Different surgical techniques have been described to treat anteroposterior collapse in the palate. Anterior palatoplasty produces greater rigidity and anterior displacement of the soft palate, widening the retrouvular space.
Objectives: Determining the success rate of anterior palatoplasty surgical technique for treating patients with
Design: Descriptive and prospective.
Methods: Patients treated for snoring and obstructive sleep apnea with the anterior palatoplasty surgical technique between March 2017 and March 2023 were included in the study.
Patients with a body mass index greater than 30 and those who did not have a postoperative evaluation at 6 months using polysomnography or a questionnaire to assess snoring improvement were not included. The following data were prospectively collected: Age, sex, results of rhinofibrolaryngoscopy (RNF) with Müller maneuver in sitting position (March 2017 to October 2018) or sleep endoscopy (SE), along with the results of the nocturnal polysomnography.
Surgical outcomes were assessed at 6 months, considering the surgery successful if the improvement in snoring was ≥ 50% and the apnea/hypopnea index decreased by 50% or more or to less than 10.
Results: Twenty-one patients with anterior palatoplasty for snoring or OSA were treated. Eight patients were excluded from the results analysis because they did not undergo postoperative PSG or did not respond to the questionnaire about snoring improvement. Of the 13 patients who completed postoperative studies, six were evaluated using the Muller maneuver, and seven with SE.
In the group evaluated with the Muller maneuver the improvement achieved after anterior palatoplasty was 66.67%.
Among patients evaluated using SE the improvement observed was 83.30%. The overall improvement achieved in all patients was 74.98%.
Conclusions: The success rate of anterior palatoplasty for the treatment of snoring and obstructive sleep apnea in our series was 74.98%. The outcome was better in patients selected with sleep endoscopy.
Obstructive sleep apnea, Snoring, Anterior palatoplasty, Sleep endoscopy
Surgical techniques indicated to address snoring and obstructive sleep apnea (OSA) have evolved from respective surgeries of soft palate sectors that included the underlying muscle to less aggressive techniques that preserved palate muscles and shifted surgical focus from ablation to reconstruction and repositioning, thereby stiffening tissues and modifying palate position. Many surgeries targeting the palate have been described since Ikematsu's uvulopalatopharyngoplasty and later by Fujita and Simmons [1]. Minimally invasive techniques such as interstitial radiofrequency [2], palate implants [3], CAPSO (palate stiffening by cauterization) [4], and barbed suture placement [5] are most commonly used to address anteroposterior collapse of the soft palate. The anterior palatoplasty described by Kenny Pang [6] combines the CAPSO technique with suturing of resected mucosa margins, producing stiffness and anterior displacement of the soft palate.
Determining the success rate of anterior palatoplasty surgical technique for treating patients with snoring and obstructive sleep apnea selected through Müller maneuver or sleep endoscopy.
Descriptive and prospective.
Patients treated for snoring and obstructive sleep apnea with the anterior palatoplasty surgical technique between March 2017 and March 2023 were included in the study. Patients with a body mass index greater than 30 and those who did not have a postoperative evaluation at 6 months using polysomnography or a questionnaire to assess snoring improvement were not included. Patients with moderate or severe obstructive sleep apnea were not willing to use CPAP. The following data were prospectively collected: Age, sex, results of rhinofibrolaryngoscopy (RNF) with Müller maneuver in sitting position (March 2017 to October 2018) or sleep endoscopy (SE) performed with Propofol and monitored by bispectral index (BIS). The diagnosis determined whether the collapse occurred in the palate or pharynx (in anteroposterior, lateral, or concentric direction), or in the base of the tongue or epiglottis, establishing the degree of collapse expressed as a percentage from 0 to 100%, along with the results of the nocturnal polysomnography.
It was recorded whether anterior palatoplasty was associated with another surgical procedure and if there were any complications. Postoperative outcomes were evaluated using PSG in patients who had an apnea/hypopnea index > 10 and with a questionnaire assessing the percentage improvement in snoring (0 to 100%).
The anterior palatoplasty technique involved performing, under general anesthesia with cautery, a rectangular resection of the mucosa and submucosa of the soft palate measuring 40 mm in length × 7 mm in height while preserving the muscular plane. The resection boundaries were 4 mm above the junction of the hard and soft palate (posterior nasal spine), 4 mm below the uvula base, and laterally from a line extending from the anterior tonsillar pillar to the soft palate.
Subsequently, two lateral incisions were made near the uvula, followed by a partial uvuloplasty. The mucosal margins of the rectangular mucosal resection of the palate were sutured with 4/0 Vicryl, resulting in anterior displacement of the palate (Figure 1).
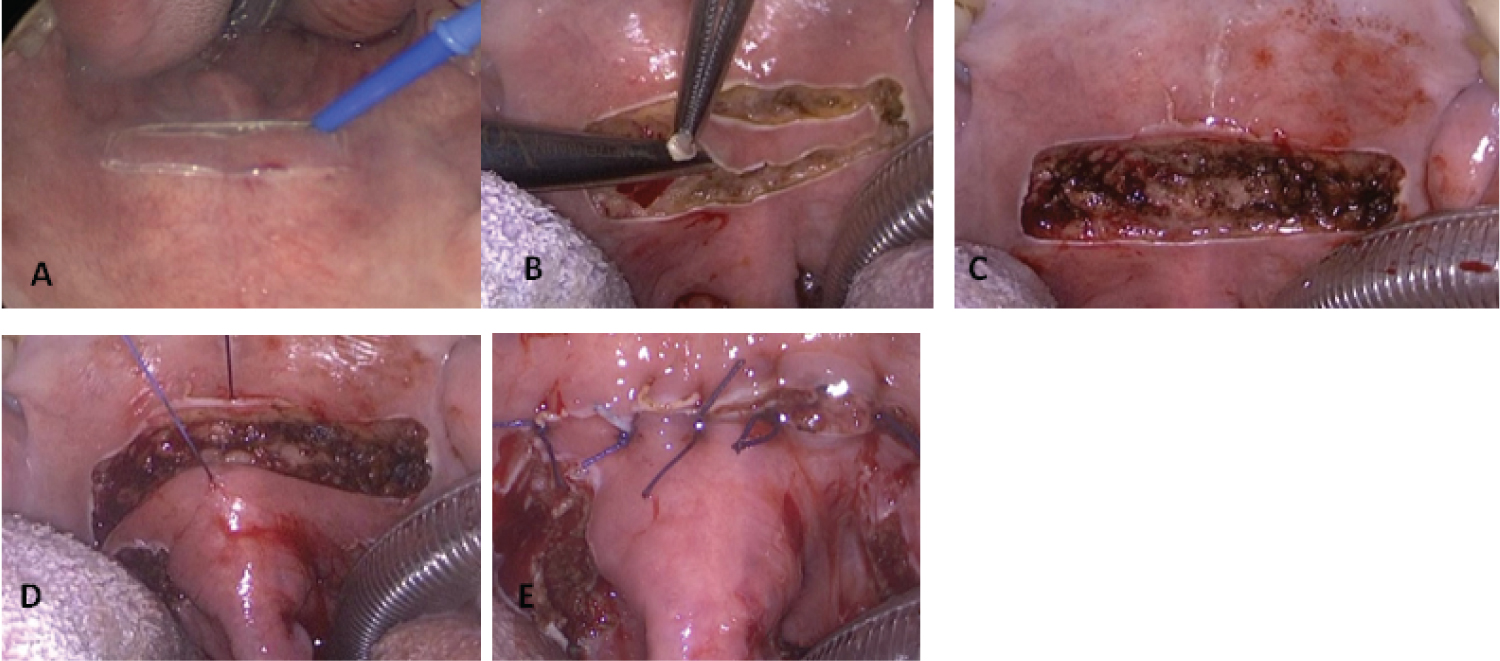 Figure 1: Anterior palatoplasty technique: A) Rectangular mucosal resection on the palate; B) Submucosal resection; C) View of the palate after mucosal and Submucosal resection; D) Elevation and anterior displacement of the palate when pulling mucosal sutures; E) Mucosal suture of the palate.
View Figure 1
Figure 1: Anterior palatoplasty technique: A) Rectangular mucosal resection on the palate; B) Submucosal resection; C) View of the palate after mucosal and Submucosal resection; D) Elevation and anterior displacement of the palate when pulling mucosal sutures; E) Mucosal suture of the palate.
View Figure 1
In some patients, a Vicryl suture was placed between the deep muscular plane and the aponeurosis at the junction of the hard and soft palate (posterior nasal spine) (Figure 2).
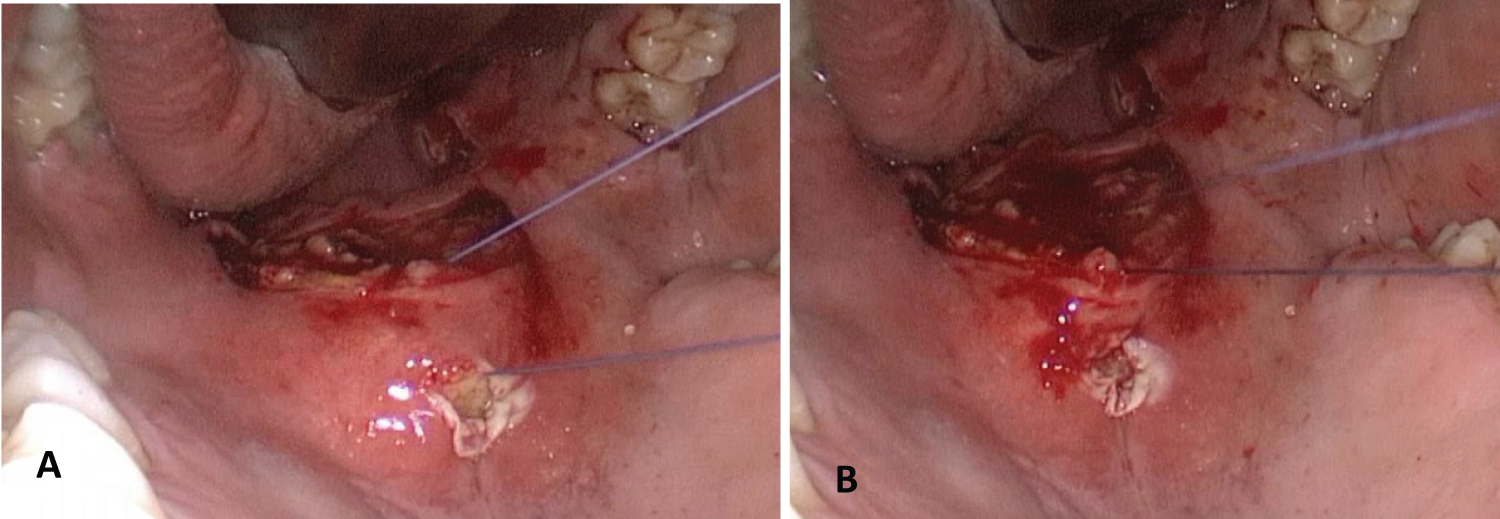 Figure 2: Resorbable suture between the deep muscular plane and the aponeurosis at the junction of the hard and soft palate (posterior nasal spine). A) Suture of the muscular plane passing through the aponeurosis that is externalized at the level of the union of the hard and soft palate; B) Suture enters from the outside towards the muscular plane encompassing aponeurosis at the level of the posterior nasal spine and is adjusted.
View Figure 2
Figure 2: Resorbable suture between the deep muscular plane and the aponeurosis at the junction of the hard and soft palate (posterior nasal spine). A) Suture of the muscular plane passing through the aponeurosis that is externalized at the level of the union of the hard and soft palate; B) Suture enters from the outside towards the muscular plane encompassing aponeurosis at the level of the posterior nasal spine and is adjusted.
View Figure 2
For patients with ASA I-II, with snoring or mild OSA, surgeries were performed on an outpatient basis. For ASA III or moderate/severe OSA patients, the surgeries were performed with the patients staying hospitalized for 24 hours in the intermediate care unit.
Surgical outcomes were assessed at 6 months, considering the surgery successful if the improvement in snoring was ≥ 50% and the apnea/hypopnea index decreased by 50% or more or to less than 10.
Twenty-one patients with anterior palatoplasty for snoring or OSA were treated between March 2017 and March 2023. Twenty were male, and one was female, with a minimum age of 28 and a maximum of 70 years, with an average age of 47.9 years. All patients had a single or predominant anteroposterior collapse at the palate level diagnosed with RNF with Muller maneuver (13/21) and SE (8/21).
One patient had primary snoring, and the remaining 20 had OSA: Mild (9/20), moderate (8/20), and severe (3/20).
Anterior palatoplasty was associated with nasal surgery in 11 patients (septoplasty, inferior turbinoplasty, adenoidectomy, endoscopic sinus surgery), and in 5 patients, tonsillectomy was also performed.
There were no complications.
Eight patients were excluded from the results analysis because they did not undergo postoperative PSG or did not respond to the questionnaire about snoring improvement. Of the 13 patients who completed postoperative studies, six were evaluated using the Muller maneuver, and seven with SE.
In the group evaluated with the Muller maneuver, one patient with primary snoring did not improve snoring intensity. Two patients with mild apnea indices of 7 and 5 showed snoring improvement of 70% and 90%, respectively. Two patients with moderate apnea/hypopnea indices improved from 15.8 to 6.6 and from 25.3 to 12, respectively. Another patient with moderate apnea worsened the postoperative AHI index (16 to 31.5).
In this series of patients, the improvement achieved after anterior palatoplasty was 66.67%.
Among patients evaluated using SE, two with primary snoring improved snoring by 80% and 100%, respectively. One patient with mild apnea (AHI: 13.3) showed a 50% improvement in snoring but did not undergo postoperative PSG. Another patient with mild OSA significantly improved from 15 to 4, and one patient did not change their apnea-hypopnea index (20.3 to 19.2). Another patient with moderate OSA (AHI: 15.8) did not undergo postoperative PSG, but snoring improved by 100%. A patient with severe OSA (AHI: 63.4) experienced a reduction in their apnea-hypopnea index by more than 50% (postoperative AHI: 26.5). The improvement observed in this SE-selected group was 83.30%. The overall improvement achieved in all patients was 74.98% (Table 1).
Table 1: Results of patients treated with anterior palatoplasty for snoring and obstructive sleep apnea. View Table 1
The surgical technique of anterior palatoplasty was described by Kenny Pang in 2013 [6], modifying previous techniques such as CAPSO, which had good results in improving snoring (77% reduction in snoring at one year in 206 patients) [4]. However, CAPSO caused unpredictable scarring of the soft palate with adhesions that pulled the lateral pharyngeal walls, leading to narrowing of the lateral distance between the tonsil and the pillars. Suturing the margins of the resected mucosal rectangle closes the wound and promotes predictable healing by advancing and stiffening the soft palate. The original technique was described using local anesthesia; however, in our series, patients underwent surgery under general anesthesia primarily because the majority also required nasal surgery or tonsillectomy. Anterior palatoplasty can also be combined with the barbed suture technique in the palate, providing sutures from the muscle to the hamulus and to the aponeurosis at the junction of the hard and soft palate or by suturing back and forth from side to side through the respected mucosal rectangle [7]. In some patients in our study, we sutured the deep plane of the palate to the posterior nasal spine of the palate. Others have reported combining anterior palatoplasty with sphincter pharyngoplasty [8].
We believe that it is better to combine pharyngoplasty, especially if it is with barbed suture, with the suture from hamulus to hamulus passing through the posterior nasal spine to treat when there is anteroposterior collapse.
Several studies have reported a better diagnosis of the collapse site in the airway causing snoring and apnea with sleep endoscopy, but they highlight that there is no consensus on whether this examination can predict the success of surgery. In a systematic literature review, 535 patients were included, comparing the topodiagnosis of the collapse site diagnosed by evaluating the awake patient vs with sleep endoscopy. Treatment changed after sleep endoscopy in 50.24% of cases, and these changes were most frequently associated with hypopharyngeal and laryngeal structures. The authors conclude that there is insufficient evidence to link these changes with better surgical outcomes. In another multicenter study that included 275 patients, the results of sleep endoscopy and its correlation with surgical outcome were evaluated. They concluded that the prognosis of surgery was not clearly related to the type and degree of velopharyngeal obstruction [9].
In a multicenter, prospective study including 326 patients, the evaluation of the collapse site with sleep endoscopy vs without SE was compared. They concluded that preoperative SE did not affect the surgical outcome [10,11].
In our study, the comparison between two small patient groups showed a trend toward better surgical outcomes in those who underwent topodiagnosis of anteroposterior palate collapse using SE compared to RNF with Muller.
In a systematic review including 240 patients treated with anterior palatoplasty with and without multilevel surgery, a significant improvement was reported in the apnea-hypopnea index, visual analog scale of snoring, and Epworth Sleepiness Scale. The success rate of palatoplasty was 72.5% with a follow-up of 17.3 months [12].
Binar, et al. [13] in a meta-analysis involving 170 patients treated for obstructive sleep apnea syndrome (OSAS) reported a success rate of anterior palatoplasty (reduction of AHI ≤ 50% and < 20) of 60.6%.
In our study, the results of anterior palatoplasty are compared with those reported in the literature.
The success rate of anterior palatoplasty for the treatment of snoring and obstructive sleep apnea in our series was 74.98%. The outcome was better in patients selected with sleep endoscopy.
Anterior palatoplasty is a simple surgical technique that can be combined with other surgeries to treat multilevel collapse, preferably in patients with primary snoring and mild to moderate obstructive apneas with topodiagnosis of anteroposterior collapse at the level of the palate.
This work did was not supported by any funding.
All of the above authors have seen and approved the manuscript.
The authors do not have any conflict of interest to declare.