Introduction: Fractures of the zygomatic arch are responsible for anatomical changes with functional and aesthetic repercussions. Diagnosis is clinical and paraclinical. The aim of this study was to determine the epidemiological, clinical and scanographic aspects of these fractures.
Patients and methods: This was a retrospective, descriptive, analytical, cross-sectional, monocentric study conducted from 2016 to 2022, covering zygomatic arch fractures admitted to the Department of Stomatology and Maxillofacial Surgery. All radiologically confirmed zygomatic arch fractures were included. Patients with incomplete records and facial fractures without zygomatic arch fractures were excluded. Fracture features were classified according to the Özyazgan and Jung classifications. The following parameters were studied: age, sex, profession, mode of recruitment, etiology, mechanism, time to consultation, functional and physical signs, CT findings.
Results: 44 cases were collected. The mean age was 34 ± 12.9 years. Men accounted for 84% of cases. 59% of patients came from the emergency department. MVA was observed in 60% of cases, and the mechanism was direct in 88%. Trismus was found in 93.2%, facial pain in 95.5%, facial asymmetry in 98% and preauricular depression in 75%. CT scans were performed in 100% of cases, combined zygomatic arch fractures accounted for 82% and isolated fractures for 8%.
Conclusion: Fractures of the zygomatic arch are frequent, affecting young males. Road accidents are the main etiology. Limited mouth opening and preauricular depression are the signs of appeal. CT is the reference examination.
Fracture, Zygomatic arch, Epidemiology, Diagnosis, CT scan
The zygomatic arch is a long, thin, cylindrical bridge-like bony structure which plays a major role as a lateral bumper for the face [1]. As a result, it is frequently subject to maxillofacial trauma, leading to bone continuity fractures. These fractures are generally the result of high and low speed forces or impacts on the lateral part of the face [2].
Fractures of the zygomatic arch are common in young males, and road accidents are the main cause of these fractures [3]. Zygomatic arch fractures frequently occur as part of zygomatico-maxillary complex fractures, which account for around 25% of all facial fractures, but isolated zygomatic arch fractures account for 10% of all malar fractures and 5% of all facial fractures [4,5].
Diagnosis is straightforward, suspected clinically in the presence of post-traumatic facial asymmetry, and confirmed by maxillofacial computed tomography (CT), which is then used to search for associated lesions and the characteristics of the fracture line. For certain complex fractures, CT is taking on an increasingly important role as a means of better assessment [6-8].
The aim of this study was to determine the clinical and CT aspects of zygomatic arch fractures at Owendo University Hospital.
This was a retrospective, descriptive, analytical, cross-sectional, monocentric study conducted over a period of 06 years, covering all maxillofacial trauma patients with a fracture of the zygomatic arch who were admitted Department of Stomatology and Maxillofacial Surgery at the Centre Hospitalier Universitaire d'Owendo (CHUO). All radiologically confirmed cases of zygomatic arch fractures hospitalized in the department and with a complete file were included. Patients with incomplete records were not included in our study. Patients with maxillofacial trauma without CT fracture of the zygomatic arch.
In our study, we used two classifications. The classification of zygomatic arch fractures proposed by Özyazgan, et al. [9], and the classification of isolated zygomatic arch fractures proposed by JUNG, et al. [10].
Data were collected on a form from: Hospitalization records, consultation and hospitalization registers, and from the operating theatre intervention register.
The parameters studied were: Age, sex, profession, mode of recruitment, etiology, mechanism, consultation time, functional and physical signs, CT scan results.
Data analysis was performed using SPSS (Statistical Package for the Social Sciences) version 23 and Word and Excel 2019 software. Qualitative variables were expressed as effectives and percentages, and quantitative variables as means, minima and maxima. The association between certain variables was analyzed using the chi-square test with Yates correction and was deemed statistically significant for a value of P < 0.5.
Our search engines were: Pub Med, Google scholar, RefSeek, National Library of Medicine (NLM).
44 patients were enrolled during the study period. The mean age was 34 ± 12.9 years, with extremes of 13 and 68 years. There were 37 men (84.08%) and 7 women (16%).
Employees represented 50% of cases, the unemployed 22% of patients, students/pupils 22% of cases and retired people 6% of cases. 59.1% of cases came from the CHUO emergency department (Figure 1). There were no cases in June (Figure 2). Public road accidents caused 59.1% of fractures, domestic accidents 16%, fights/aggressions 13.41% and work-related accidents 7%. The mechanism of RTA was auto-pedestrian in 57.6% of cases and auto-auto in 27% (Table 1).
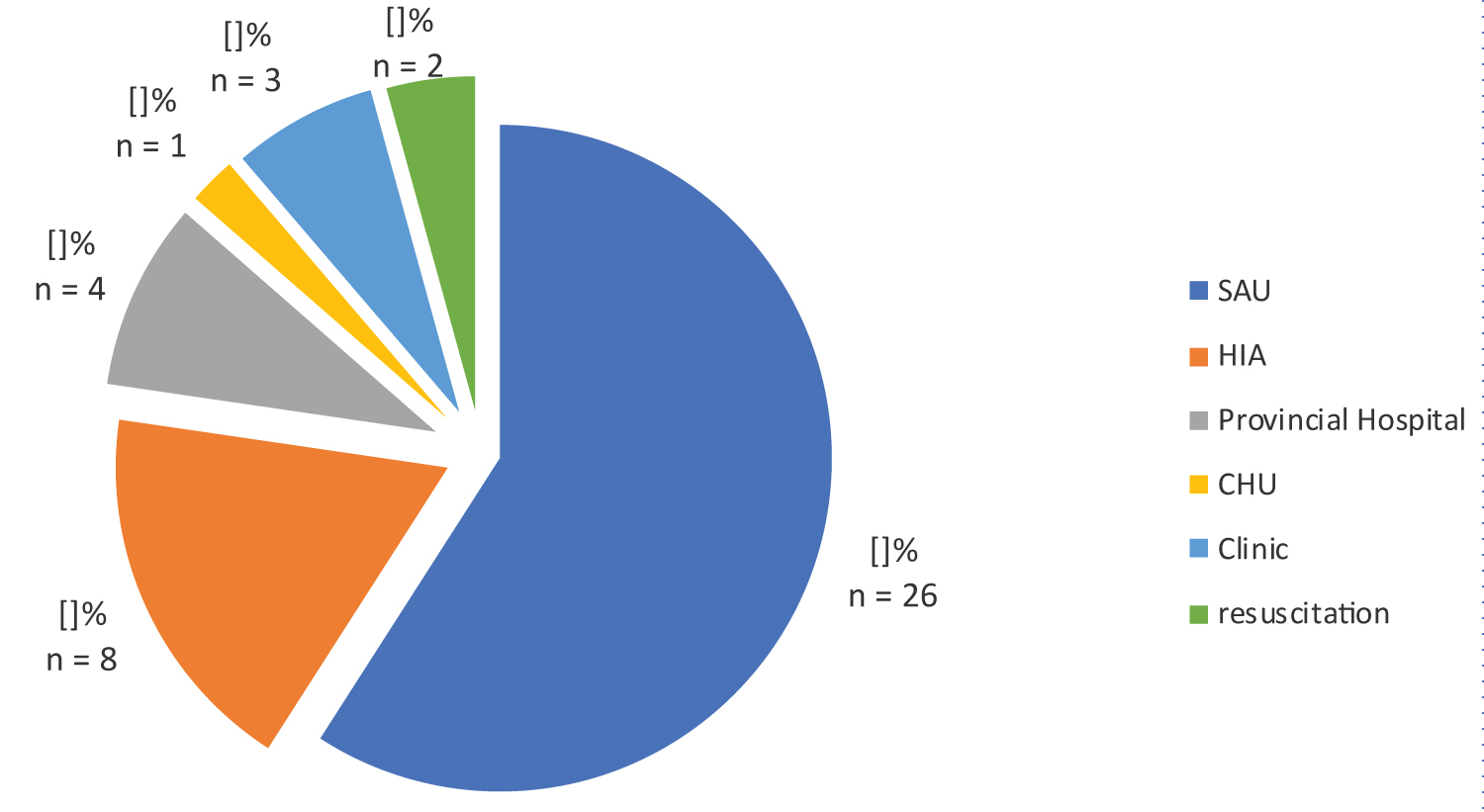 Figure 1: Patient recruitment method.
View Figure 1
Figure 1: Patient recruitment method.
View Figure 1
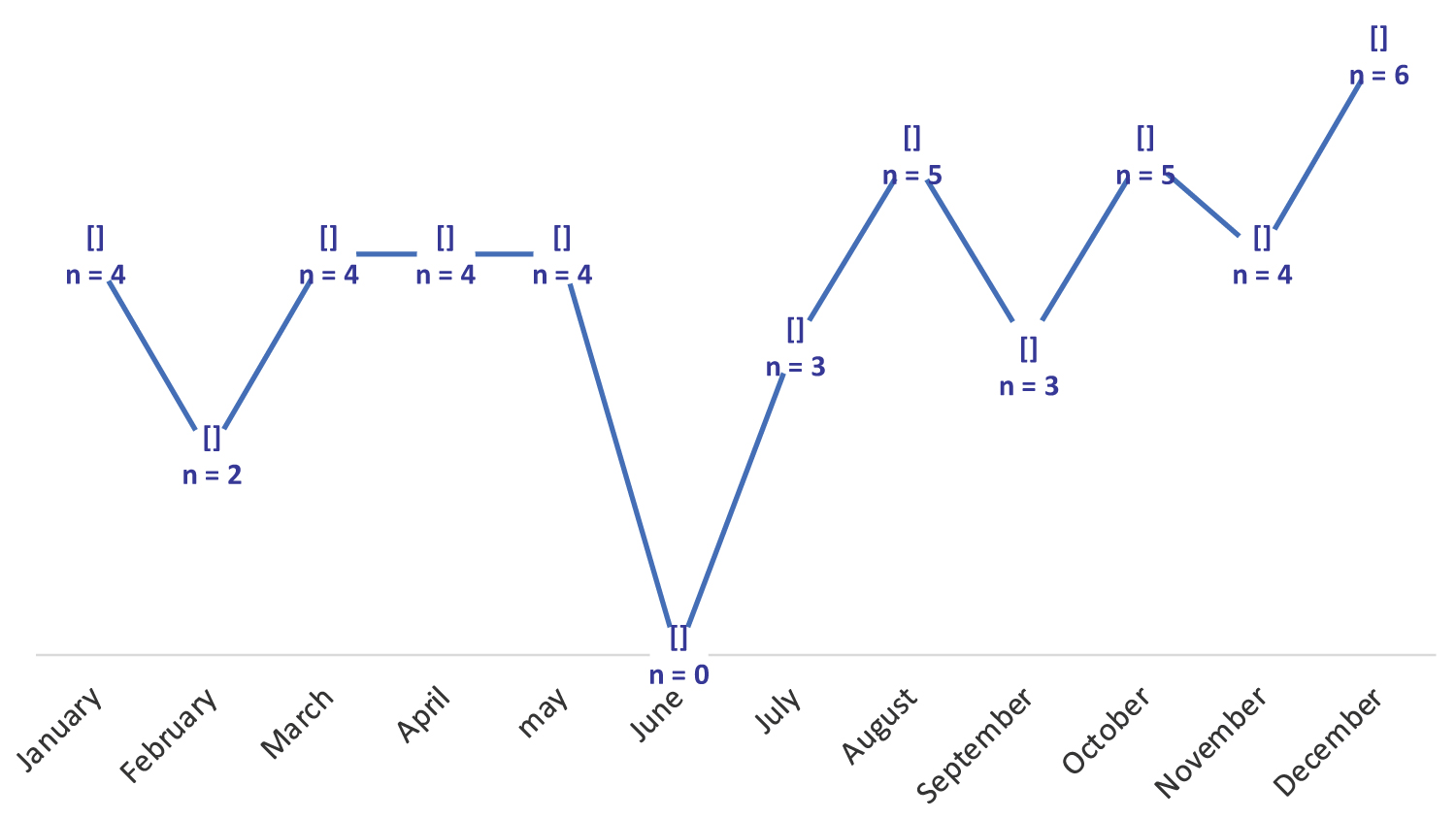 Figure 2: Monthly patient distribution.
View Figure 2
Figure 2: Monthly patient distribution.
View Figure 2
Table 1: Breakdown of patients by MVA mechanism. View Table 1
38.63% of cases consulted a doctor within the first six hours of trauma (Figure 3). Facial pain was present in 95.5% of cases, and opening limitation was observed in 93.5% of patients (Figure 4). Facial asymmetry (88.1% of cases), preauricular depression (75.0% of cases) and exquisite pain (84.1% of cases) were the most frequent clinical signs (Table 2).
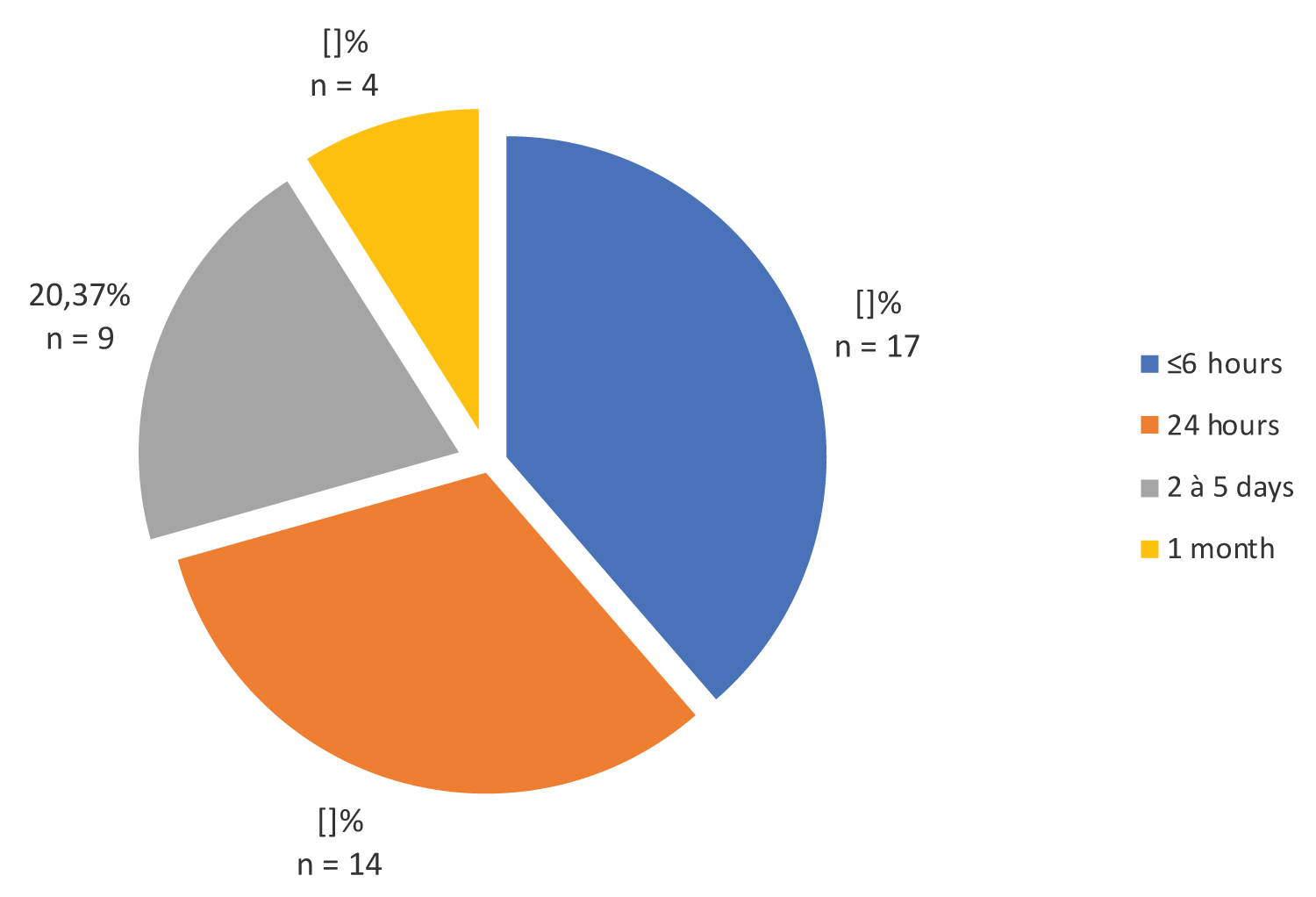 Figure 3: Breakdown of patients by length of consultation.
View Figure 3
Figure 3: Breakdown of patients by length of consultation.
View Figure 3
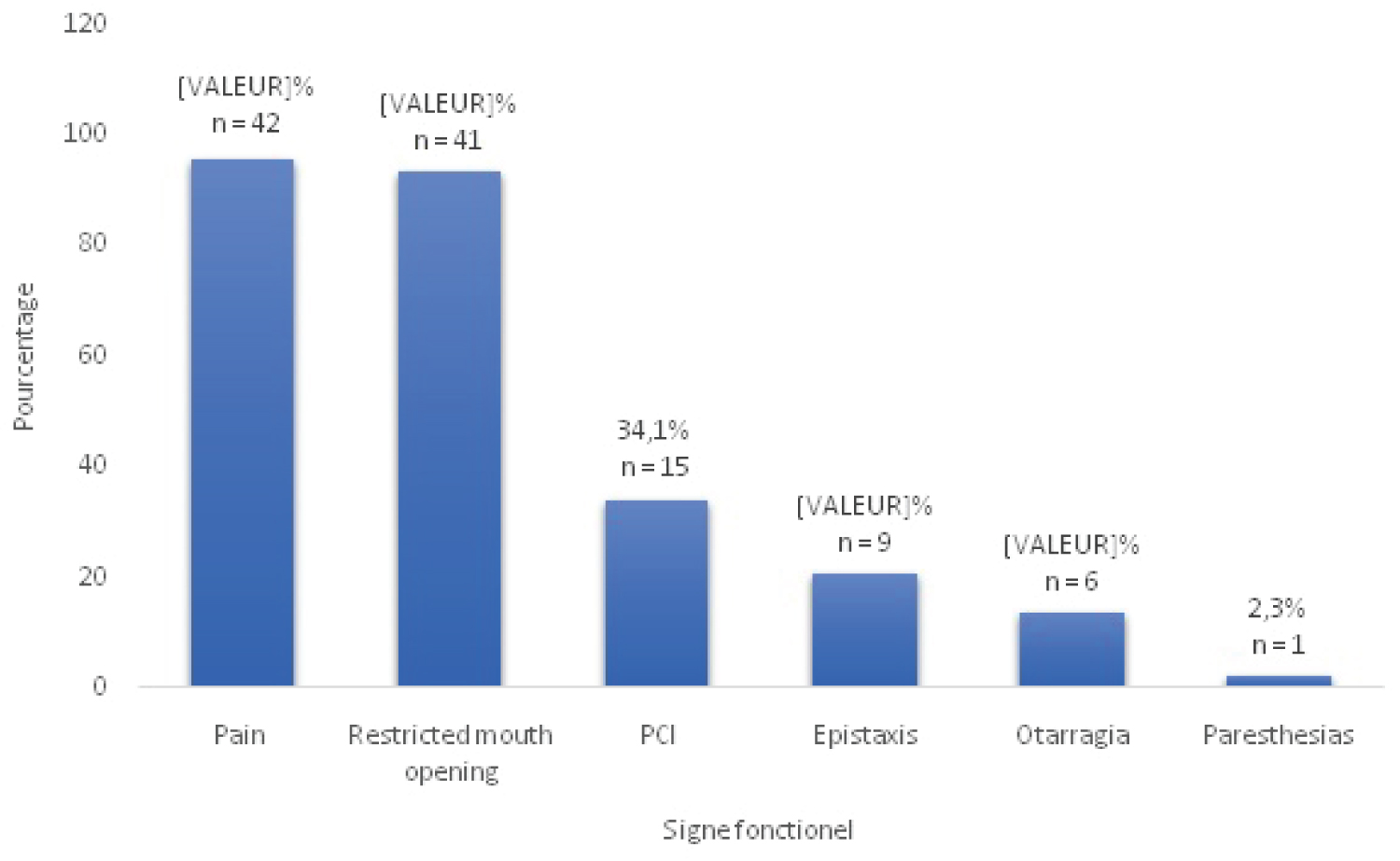 Figure 4: Distribution of patients' functional signs.
View Figure 4
Figure 4: Distribution of patients' functional signs.
View Figure 4
Table 2: Distribution of patients according to physical signs. View Table 2
CT scans were performed in 100% of cases. Combined zygomatic arch fractures accounted for 82% of cases, and isolated zygomatic arch fractures for 18%.
Subtype IV isolated zygomatic arch fractures accounted for 37.5% of cases (Table 3). The fracture line was located on the right in 52.3% of cases, on the left in 31.8% and bilateral in --16%.
Table 3: Distribution of patients according to subtype of isolated zygomatic arch fractures. View Table 3
Tegument involvement accounted for 81.81% of associated lesions (Table 4).
Table 4: Distribution of patients according to associated facial lesions. View Table 4
Fractures of the zygomatic arch mainly concern young subjects, with an average age of 34 ± 12.9 years, which is in line with the work of Kim J, et al. [11] and Sanago S, et al. [12], in which the average age is 26 years, or Cho J, et al. [13].
The male population is the most affected by these fractures, as reported in the study by Jung S, et al. [10] with a sex ratio of 4, and that by Sanogo S, et al. with a sex ratio of 3 [12].
This average age and male predominance can be explained by the fact that the country's population is very young and engages in physical and violent activities.
In a third of cases, patients were transported by ambulance. This demonstrates the poor communication in the care of trauma victims at the scene of the accident, and the difficulty the population has in reaching emergency units in our country.
In terms of monthly trauma frequency, December and, to a lesser extent, August and October are the most accident-prone months. This corresponds to the period of social unrest and large-scale crowd movements.
In the vast majority of cases, the impact is direct, reflecting the zygomatic arch's exposure to violent contact and its role as a lateral shock absorber for the face.
In this study, the dominant etiology was a public road accident, which confirms the work of Kim J, et al. [11], Orabona, et al. [14], Sanago S, et al. [12], but contradicts the studies of Czerwinski M, et al. [2] where brawls and assaults are the dominant etiologies. This contrast can be explained by the quality of the road network and the lack of respect for the rules of the road in our country. However, a study carried out in the city of Montreal shows a 50% rate of zygomatic arch fractures following fights and assaults, demonstrating the opposite.
The average consultation time in our series was 2 to 3 days, i.e. 38.63% of cases. Our data contrast with those of Diallo, et al. in Mali, where most patients (66.2%) consulted on the day of the trauma. This difference can be explained by the fact that, in our context, patients first stay in the ICU or intensive care unit before consulting the stomatology and maxillofacial surgery department of the CHUO.
Mouth opening limitation and facial pain were the main functional signs, with frequencies in excess of 90%. Our data corroborate those of Do Santos Zounon, et al. and Moussa, et al. where these functional signs account for over 90% [12,15].
Morphologically, facial asymmetry and preauricular depression were the main signs, with frequencies of over 80%. Our results corroborate those of literature, such as Jung S, et al. Rosselo, et al. Kim J, et al. where these morphological signs are in the foreground [10,11,16].
Diagnosis of zygomatic arch fractures always requires CT scanning, as shown in the studies by Jung S, et al. [10], Kim J, et al. [11] and Valdes, et al. [17], where CT was performed in all patients in these studies. CT is the reference examination, enabling us to establish classifications that are highly useful for both diagnostic and therapeutic purposes.
We have 06 classifications of zygomatic arch fractures at our disposal, of which the most clinically and paraclinically useful are:
The classification of Özyazgan, et al. [9], which divides fractures of the zygomatic arch into two groups (Figure 5), and the classification of Jung, et al. [10], which proposes a classification of isolated fractures of the zygomatic arch (Figure 6) are the classifications we have used, as they are easy to interpret. However, there is also the classification of Kim Jaye, et al. [11], which offers a very detailed description of isolated zygomatic arch fractures, zygomatic-maxillary complex fractures involving the zygomatic arch and comminuted zygomatic arch fractures (Figure 7 and Figure 8), as well as the classification of Valde R, et al. [17] and Honig, et al. [7]. In our study, combined zygomatic arch fractures accounted for 82% of cases, and isolated zygomatic arch fractures for 18%. Our work is similar to that of Ozyazgan, et al. who found 90.68% combined fractures and 9.32% isolated fractures. But also, those of Kim J, et al. whose combined fractures accounted for 78% of cases and isolated fractures of the zygomatic arch for 22% [9].
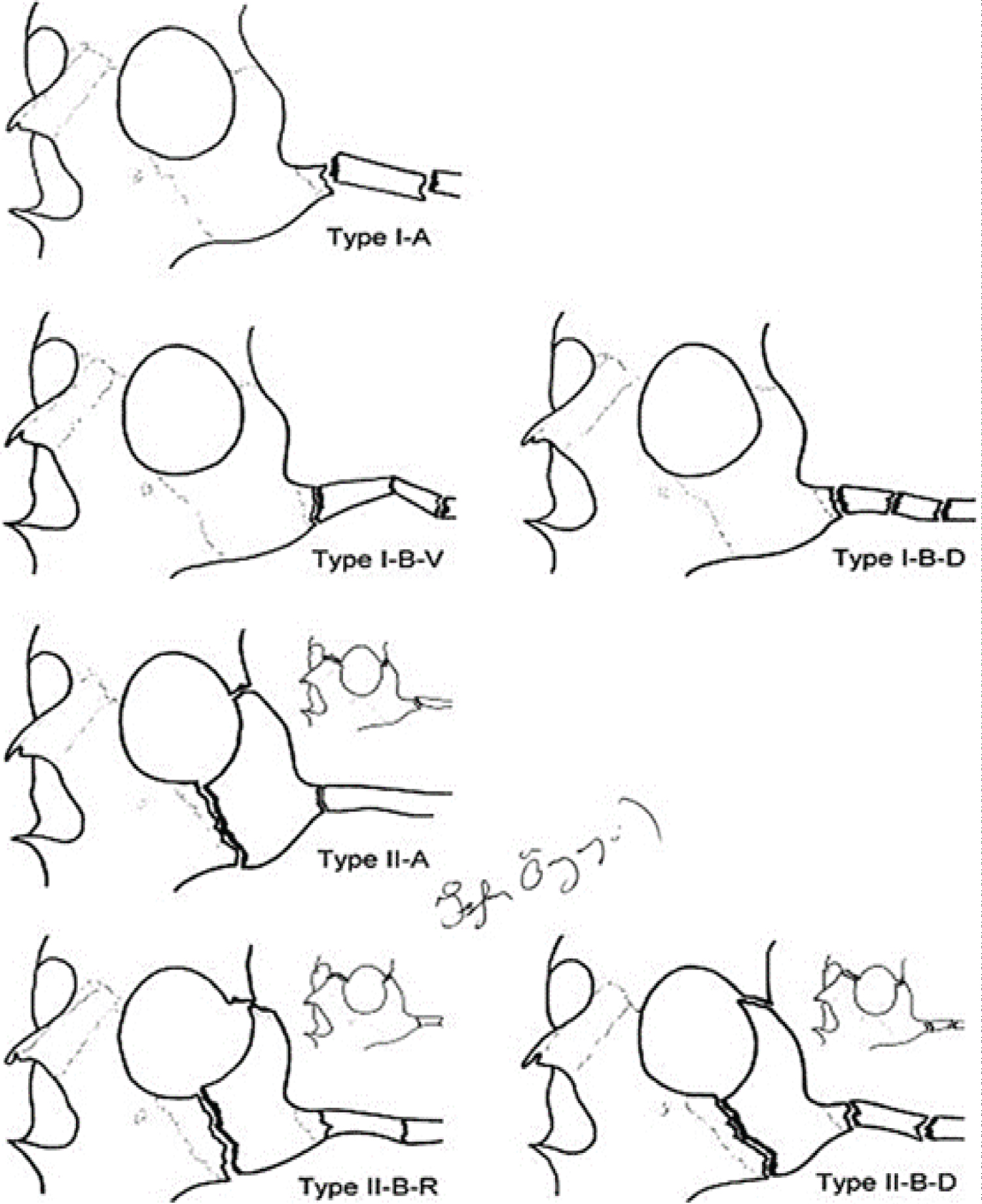 Figure 5: Özyazgan, et al. classification of zygomatic arch fractures [16].
View Figure 5
Figure 5: Özyazgan, et al. classification of zygomatic arch fractures [16].
View Figure 5
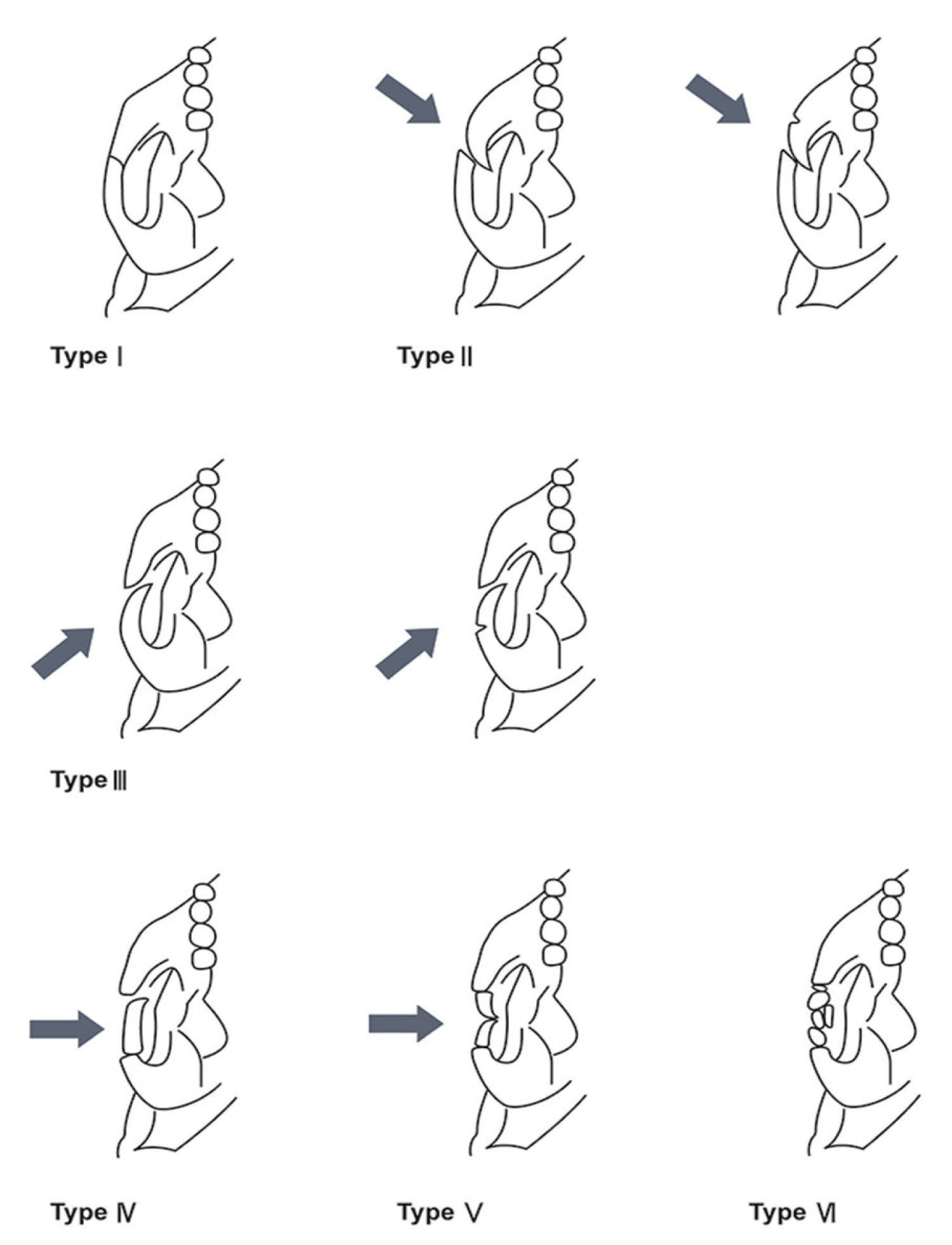 Figure 6: Nam and Jung classification of isolated zygomatic arch fractures (the arrow represents the force vector of the lesion) [12].
View Figure 6
Figure 6: Nam and Jung classification of isolated zygomatic arch fractures (the arrow represents the force vector of the lesion) [12].
View Figure 6
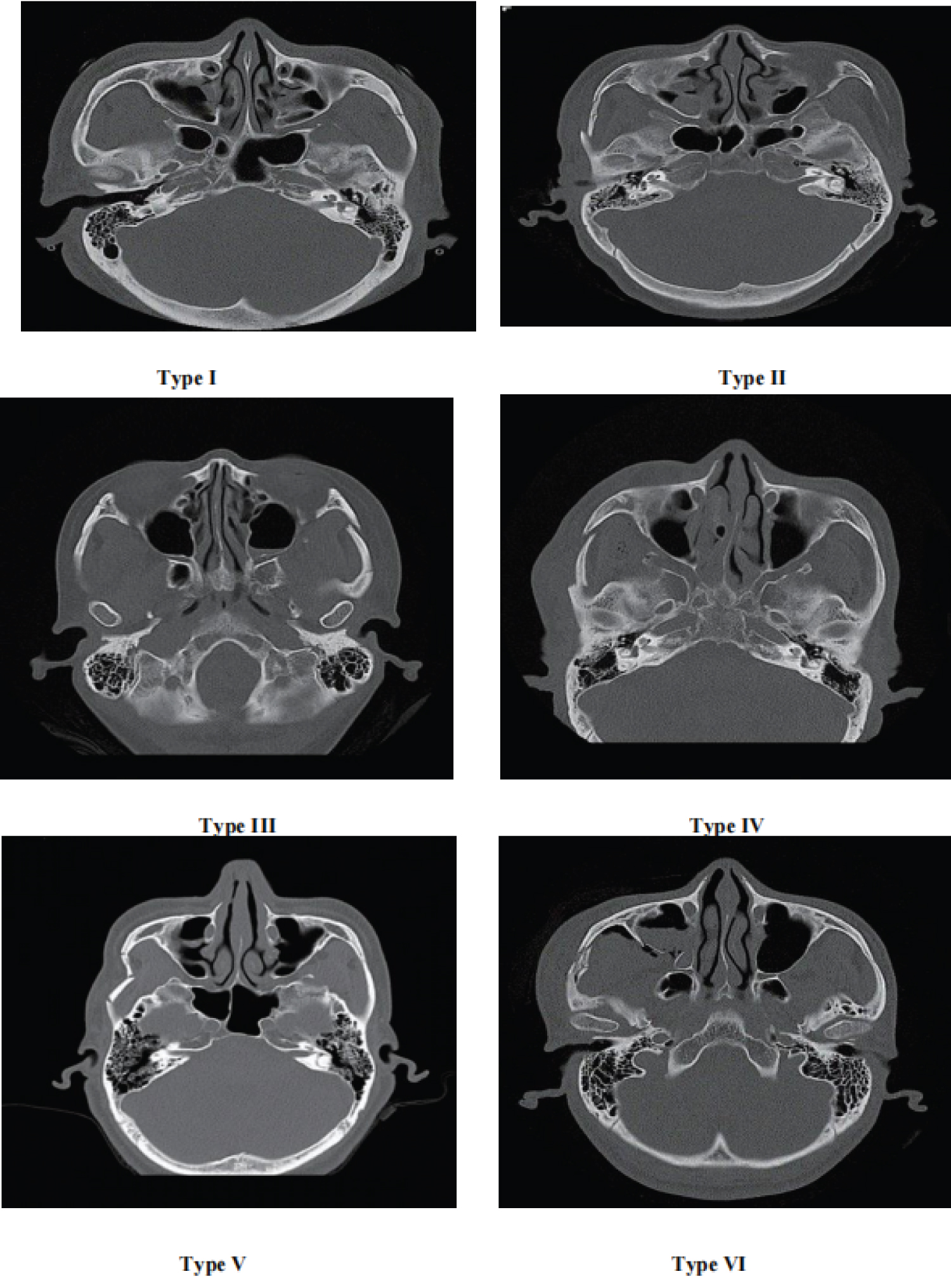 Figure 7: Maxillofacial CT scan in coronal section showing the different types of isolated fractures of the zygomatic arch according to the classification of Jung, et al. 2021 [12].
View Figure 7
Figure 7: Maxillofacial CT scan in coronal section showing the different types of isolated fractures of the zygomatic arch according to the classification of Jung, et al. 2021 [12].
View Figure 7
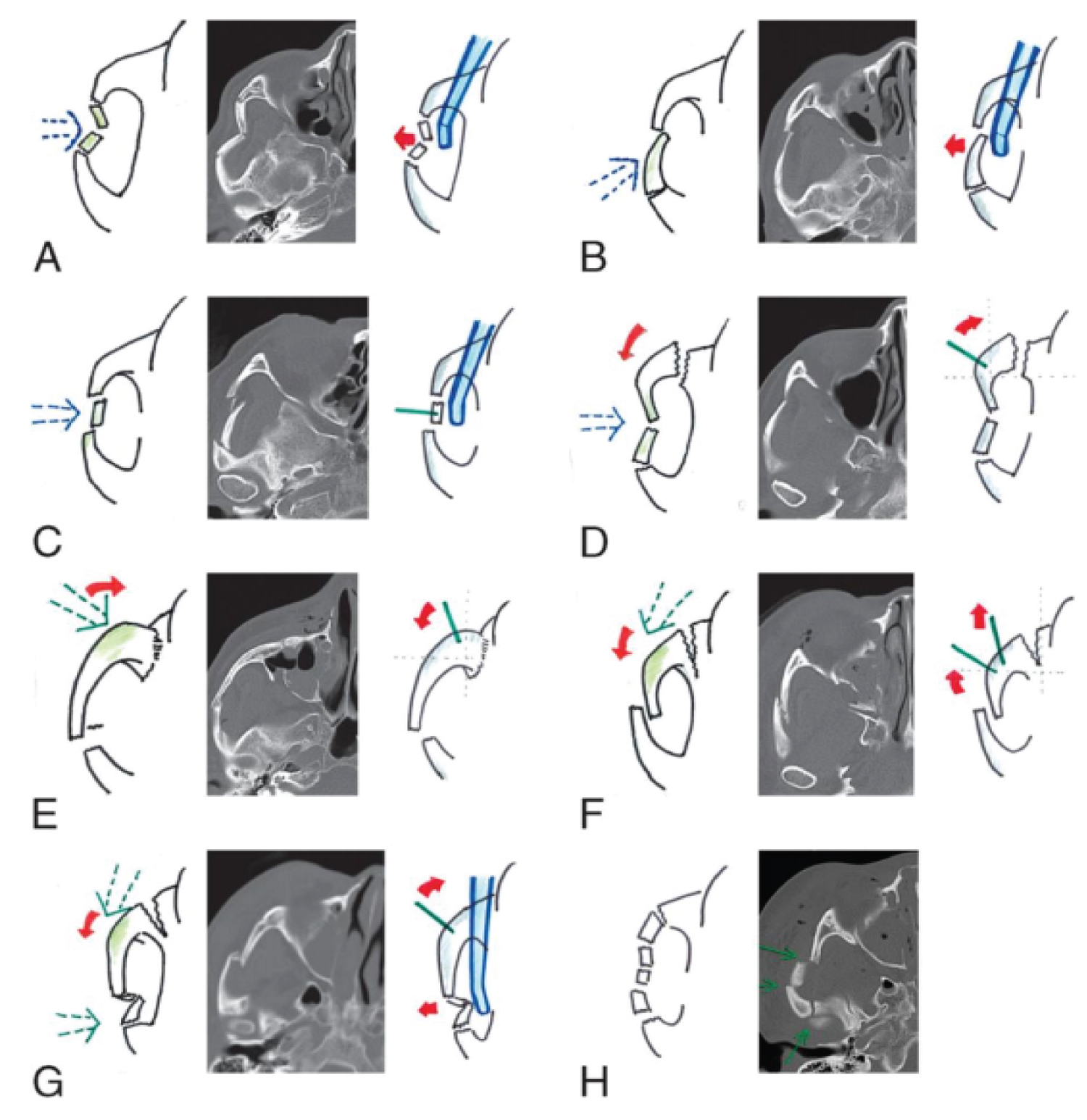 Figure 8: Classification of zygomatic arch fractures and their reduction (arrow Blue dotted line- traumatic force; red arrow- rotation vector; green line- pin inserted on zygomatic segment; blue device- Dingman elevator). A: subtype 1A; B: Subtype 1B; C: Subtype 1C; D: Subtype 2A; E: Subtype 2B; F, Subtype 3A; G: Subtype 3B; H: subtype 4 [11].
View Figure 8
Figure 8: Classification of zygomatic arch fractures and their reduction (arrow Blue dotted line- traumatic force; red arrow- rotation vector; green line- pin inserted on zygomatic segment; blue device- Dingman elevator). A: subtype 1A; B: Subtype 1B; C: Subtype 1C; D: Subtype 2A; E: Subtype 2B; F, Subtype 3A; G: Subtype 3B; H: subtype 4 [11].
View Figure 8
Typing of isolated zygomatic arch fractures revealed that the most predominant subtype was subtype VI with 37.5% of cases, followed by subtype V with 25% of cases. These results differ from those reported in the literature. Thus, for Jung, et al., the majority subtype is subtype V with 56% [10]. In the study by Valdes, et al., the most frequent subtype is subtype IV with 56% [17]. And in the study by Kim J, et al., the most frequent subtype is IIB [11]. The literature testifies to the variability of occurrence of the different subtypes of zygomatic arch fracture in trauma.
With regard to combined fractures of the zygomatic arch, of which Lefort 3 fractures represent 44.44% of cases and malar fractures 33.33%, our results differ from those of the study by Özyazgan, et al. where malar fractures predominate with 71.17% and Lefort III fractures represent 19.51%, whereas in the study by Ragupathy, et al., Lefort III fractures predominate with 51.42% of cases [9,18].
Fractures of the zygomatic arch are common in young males, with road traffic accidents being the main cause. Limited mouth opening, preauricular depression, facial asymmetry and facial pain are the warning signs of a zygomatic arch fracture. CT is the gold standard for confirming the diagnosis, establishing classifications, and identifying associated lesions.