Background: College students engage in large amounts of sedentary behavior which have been linked to adverse mental health outcomes. Poor postural habits due to the increase in this behavior, in conjunction with prolonged mobile phone usage, can lead to poor posture in these younger populations. As such, this study aims to identify how college-students feel about their posture, the prevalence of pain patterns, psychological status, and their knowledge of intervention options available.
Methods: A descriptive, observation survey study collected data from a healthy college-age population of 58 male and 100 female (n = 158) (mean = 21.6 ± 1.9y). Survey included assessments of self-perceived attitudes regarding posture, ergonomics, neck disability (NDI), mental health outcomes, knowledge of postural rehabilitation techniques, and range of motion (ROM).
Results: In total, 88.6% of participants wished their posture was better, 93.7% and 96.2% believed their standing and sitting postures could be improved, respectively. Thirty-five percent of participants qualified as Mild or Moderate Disability based upon their cumulative NDI scores. Strong correlations (r = 0.61) between participants' self-reported need to improve standing and sitting posture, and a moderate correlation(r=-0.47) between pain when sitting and total NDI.
Conclusion: We noted a prevalence of posture-related issues and the impacts on daily function including sleeping and sitting. Future research should look to objectively assess posture through validated measures to investigate the extent of posture-related pain and dysfunction. To alleviate early-onset neck pain and reduce the risk of developing future chronic neck pain, college aged populations need education on proper posture and rehabilitation interventions designed to alleviate pain and dysfunction over the short- and long-term.
Posture, College students, Pain, Psychology
MET: Metabolic Equivalent for Task; FHP: Forward Head Posture; CVA: Craniovertebral Angle; GDPR: General Data Protection Regulations; NDI: Neck Disability Index; DPES: Dispositional Positive Emotion Scale; ROM: Range of Motion; BMI: Body Mass Index
It has been shown that college students engage in large amounts of sedentary behavior irrespective of geographical location, in the form of class, study, and leisure activities [1-3]. Sedentary behavior has been defined as a metabolic equivalent (MET) of ≤ 1.5 while in a relaxed position such as sitting [4]. Long durations of sedentary behavior have been associated with negative psychological states such as depression and anxiety [5] and can cause changes in musculoskeletal function. As hybrid and remote learning environments have increased, college students may be at more risk of sustaining adverse body positions which can ultimately lead to negative psychological states and chronic changes in individual posture and musculoskeletal function.
College is a pivotal time for this age population as they position themselves for a career that is accompanied by a median annual salary $20,000 higher than those who don’t complete a college undergraduate program [6]. Therefore, maximizing the ability to maintain optimal mental, emotional, social, and physical health during this period is of critical importance.
Unfortunately, according to the American College of Health Association [7], 27.4% and 21.7% of college students had been diagnosed with anxiety or depression, respectively. These findings are substantiated by independent studies that report from 20% to 36% of college-aged students are impacted by mental health issues [8-10] and over half of students were categorized as having poor sleep [11] or sleeping less than 8 hours per night [12,13]. The need for specific mental health intervention strategies in this population are imperative, and research has commonly cited physical activity as an effective intervention strategy [14-18].
Nonverbal communication literature has demonstrated a person's posture has been linked to pain measures, quality of life, and mental health outcomes such as mood and confidence [19-21]. Forward head posture (FHP) is a common postural dysfunction caused by imbalances in the anterior and posterior musculature of the neck and upper shoulders. FHP affects the cervical spine and presents with a forward protrusion of the head, and is estimated to be present in 63-67% of college students [22,23]. This postural malalignment is exacerbated by prolonged screen usage, particularly mobile phone usage, and has been colloquially referred to as ‘text neck’ [24-28].
Mobile phone usage places the craniovertebral angle (CVA) at 33-45 degrees on average [27], which increases the mechanical load on the neck, leading to pain and dysfunction [29-31]. FHP can lead to a multitude of etiological complications such as temporomandibular joint dysfunction syndrome [32,33], headaches [34], and thoracic outlet syndrome [35], and chronic neck pain [36-38]. Neck pain is the fourth largest cause of disability globally [39]; therefore, addressing this issue is important - particularly given that neck musculoskeletal disorders impact late adolescence at almost the same rate as adults [40].
To our knowledge, no investigations have been done to examine self-reported ratings of posture and the interrelationships between function, knowledge of rehabilitation exercises, and psychological disposition in college-aged students. With nonverbal communication literature demonstrating a clear link between posture and psychology, the aim of this study was to perform an investigative survey on how posture affects daily living, neck disability, and mental health in a college-aged population. We hypothesized that there would be a statistical relationship between posture, neck disability, and psychological disposition. Specifically, we expected that those who report their posture as being poor or in need of improvement would report worse psychological outcomes and higher levels of neck disability as measured by the survey. This would demonstrate the importance of healthy lifestyle habits for this population and provide the rationale for future research in this subset.
A self-reported exploratory survey was conducted during a 15-week spring semester on a large south-central campus in the United States. Participants were recruited via social media, printed flyers, in-person contact, and email distribution which allowed for a broader sample size. Participants clicked a hyperlink or scanned a QR code to take the survey through their own personal devices (e.g., phone, laptop, tablet). Each survey was anonymous and completed through the secure online QuestionPro survey system. The QuestionPro system ensures all data collected using the platform is fully compliant including data portability, data protection, consent and other compliance features according to General Data Protection Regulations (GDPR).
QuestionPro meets globally recognized international standards for managing risks related to the data security. The average completion time for the 43 questions was 8 minutes. The study was approved by the Institutional Review Board at the university. Study participants electronically signed an informed consent document before completing the survey questions. Inclusion criteria were: college-aged students (18-26 years-old). Exclusion criteria were: Current/acute upper extremity injury, history of surgery to upper body, head, neck, back or upper extremities, history of cervical fractures, stenosis, or disc herniation, history of cervical or brachial nerve related injury, neurological symptoms to the upper limb, diagnosed musculoskeletal pathologies (acute or chronic) in the upper extremity, congenital defects, or inner ear issues/vertigo. This study was developed with an exploratory aim to assess the psychological and physical effects of posture in college-aged populations. No power analysis was performed to determine sample size, instead, a maximal number of participants were recruited. Only completed surveys were used in the subsequent statistical analysis.
Demographics: The first survey section consisted of questions regarding demographic data (age, height, weight, sex, ethnicity) and physical activity level based upon the Tegner Activity Scale to gauge exercise participation levels of the participants. This activity questionnaire asked participants to rate their current levels of exercise from zero (avoiding exercise) to ten (running over 25 miles per week or comparable physical activity). Although the Tegner Activity Scale was initially developed for knee injury populations, the data collected provided general data related to self-reports of physical activity.
Self-reported assessment of posture: The second section consisted of six questions pertaining to posture and daily living that were written by the research personnel. Of these six questions, four of these were binary yes/no questions relating to feelings about posture and presence of pain. Asking participants ‘Do you wish your posture was better’ was aimed to identify the desire for posture improvement, while questions relating to upper body pain were designed to illuminate the participants’ current levels of discomfort. Questions about ergonomics were used to identify participants’ awareness of factors that might influence posture and pain. The remaining two questions asked participants to rate their standing and sitting postures from Very Poor (1) to Very Good (4). These questions were used to gauge an individual’s ability to recognize their own postural deficiencies.
Patient-rated outcomes: The third section contained patient-rated outcomes including the Neck Disability Index (NDI) and the Dispositional Positive Emotion Scale (DPES). The NDI is a ten-item questionnaire pertaining to daily living and functioning for neck pain and disability. Each question is ranked on 6-point scale from full-function to completely disabled. Scores are then cumulated, and participants are ranked into categories of disability from no disability (score 0-4) to completely disabled (score > 34). The NDI form has been shown to be a valid and reliable form used to assess neck pain and function in both non-specific and pathological neck disorders [41,42]. Psychological measures were the next topic measured, and these 5 questions were gathered from the DPES - specifically, the Pride subscale. These questions addressed many of the psychological and nonverbal communication ramifications of poor head and shoulder posture that pertain to self-esteem, emotion, dominance, and submission [19-21,43,44]. The DPES-Pride subscale was chosen because the 5 questions utilized reflect findings on the nonverbal communication ramifications of FHP. These ramifications include postures indicating submissiveness and lacking dominance, and individuals’ attempts to appear smaller to decrease attention [19,45]. These questions are scored from 1 to 7 with higher numbers associated with stronger agreement with the specified statement. Scores are calculated and averaged over the 5 questions; therefore, higher average scores indicate greater levels of positive emotion.
Rehabilitation Technique Knowledge: The fifth section on rehabilitation techniques was used to determine the participant’s knowledge of the various rehabilitation interventions used to treat postural dysfunction. Fifteen options were given that encompassed a variety of exercise, stretching, and manual therapy techniques commonly used to treat postural dysfunction. Participants were asked to select as many techniques as necessary based on their knowledge levels. Of the fifteen different rehabilitation techniques, seven were manual therapy based and required a trained professional, and the remaining eight were variations of exercise modalities.
Functional range of motion self-assessment: The final section included functional testing that participants performed through a series of range of motion (ROM) tests to measure the mobility and function of their shoulders and neck (Figure 1). ROM tests included cervical range of motion measurements and shoulder flexion, shoulder internal and external rotation. Cervical range of motion measurements were taken for; lateral flexion where participants aimed to touch their ear to the three fingers of the hand (Figure 1a and Figure 1b), lateral rotation with a passing grade scored if the participants nose was over their shoulder (Figure 1c and Figure 1d), and cervical flexion which scored a passing grade if participants successfully touched their chin to their chest (Figure 1e). Shoulder flexion was assessed with the participant sitting on the ground against a wall (to remove compensation) and raising arms overhead - an attempt was deemed successful if the participant’s straight arms touched the wall (Figure 1f). For shoulder internal and external rotation, the Apley’s Scratch test was used and passing grades were given if fingers of opposite hands were able to touch (Figure 1g and Figure 1h). All measurements were performed bilaterally and scores of pass or fail, based upon the qualification criteria provided, were self-reported by the participant.
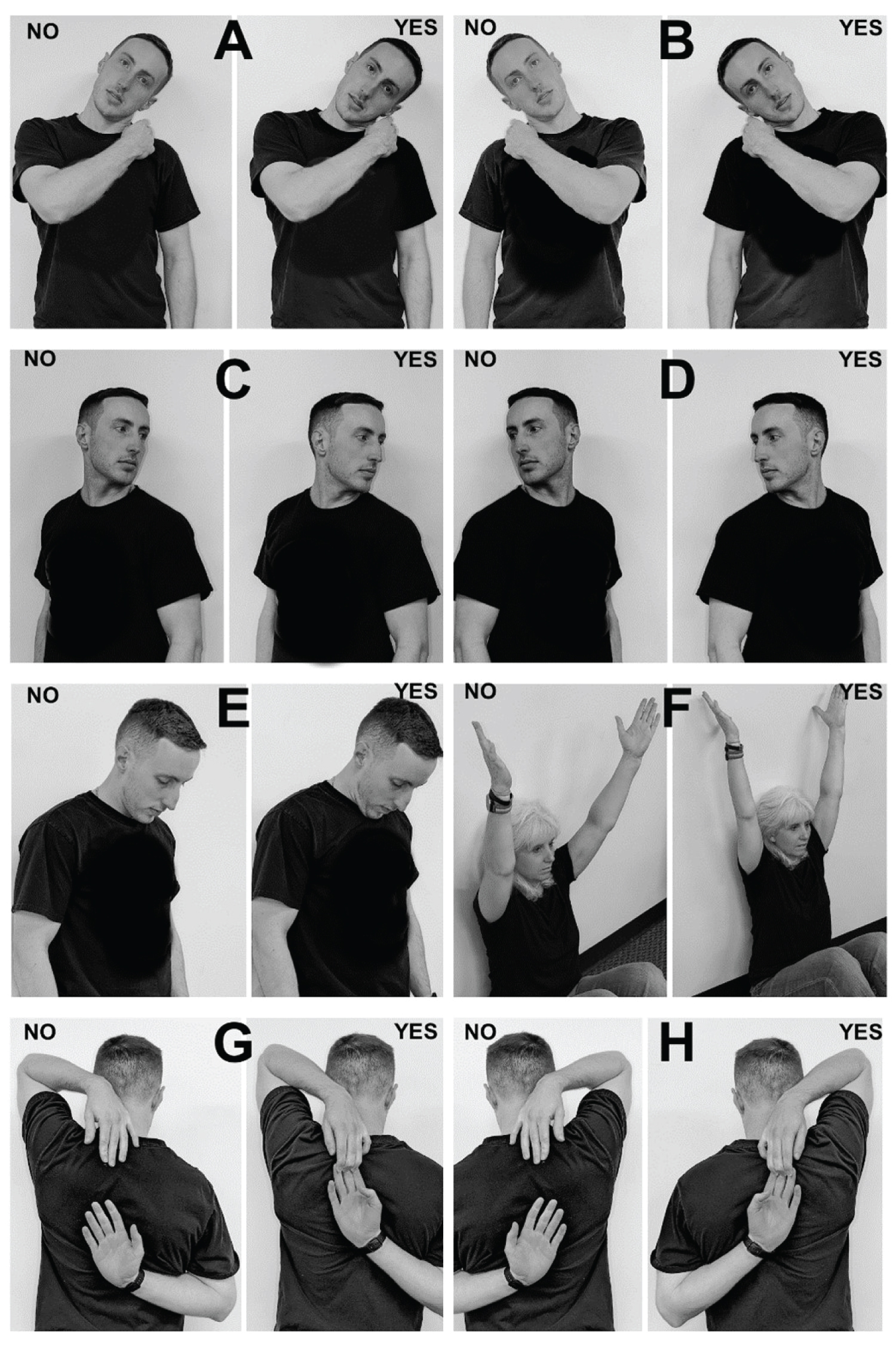 Figure 1: Cervical spine and shoulder range of motion tests. (a) Lateral Cervical Flexion (left); (b) Lateral Cervical Flexion (right); (c) Cervical Rotation (left); (d) Cervical Rotation (right); (e) Cervical Flexion; (f) Seated Shoulder Flexion; (g and h) Apley’s Scratch Test. ‘No’ indicates failure of test, ‘Yes’ indicates passing of test.
View Figure 1
Figure 1: Cervical spine and shoulder range of motion tests. (a) Lateral Cervical Flexion (left); (b) Lateral Cervical Flexion (right); (c) Cervical Rotation (left); (d) Cervical Rotation (right); (e) Cervical Flexion; (f) Seated Shoulder Flexion; (g and h) Apley’s Scratch Test. ‘No’ indicates failure of test, ‘Yes’ indicates passing of test.
View Figure 1
Statistical analysis: QuestionPro data analytics and Excel statistical packages were used to report and analyze quantitative data. Descriptive statistics and Pearson correlation coefficients (r) were used to report and compare data across the survey subsections.
Our survey captured 174 responses from college-aged students; however, 158 participants met the inclusion criteria for the study and completed the survey in its entirety. The majority of participants were located at a south-central-based university in the United States of America; however, the survey was disseminated to other institutions through social media. Female participants comprised 63% of the total (Table 1). On average, participants ranked their activity level as 6.8 out of 10, which indicated that participants typically run about 6 to 10 miles per week, walk about 7 to 13 miles per week or spend about 1 to 3 hours per week in comparable physical activity. All BMI ranges fell within the healthy limit as defined by scoring less than 25.0.
Table 1: Demographic data. View Table 1
Responses from self-reported posture ratings and feelings towards posture are presented in Table 2. Participants largely agreed that their posture could be better and tended to rate their sitting posture as worse than their standing posture. Pain or discomfort in neck was also common during sleeping on the back. Males also tended to feel more positively about their posture when compared to females. However, only 6.2% and 3.7% rated their posture as ‘Very Good’ for standing and sitting posture respectively, specifically outlining that there was no room for improvement. Standing posture was more commonly categorized as ‘Good but could be better’ (60%), while over 75% of participants rated their sitting posture as ‘Very Poor’ or ‘Poor and Needs Improvement’. Eighty-eight percent of participants wished their posture was better, and sitting posture was more commonly rated as ‘Poor and Needs Improvement’ than standing posture (53.8% & 31% respectively). Regarding pain during sedentary tasks such as sleeping or sitting, 36.7% and 51.9% reported pain when completing these two tasks (Table 2). It should be noted that this population was required to be free from any diagnosed acute or chronic musculoskeletal condition to be eligible for this survey study.
Table 2: Self-reported posture ratings and feelings towards posture. View Table 2
Of the 158 participants, 65.2% reported having ‘No Disability’ per the NDI scoring system - meaning they had cumulative scores of 0 to 4 for the 10 questions. Despite the inclusion criteria specifying no acute or chronic musculoskeletal injury to the neck or upper body, 32.3% and 2.5% of participants scored ‘Mild Disability’ and ‘Moderate Disability’ respectively. No participants qualified as ‘Severe Disability’ or ‘Complete Disability’. Of the ‘Mild Disability’ scores, 41 females (41%) scored in this category. For the DPES scoring, the average male score was a 5.6 ± 1.0 and the average female score 5.4 ± 0.9. The lowest score for the individual questions in both groups was the question asking ‘People Usually Recognize My Authority’ with scores of 5.2 ± 1.6 and 4.9 ± 1.4 for males and females respectively. Interestingly, female participants scored lower on the question ‘I Feel Good About Myself’ (5.0 ± 1.4 vs. 5.6 ± 1.6). There was a positive moderate-strong correlation between poor sitting and standing posture (r = 0.61) and presence of pain when attempting to sleep on their back and pain between the shoulders when sitting (r = 0.55). Negative moderate correlations were seen between the desire to improve posture and a participant’s self-rating of their standing (r = -0.43) and sitting (r = -0.47) postures, in addition to NDI scores and presence of pain when sleeping (r = -0.46) or sitting (r = -0.47) (Table 3). Weak correlations (r < 0.30) were found between self-rating of posture and NDI and DPES scores, which indicated little relationship between posture beliefs, neck disability, and psychological wellbeing scores (Table 3).
Table 3: Correlational data between self-reported posture beliefs and patient-rated outcome scales. View Table 3
The eight self-assessments of functional range of motion produced mostly passing values across both neck and shoulder range of motions. The percentage of participants that recorded a pass for the neck range of motion assessments are as follows: Cervical Forward Flexion (94.3%), Cervical Lateral Flexion (Right) (84.8%), Cervical Lateral Flexion (Left) (83.5%), Cervical Rotation (Right) (94.9%), and Cervical Rotation (Left) (92.4%). The percentage of participants that recorded a pass for the shoulder range of motion assessments are as follows: Seated Shoulder Flexion (88.6%), Apley’s Scratch Test (RA over) (72.2%), Apley’s Scratch Test (LA over) (56.3%).
Figure 2 contains data demonstrating that cupping and acupuncture techniques yielded the largest recognition rate amongst the manual therapy techniques (59% and 39.1% respectively), while stretching and resistance training topped the exercise modality list (88.8% and 80.7%). Feldenkrais, Alexander, and Rolfing techniques were the least known rehabilitation techniques with 3.1% of participants being familiar with each of those. Only 2.4% of participants did not recognize any of the fifteen techniques listed (Figure 2).
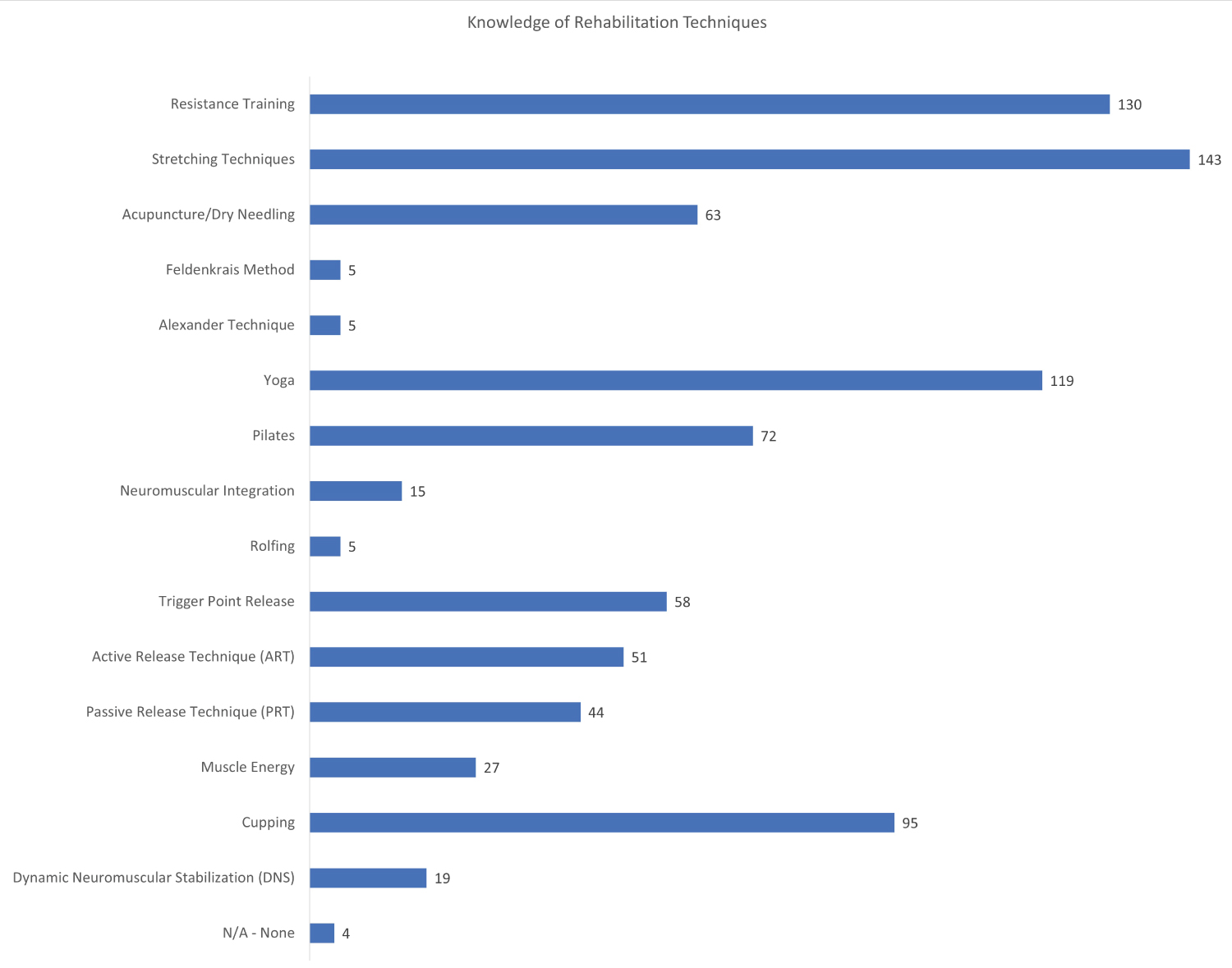 Figure 2: Knowledge of rehabilitation techniques.
View Figure 2
Figure 2: Knowledge of rehabilitation techniques.
View Figure 2
The aim of this study was to perform an investigative survey on the impacts posture has on daily living, neck disability, and mental health in college-aged populations. The main findings of the study observed that only 6.3% and 3.8% of participants reported their posture as not needing improvement while standing and sitting, respectively. Additionally, despite inclusion criteria specifying participants be healthy and free of acute or chronic injury, 36.7% and 51.9% reported pain between their shoulders when attempting to sleep on their back and while sitting, respectively. These two findings highlight two key aspects of concern: 1) that college-aged students recognize their posture needs improvement, and 2) that it is impacting their ability to be comfortable in two basic rest positions. The hypothesis that there would be relationships between self-reported posture and measures of disability and psychological disposition were unfounded.
When comparing these self-reported measures to validated outcomes such as the NDI, 34.8% (n = 55) of participants reported having some level of disability based on the NDI’s scoring parameters. Of these, 92.2% were classified as ‘Mild Disability’, and 7.8% as ‘Moderate Disability’ per the NDI classification index. It should be reiterated that all participants were free from acute injury and had no history of surgery to the upper extremities or torso. The average NDI score was 4.6 ± 4.3 which is slightly lower than those seen by Ahmed, et al. [46] (5.9 ± 2.3) and Gong, et al. [47] (7.0 ± 5.8) who also investigated college-aged populations.
The DPES consists of seven subscales that aim to measure the propensity for an individual to feel positively towards others in their daily lives amongst the various subscales. The Pride subscale specifically was chosen because the questions asked aligned closely with nonverbal communication findings that individuals with poor posture would display less pride and more submissiveness as noted by Mehrabian [45], Burgoon and Dunbar [19], and the work by Coulson [43]. Shiota, et al. [48] demonstrated that the DPES-Pride subscale had a moderate correlation with Extraversion, and a moderate negative correlation with Neuroticism - two of the five traits in the Big Five Inventory (BFI) of personality traits [49]. We reported a weak positive correlation between participants’ thoughts about their sitting and standing posture, and their scores in the DPES-Pride subscale.
Arguably the biggest strength of this study was the high number of college-aged participants that self-reported patterns of poor posture. Sitting posture had 35 participants (22.1%) rank themselves as having ‘Very Poor’ posture compared to the 4 participants (2.5%) who ranked themselves as having ‘Very Poor’ standing posture. This is particularly noteworthy considering that 62.7% of individuals did not believe their workplace was ergonomically set up. With the onset of the COVID-19 pandemic, education systems employed online and hybrid delivery methods for college-aged populations, thereby reinforcing a sedentary lifestyle which is a risk factor for bad posture. Although our participants did not exhibit deviations in functional range of motion in their neck and shoulders, their knowledge of rehabilitation techniques to fix these bad postures was clearly biased to more traditional methods such as resistance training, stretching, yoga, and cupping, with little to no knowledge about posture-specific rehabilitation techniques such as the Feldenkrais Method and Alexander Technique.
Additionally, the breadth of the survey questions allowed for multiple facets to be assessed related to posture. Nonverbal communication literature has long supported the relationship between posture and psychological disposition through the notable works of Dr. Albert Mehrabian and Dr. Judee Burgoon in particular [19,20,45]. As such, it is easy to see this study as a precursor to future more detailed studies on the various aspects investigated, particularly with a larger emphasis on the relationship of posture to psychological outcome measures. We only used one psychological subscale in this study, but we encourage future studies to investigate other domains that encompass physical, mental, and social aspects of health.
Some limitations of the study were how geographically bound the participants were, and not recording the participant’s dominant side. Seventy-three percent of the participants in this study were in the south-central region of the United States which limits the ability for these results to be generalized over all college-age populations. Additionally, not recording the dominant hand during functional assessment tasks, makes analyzing the movement impairments difficult to categorize based on left- or right-handedness. Future studies would be wise increase the breadth of participants involved to get a better understanding of posture beliefs and their impacts across a broader population. Furthermore, including more patient-rated outcome scales would allow for a better understanding of the relationship between postural beliefs and mental health status.
This study reinforces the notion that posture issues are prevalent in today’s society amongst both college-aged and adult populations [22,50]. Results from this study clearly show that participants were able to identify their poor posture and recognize their need to improve it in both sitting and standing settings, but they may not be familiar with rehabilitation techniques that are designed to improve or maintain posture.
Identifying that we have an issue with posture and the prevalence of pain in healthy, college-aged populations demonstrates the need for intervention in this population. Interventions could not only improve an individual’s health, but also reduce the potential for future impact on a society level through health care costs and loss of work productivity.
Future research should aim to focus on measuring posture in college-aged populations to investigate if individuals who identify as having “bad posture” indeed have less desirable posture as determined by measures such as craniovertebral angle and scapular index. If such relationships exist, interventions can focus on musculoskeletal intervention, and education of good postural habits.
There was no funding received for this work.
All authors have contributed equally.