Cardiovascular disease and myocardial infarction comprise the leading causes of more than half of the total death often among elderly people. Psychological stresses, imbalanced diet, sedentary lifestyle, obesity, tobacco, alcohol, and metabolic diseases such as hypothyroidism and diabetes mellitus are the main risk factors for the disease. In order to better understand the underlying risk factor for the disease we performed complete analyses of biochemical factors in sera of obese, non-diabetic and non-hypothyroid male (174) and female patients (213). Among the determinant parameters, TSH, BUN, Creatinine, AST, ALT, FBS, LDL, and TG/HDL ratio, which show correlation and suit structural equation models were selected for path analysis. The averages of these parameters were also compared by one way ANOVA test. In addition, for more detailed comparison, their two-tailed correlations were assessed by Person's test. Our path models indicate that LDL was the central factor mediating causal effects of studied parameters on TG/HDL ratio, the ratio reflecting increased probability for cardiovascular problems. Higher total regression coefficient in female group (twice that of male group) reveals higher susceptibility of female in contrast to male for increased risk of myocardial infarction, the process which we think to be induced primarily by liver abnormality.
TG/HDL ratio, Path analysis, Multivariate regression, Myocardial infarction
TSH: Thyroid Stimulating Hormone; BUN: Blood Urine Nitrogen; FBS: Fast Blood Sugar; TG: Triglyceride; Chol: Cholesterol; HDL: High Density Lipoprotein; LDL: Low Density Lipoprotein; VLDL: Very Low Density Lipoprotein; ALT: Alanine Amino Transferase; AST: Aspartate Amino Transferase
Cardiovascular disease (CVD) is a serious cause of mortality and morbidity in human populations especially in females. Meta data analysis has shown that there is about 50 percent higher risk for cardiovascular disease in females with diabetic, high blood pressure and hyperlipidemia complications compared to males [1]. Diabetic females also show more than 4 fold higher risk for myocardial infarction than males [1,2]. In addition, more abdominal fat storage and lower physical activity in females comprise the main causes for cardiac problems in this group. However different psychological stresses and sex hormones especially in postmenopausal period play roles in this context [3-5]. In hypothyroid females, increased secretion of thyroid stimulating hormone (TSH) with age dependent pattern correlates positively with blood triglyceride (TG) and low density lipoprotein (LDL) [6,7].
It is well known that increased serum TG and/or LDL and decreased high density lipoprotein (HDL) are the two important factors that participate in cardiovascular complications [8]. The ratio of TG/HDL conforms to the risk status of patients to cardiovascular disease, e.g. the higher is the ratio the higher will be the risk of infarction. Accordingly, this ratio is used as a strong independent index to predict the susceptibility to atherogenic abnormalities as well as prediction of insulin resistance prevalence [9,10]. Low ratio of TG/HDL (< 2) is often attributed to high HDL concentration in blood and to normal status. By transporting cholesterol from tissues to liver, HDL acts as safety factor against cardiovascular diseases. On the other hand, high ratio of TG/HDL (> 4), caused by decreased HDL or increased TG concentrations, accelerates cardiovascular events. Therefore, TG/HDL value is accepted clinically as a risk factor. Conversely, acting as endogenous cholesterol transporter from production sites to tissues, LDL comprises a serious risk factor in this context [11-13]. Reports show that TG/HDL ratio statistically correlates with the presence of chronic diseases such chronic renal failure and diabetes mellitus as predisposing factor to cardiovascular complications [10,14-16]. It is important to mention that the association between the chronic disease and TG/HDL ratio higher than 4 is an ethnic and geographic dependent trait [7,17-19]. It is also shown that TG/HDL ratio higher than 3.5 is strongly associated with metabolic syndrome such as hypertension, hyperglycemia, hypercholesterolemia and hypertriglyceridemia with increased fat storage in abdomen that facilitates development of diabetes mellitus as well as cardiovascular diseases [20].
In the current work, we studied the correlation between biochemical parameters including TSH, BUN, Creatinine, AST, ALT, FBS, Chol and LDL in both sexes in order to construct a causality model between these parameters and the corresponding TG/HDL ratios in a bid to find explanation for higher rate of cardiovascular disease and mortality in females compared to males.
A sample, including 174 males and 213 females was selected from outpatients referring to Atieh clinic, No: 122, 9th Bustan, Pasdaran, Tehran, Iran, and their prior consents for enrollment in this study were ensured. The patients aged 40 ± 10 years and had systolic blood pressure of 13 ± 1.5 mmHg, diastolic pressure of 8 ± 2 mmHg, BMI index more than 24, low physical activity, fasting glucose under 120 mg/dL and TG/HDL ratios of more than 4. They were nonalcoholic and nonsmoking except of 30% of male.
In order to carry out biochemistry tests, a 10 ml blood sample per patient fasted for 8-10 hours was taken and left for 15 minutes at room temperature to clot. The samples were then centrifuged for 10 minutes at 1000-2000 × g at 4 degree centigrade. Biochemical factors including BUN, creatinine, AST, ALT, FBS, LDL, HDL and TG were measured by automatic auto-analyzer. Hormone assay of TSH was determined by IDEAL kits (www.mgmkala.com).
Correlations and mean comparisons to construct structural equation modeling (path analysis) were tested by two tail Pearsons' test, one way ANOVA analysis in addition to multiple linear regression using SPSS software (Statistical Package for the Social Science version 21.0.Armonk, NY: IBM Corp. software). P-values of < 0.05 were considered as significance criteria throughout Persons' and ANOVA tests.
Sequential stepwise multiple linear regression tests were performed given TG/HDL as the dependent variable and the rest of factors including TSH, BUN, creatinine, AST, ALT and LDL as independent variables to decide which parameter is the best predictor of variance in TG/HDL ratio. In path model, these factors are the direct effectors linked to TG/HDL ratio. However, in separate regression tests, each of these factors were taken as dependent variables and their linkage to other factors were studied to construct full diagram as path model. As a final step, the obtained diagrams for male and female groups were transferred to AMOS (version 24.0) software to optimize the extracted paths for further consideration [21]. All equations were checked for significance at 0.05 levels.
The guidelines of Ethical Committee of Shahid Chamran University of Ahwaz, Iran, were observed throughout this study.
One-way ANOVA analysis we carried out in order to compare biochemical parameters determined in this study for both sexes. Table 1 represents the results as Mean ± SD with corresponding p-value for each parameter. As shown, BUN and creatinine, as markers for kidney function, fall in normal range for both groups. Hepatic enzymes of AST and ALT are also in normal range. Despite the fact that kidney and hepatic markers are significantly higher in males than females, males seem to be at higher risk to kidney, hepatic and consequently cardiac problems as they get elder. The only out of range parameter in these groups is LDL. Given the role of LDL in cardiovascular disease, greater levels of LDL in female group may reasonably lead to higher incidences of cardiac diseases. However, TSH and FBS levels were in normal range and did not differ significantly.
Table 1: One-way ANOVA test carried out for parameters measured in male and female groups. View Tables 1
Table 2a and Table 2b show Persons' results for all parameters listed in Table 1 for males and females respectively. The tests were performed to assess the significant correlations between paired parameters to be used for further analysis. Those parameters which showed at least one significant correlation (Table 2a and Table2b) were used for multivariate regression and path analysis.
Table 2A: Results of two-tailed Pearsons' test for parameters in male group (n = 174) having the ratio of TG/HDL > 4, P-values are shown in parenthesis. View Table 2A
Table 2B: Results of two-tailed Pearsons' test for parameters in female group (n = 213) having the ratio of TG/HDL > 4, P-values are shown in parenthesis. View Table 2B
As tabulated, all measured parameters for both groups display at least one significant correlation. Accordingly, all parameters were entered in multivariate regression and path modeling tests. As described earlier (in Methods), in linear regression tests, TG/HDL ratio was used as a dependent variable and the remaining parameters were used as independent variables. The tests were done using SPSS software in a stepwise mode of linear regression. As indicated in Figure 1, LDL is the only variable that affects TG/HDL ratio directly, therefore, all other variables are excluded from the models. This means that the remaining variables affect TG/HDL ratio indirectly via LDL. In the next step, we repeated the regression test using LDL as a dependent variable and the rest as independent variables. Figure 1A and Figure 1B represent the final diagrams obtained for male and female groups respectively. These diagrams are plotted, optimized and standardized in AMOS (version 24). One headed arrows are drown from independent to dependent variables carrying standardized regression coefficients as superscripts. Two headed arrows are linking two independent variables. These arrows are added to the model on a try and error basis. In case the added arrows improved the model they were kept, otherwise they were removed. The connection reveals that there should be a statistic relation between the interacting variables that caused by an unknown intervening variable. The circles with (e) sign linked to each dependent variable comprise the error parts of the model which define that parts of variance in dependent variables not predicted directly or indirectly by linked independent variables.
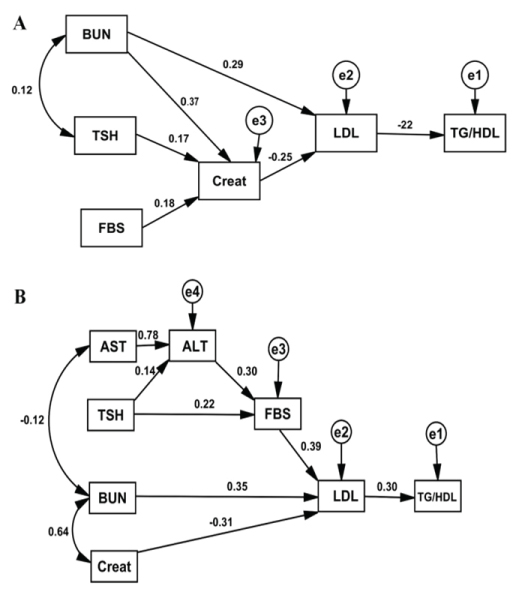 Figure 1: The best diagram extracted for male (A) group (n = 174) and female (B) group (n = 213).
Figure 1: The best diagram extracted for male (A) group (n = 174) and female (B) group (n = 213).
All variables (dependent and independent) are shown in rectangles. Variables not included in the models are shown in circles. Single headed arrows with standardized coefficients link independent variables to dependent variable. The diagrams are plotted and optimized in Amos (version 24.0).
View Figure 1
Table 3 and Table 4 summarize the regression standardized coefficients for direct and indirect effects of all parameters included in models for male and female groups. Positive coefficients mean that increase in an independent variable leads to rise in a dependent variable and vice versa. We also calculated overall coefficients for male and female groups as 0.250 and 0.503 respectively.
Table 3: Regression coefficients for direct and indirect effects for parameters included in path diagram for male shown in Figure 1A. View Table 3
Table 4: Regression coefficients for direct and indirect effects for parameters included in path diagram for female shown in Figure 1B. View Table 4
Table 5 represents model fitting parameters extracted for male and female models from AMOS software. P-vale higher than 0.05, TLI (Tucker Lewis index) and CFI (Comparative Fit Index) greater than 0.95 and RMSEA (Root Mean Square Error of Approximation) lower than 0.05 as well as Chi-Square/DF ratio lower than 5 are indicators accepted for models with good fit indices [22,23]. As shown, our models are in good fit state for both groups and the models could be used for data processing and discussion.
Table 5: Parameters for model fit in our study extracted from Amos (version 24.0) software for male and female models. View Table 5
Despite our record (Table 1) and many other reports on higher levels (p-value < 0.01) of BUN, creatinine, AST and ALT in males compared to females measured in non-diabetic and non hypothyroid individuals [14,15,20], cardiovascular disease and myocardial infarction have greater rate of incidence in female group [1,2]. Path analysis provides a powerful means to build a causal linkage between the biochemical parameters and TG/HDL ratio and helps to quantify these relations.
Figure 1A and Figure 1B represent path diagrams for male and female respectively. The first point drown from these figures is that LDL acts as the central factor affecting TG/HDL ratio and is, therefore, the main parameter effective in myocardial infarction experience. The second point is that the number of parameters participating in females' diagram are much more than those involving in males' one, while the total regression coefficients for these parameters are 0.503 and 0.250 for both sexes respectively. The greater positive coefficient for females means that the risk of cardiovascular disease in female is two folds higher than in males. The third point is that FBS showed coefficient 3 times higher for male than for female group, in contrast to TSH which showed coefficient 3 times higher for female group. These findings convey that unbalanced diet which increases fasting glucose in aged males may exert effect on TG/HDL ratio in females at 3 times higher levels with higher cardiovascular consequences. By the same token, hypothyroidism disease, which is more frequent in elderly females, causes 3 times more cardiovascular incidences, as widely reported [2-5].
The fourth point is that BUN and creatinine exert positive and negative effects on LDL variable respectively, but they exert the same net positive effect on TG/HDL ratio in both sexes. According to our models and given the positive effects of creatinine and BUN on TG/HDL value, abnormal increase in these two factors in patients with renal insufficiency may comprise risk factors of myocardial infarction frequency in both sexes, the fact that contrasts previous reports [10,14-16]. The fifth point is that hepatic enzyme of AST and ALT showed a cumulative coefficient of 0.062 on TG/HDL ratio equal to 12% of total effects of all parameters in female group but never in male group. This fact reveals that hepatic problems is the main factor playing role in myocardial infarction in females.
Given the fact that all parameters studied here are metabolized partly or totally in liver and the number of parameters involved in females' diagram are greater than males' one, we can conclude that females' liver is in more worsen status than that of males, the condition that exposes females to higher risk of myocardial infarction.
The authors would like to express their thanks to the vice chancellor of research and technology of Shahid Chamran University of Ahvaz for providing the financial support of this study under Research Grant No: 963027207.