospective analysis was performed of freehand clerk-ins against RCS standards. A new orthopaedic admission document was designed, and after an introductory period further retrospective analysis was performed of document clerk-ins with statistical analysis performed.
80 freehand records and 64 Admission documents were analysed. Use of proforma increased documentation in 29 out of 32 criteria set by RCS. This was statistically significant in 22 out of 29 criteria.
Documentation of patient information is significantly improved with use of an admission document. Clerk- in quality is more consistent and comprehensive and is a quick and accessible source of information for all members of the multidisciplinary team. We have designed an effective admission document that is reproducible and an auditable tool that would benefit a range of surgical specialties and unit sizes.
Surgical Admissions, Documentation, Proforma, Orthopaedics, Trauma
Meticulous documentation of patient information cannot be overstated and is a cornerstone of good clinical practice. Poor quality documentation is associated with a higher rate of adverse events 1], and clear and accurate documentation is linked with improved patient care and clinician performance [2].
Clear and comprehensive documentation must thus start from the moment a patient is admitted to hospital. There is good evidence to suggest that printed admissions documents aid this and have been shown to be preferred in surgery [3,4] and medicine alike [5-8] over unprompted 'freehand' documentation. They have been shown to improve data retrieval time and with pointed headings act as an aide-memoire, which is of benefit to any medical or nursing professional given the time pressures and large number of tasks that contribute to a typical shift [6,9].
If we consider medicolegal ramifications, more complete recording of patient information is more likely to prevent adverse events [10]. In a typically busy surgical environment where time is scarce and patient management is often decided in short time frames, comprehensive and accessible patient documentation can prevent a patient coming to harm and avoid significant consequences facing both the responsible medical individual and service.
The Royal College of Surgeons of England (RCS) issues guidance on admission documentation and what it should contain [11]. It advises inclusion of 32 key criteria that should be documented in the admission of a surgical patient (Table 1).
Table 1: Royal College of Surgeons Criteria for Documentation. View Table 1
The Authors work in a busy tertiary trauma unit serving a population of 1.1 million, and in one of the largest health boards in the United Kingdom [12]. Previous admission policy for patients admitted to the unit involved 'freehand' clerk ins. There was widespread variability in the completeness and quality of freehand clerk-in documentation. The authors felt that there was a need for change and desire for a document that would establish itself as the status quo for departmental admission practice.
Furthermore, literature review revealed that there is evidence to suggest the use of proformas in aiding data recording in orthopaedic operation note writing [13,14]. There is a paucity in the literature on comparison between freehand and admission documentation being attempted in a tertiary centre with orthopaedic patients. We therefore set out to assess whether an admission document would improve the recording of patient information according to RCS standards.
Retrospective analysis of freehand clerk-ins for trauma admissions over a two-week period against the 32 RCS criteria was performed by a single author. A new admission document was then designed and produced by the authors using RCS criteria and with further input from members of the multidisciplinary team. Final approval by departmental seniors in accordance with hospital policy was confirmed. There was uniform agreement no freehand clerk-ins would be performed for trauma patient admissions to the unit once the document was introduced. Supplementary Material.
After a period of education about the document and its introduction, further retrospective analysis of clerk-ins using the admission document was performed over a two-week period against RCS guidelines, again by a single author. Inclusion criteria included all trauma patients admitted to the unit in that period. Exclusion criteria included clerk-ins by authors. In both evaluation cycles on-call teams completing admission documentation were unaware that they were being audited. The audit period was chosen at random and included every trauma patient admitted within the period on a consecutive, chronological basis.
Statistical analysis was performed with Fisher's Exact test using SPSS© software with a P-value of < 0.05 deemed statistically significant.
Eighty freehand clerk-ins and Sixty-Four clerk-ins using the admission document were evaluated. There was total compliance with admission document use following its introduction Table 2 and Figure 1.
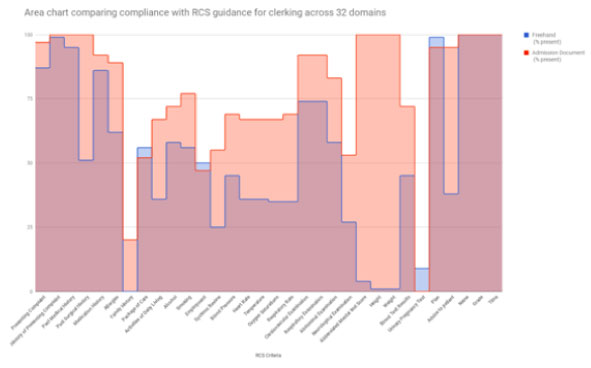 Figure 1: Area Chart comparing compliance between freehand and admission document clerk ins across 32 domains.
View Figure 1
Figure 1: Area Chart comparing compliance between freehand and admission document clerk ins across 32 domains.
View Figure 1
Table 2: Results of freehand clerk-ins against the admission document. View Table 2
In all, Documentation improved in 29 out of 32 criteria, 21 of which were statistically significant. 11 out of 13 criteria in history taking saw an improvement using the admission document, the largest increases including past surgical history (51% against 100%), allergies (62% v 89%), and family history (0% v 100%). Of the 11 improvements in criteria, seven were statistically significant (p < 0.001): Presenting complaint, Past Surgical History, Allergies, Family History, Alcohol intake, Smoking status, and systems review. Recording of employment and package of care status did not see an improvement with the use of the admission document.
Of aspects recorded from clinical examination, all basic observations of blood pressure, heart rate, temperature, oxygen saturations, and respiratory rate resulted in an improvement with the admission document, all of which were statistically significant. Recording of examinations including cardiovascular, respiratory, abdominal, and neurological systems all saw statistically significant improvements and all patients had an Abbreviated Mental Test performed in the admission document cohort compared with just 4% of freehand clerk-ins, which is of particular benefit in the orthopaedic hip fracture patient populous. Documentation of height and weight both saw improvements of 100% recording in admission document against 1% apiece in the freehand cohort. This was significant p < 0.001.
The admission document improved recording of blood test results 72% compared with 45% of freehand clerk ins (p < 0.001). The clerk in document did not show an improvement in recording pregnancy test results with 9% freehand versus 0% in the admission document, however this is a likely consequence of the infrequent use of the test.
Administrative aspects of documentation; name and grade of clerking doctor, time of clerk-in, and recording of a plan was consistently done well in both freehand and admission document clerk-ins with 100% inclusion in both. Documented advice to patients saws a significant improvement from 38% freehand to 95% with the admission document. Recording of a plan was performed in 99% freehand clerk ins compared with 95% in the admission document cohort.
Our results have shown recording of patient information on admission to our unit is significantly superior with the application of a dedicated admission document. Its implementation has been positively received by the unit and wider ranging medical and nursing professionals. The objective results match that of previous studies [2,3] that highlight admission documents can improve recording patient information in both medical and surgical patients. Whilst Faraj, et al. explored the use of an admissions proforma for elderly trauma patients, not based on RCS guidance but designed according to the departmental needs of a regional unit [4], this is the first to describe its use and success in a major trauma centre. Our results are an advance on previous studies [2,3]. Using RCS guidance, with more improvements in criteria recording and more statistically significant results in our orthopaedic admission document.
The quality of clerk-ins was more thorough and consistent. Key criteria saw an improvement in documentation as colleagues were prompted by the flowing and comprehensive design, which in support of previous studies can act as an aide memoire [6]. Furthermore, it acts as a beacon of readily available, comprehensive information for members of the MDT including, but not exhaustive to Anaesthetists, Physiotherapists and Occupational therapists, and retrieval of information using the document can be performed with ease and is quicker than sifting through single pieces of freehand notes.
The admission document is readily auditable and easily changed if the need arises or guidance makes for further recommendations.
A limitation our study lies in that although colloquial feedback of the new admission document was well received and positive, Questionnaires to MDT colleagues and doctors using the document would have been of benefit in subjectively supporting our findings in comparing the two forms of clerk-ins. However, it would be elementary to audit the document in the future and include a subjective questionnaire.
We have shown that a new admission document can be successfully implemented with profound results. The document is a focus for a wealth of vital patient information that should be included in all admissions, and acts to streamline the search for patient information that is of benefit to a variety of medical and nursing professionals during the pre, peri, and postoperative chapters of patient admissions.
We believe our work is easily reproducible, and although designed for orthopaedic patients, would be of benefit to a range of surgical specialties and in departments of varying size and pressures.
The authors declare that they have no conflict of interest.
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sector.
This article does not contain any studies with human participants or animals performed by any of the authors.
Trauma Admission Document.