The Fetiform Teratoma (FT) is a rare entity, characterized by presenting tissues of different pluripotent cells without organization or organogenesis. Fetus in Fetus (FIF) on the other hand is usually an encapsulated lesion, with rudimentaryly developed organs and typically the presence of vertebral bodies.
A 5-month-old with normal prenatal checks, with a right permeable hydrocele antecedent, a non-painful and well-delimited mass, which occupied the entire right hemi abdomen, was incidentally detected. Ultrasound and abdominal CT show a retroperitoneal lesion that occupied the entire abdominal cavity, with the presence of fat bulbs and calcifications, which did not depend on any organic structure. Tumor markers were normal. Laparotomy was performed with complete exéresis of tumour. Histopathological study showed a mixed composition, being compatible with immature fetiform teratoma. Favorable evolution.
Fetus in fetu, Teratoma, Retroperitoneal, Mass
Teratomas are neoplasms made up of tissues that do not belong to the anatomical site where they are found. They show varying degrees of differentiation, from simple somatic elements to highly structured formations with axial and metameric organization. Its most frequent location is in the sacrocoxygeal region, although they can also be located in ovaries, retroperitoneum, head, neck and mediastinum, among others.
The Fetus In Fetu (FIF) is a rare congenital malformation, distinguished from Fetiform Teratomas (FT) by the presence of a vertebral axis in an encapsulated, pedunculated mass, of the fetiform type, with disorganized structures around this axis. It is more frequently located in the retroperitoneal area. However, there is controversy in the distinction between fetus in fetu and fetiform teratoma and that both entities could represent two aspects of the same pathology at different stages of maturation [1-6].
A 5-month-old with normal prenatal checks, with a right permeable hydrocele antecedent, that during an episode of bronchiolitis a non-painful and well-delimited mass, which occupied the entire right hemi abdomen, was incidentally detected. Ultrasound and abdominal CT show a 16 × 9 × 8 cm retroperitoneal lesion that occupied the entire abdominal cavity, with the presence of fat bulbs and calcifications, which did not depend on any organic structure (Figure 1A and Figure 1B). Tumor markers were normal.
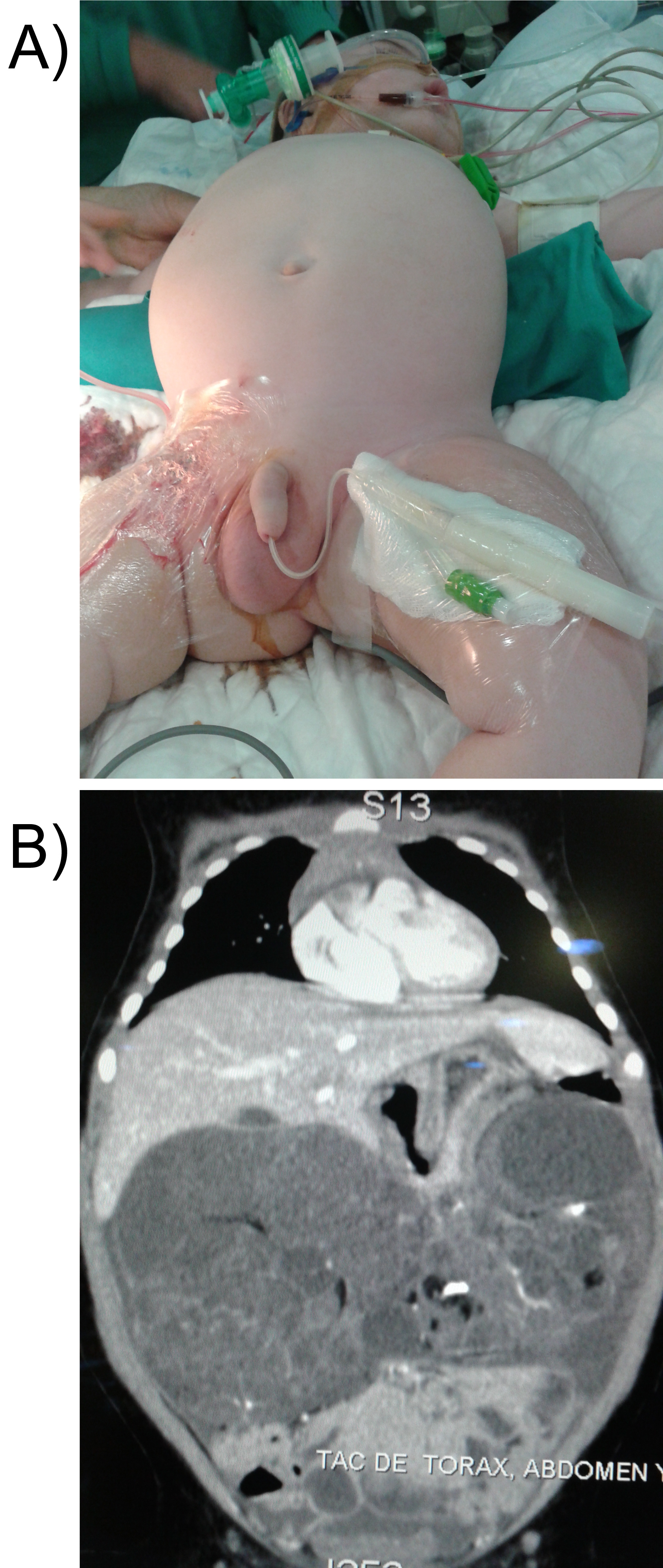 Figure 1: A,B) Abdominal mass and TC: A 16 × 9 × 8 cm retroperitoneal mass that occupied the entire abdominal cavity, with the presence of fat bulbs and calcifications.
View Figure 1
Figure 1: A,B) Abdominal mass and TC: A 16 × 9 × 8 cm retroperitoneal mass that occupied the entire abdominal cavity, with the presence of fat bulbs and calcifications.
View Figure 1
Laparotomy was performed with complete exéresis of a rich-looking tumour that has adhesions to the gastric minor curvature (Figure 2A and Figure 2B).
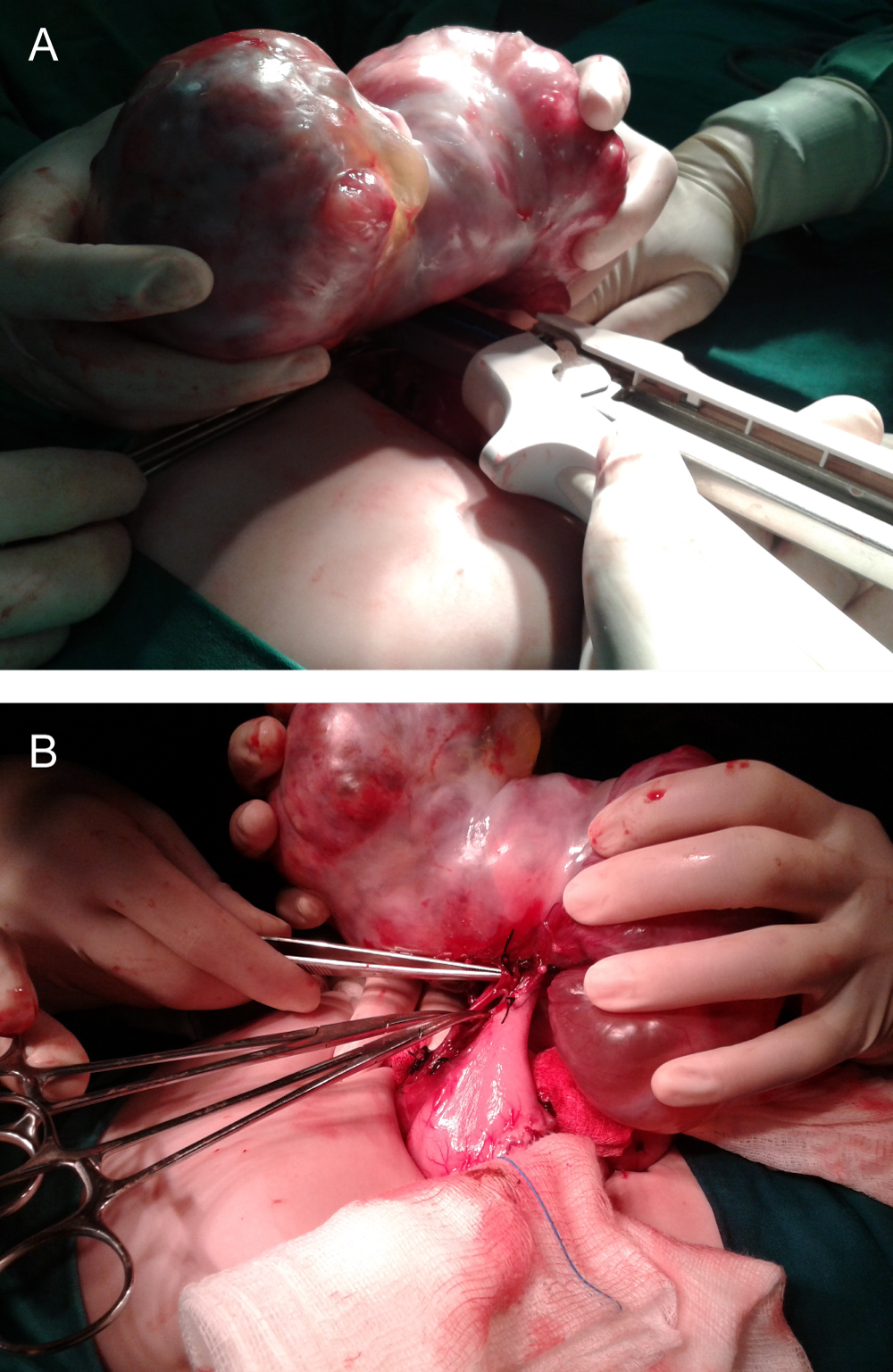 Figure 2: A,B) Intraoperative image showed fetiform teratoma attached to the gastric minor curvature.
View Figure 2
Figure 2: A,B) Intraoperative image showed fetiform teratoma attached to the gastric minor curvature.
View Figure 2
Histopathological study showed a mixed composition: An area of structures very different from the endo-ectoderm type (digestive system, respiratory, skin, pancreas) along with immature mesodermal-type forms (fibro-mixoid and osteo-cartilaginous tissue); and 65% of the lesion made by neural tissue, being compatible with immature fetiform teratoma (Figure 3A and Figure 3B). Favorable evolution.
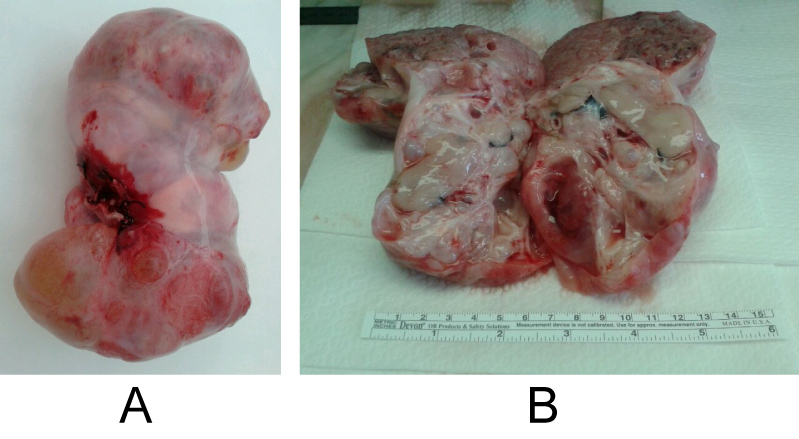 Figure 3: A,B) Macroscopic aspect and section of immature fetiform teratoma.
View Figure 3
Figure 3: A,B) Macroscopic aspect and section of immature fetiform teratoma.
View Figure 3
Fetus in Fetu (FIF) is a rare congenital malformation. Its estimated incidence is 1: 500,000 live newborns; About 200 cases have been published. Its etiopathogenesis is an abnormal embryogenesis in a biamniotic monochromic gestation in which one fetus is inside the other [6-9].
Its diagnosis is based on imaging tests. Prenatal ultrasound can identify a cystic mass with solid components and/or calcifications. Postnatally, simple radiography shows bone structures, although their non-visualization does not exclude the diagnosis, the presence of vertebral bodies is pathognomonic. The CT scan details the structures that constitute the mass, its vascular anatomy and the relationship with the adjacent organs, important for the surgical approach. MRI is gaining prominence due to its high spatial resolution and discrimination between tissues, also prevents radiation and the use of intravenous contrast. Occasional serum elevation of alpha-fetoprotein and/or beta-hCG has been reported in relation to this disease.
The main differential diagnosis is with the highly differentiated teratoma. The existence of vertebral bodies in the FIF indicates that the parasitic fetus reached the early embryogenic stage of the notocorda, precursor of the spine. In contrast, Fetiform Teratoma (FT) is caused by uncontrolled growth of pluripotential cells without organogenesis or vertebral segmentation. Also, unlike fetiform teratoma, FIF does not usually present recurrences and rarely malignant. Despite the benignity, the evolution of the mass can compromise adjacent structures, so surgical resection is the first therapeutic option. Likewise, monitoring of serum beta-HCG and alpha-fetoprotein and ultrasound monitoring of these patients for 2 years is recommended.
Several works in the literature indicate the probability of a progression between a fetiform teratoma and a fetus in fetu [7-9]. The need for the existence of a vertebral axis to affirm the existence of FIF has been frequently questioned. Spencer [10], suggested that the existence of a central nervous system or a spinal cord for the definition of fetus in fetu is superfluous, and that once the skull-caudal metameric pattern is established, many structures can survive beyond the disappearance of a rudimentary vertebral axis. The FIF has previously been considered a homozygous twin included, but lately the most agreed opinion in the literature is that it is a highly organized form of the teratoma. The assumption of this concept has practical value in terms of prognostic implications, because it implies the existence of a small but present risk of malignancy that requires the complete removal of the mass to prevent recurrence, and the careful search for immature components in the mass excised.
Unlike Fetus in Fetu, the Fetiform Teratoma is a more immature tumor so it requires stricter follow-up due to the presence of malignancy. Thus requiring a complete surgical resection.
The authors declare that they have no conflicts of interest and have nothing to disclose.
The co-authors declare that they have contributed to the preparation of the work and authorize the principal author to have their personal data appear in the publication. All authors declare that they participated and contributed to the preparation and writing of this work.