Cervical radiculopathy can lead to severe pain and disability. The study compared the effects of sustained natural apophyseal glides (SNAG) and mechanical cervical traction (MCT) in the management of patients with cervical radiculopathy.
Forty seven patients (male: n = 24, female: n = 23) from the Physiotherapy Department, Usmanu Danfodiyo University Teaching Hospital, Sokoto were recruited for the study. Subjects were randomly allocated to SNAGS or MCT group. Subjects in SNAGS group received SNAG twice weekly for six weeks while subjects in MCT group received mechanical cervical traction, for 15 minutes twice in a week for six weeks. Pain intensity, disability and range of motion were examined at baseline, 3rd and 6th weeks of each treatment session. Descriptive and inferential statistics were used to analyze the data. The alpha level was set at < 0.05.
The result at the 6th weeks showed a significant difference (F = 8.83, p < 0.001) between the pain intensity of participants in the SNAGS (0.38 ± 0.49) and MCT (0.57 ± 0.68) groups. A significant difference (F = 2.15, p < 0.001) between the neck disability of participants in the SNAGS (2.71 ± 2.47) and MCT (5.04 ± 03.46) groups and a significant difference (F = 11.06, p < 0.001) between the right side flexion of participants in the SNAGS (49.17 ± 05.65) and MCT (50.19 ± 08.30) groups were obtained.
It can be concluded that MCT reduces disability, increases range of motion better but SNAGS reduces pain intensity more.
SNAGs, Cervical traction, Pain intensity, Neck disability, Range of motion
Cervical radiculopathy is a dysfunction of a nerve root of the cervical spine. The seventh (C7; 60%) and sixth (C6; 25%) cervical nerve roots are the most commonly affected [1,2]. The common factors of neck pain leading to cervical radiculopathy include poor posture, depression, anxiety, aging, acute injury and occupational and sporting activities [3,4]. This leads to altered joint mechanics, muscle structure or function and can result in mechanical neck pain [5]. Gattermann, and Peterson and Bergmann, stated that the most common cause of mechanical neck pain is zygoapophyseal joint locking and muscle strain [5,6]. Although neck pain leading to cervical radiculopathy originates from a variety of spinal tissues, the cervical nerve roots have been shown to be vulnerable to injury resulting from foramina impingement, disc herniation, direct spinal trauma, and/or foraminal stenosis and there are no universally accepted criteria for the diagnosis of cervical radiculopathy [7,8].
Cervical Sustained Natural Apophyseal Glides (SNAGS) is a popular manual therapy technique used widely in the treatment of painful and restricted neck movement [9]. Its clinical application was based almost exclusively on convention, with little attempt to provide a biological basis and little, if any, empirical evidence as yet to support its efficacy [9]. A study by Ojoawo, et al., on the therapeutic efficacy of cervical traction in the management of cervical radiculopathy; a significant improvement in the pretreatment and post-treatment pain intensity and neck functional disability of participants in experimental group, and a significant difference in the post-treatment pain intensity between the cervical traction and control group were reported [10]. Thus, both SNAGS and MCT have been reported to effect changes in the symptoms and disabilities accompanying cervical radiculopathy [9,10]. This study was designed to explore the effects of SNAGS and MCT on cervical radiculopathy to determine which one is more effective. MCT needs kits for its application, SNAGs needs skill for effective operation, if anyone is found better, effort may need to be directed to the treatment that yield a better result. This will be highly beneficial to both the therapists and patients in term of time and cost.
Ethical approval (IPH/OAU/12/673) was obtained from the Health Research and Ethics Committee of Institute of Public Health of the Obafemi Awolowo University Ile-Ife, Nigeria before the commencement of the study; a copy of the approval was taken to Usmanu Danfodiyo University Teaching Hospital, Sokoto-Nigeria for the data collection. An informed consent was obtained from each subject for the study. The quasi experimental study recruited purposively patients with cervical radiculopathy attending the Outpatient Physiotherapy Clinic of the Usmanu Danfodiyo University Teaching Hospital, Sokoto-Nigeria for physiotherapy treatment. They were referred from the Orthopaedic Clinic of the same hospital with the diagnosis of cervical radiculopathy. The features of patients recruited for the study includes: patients diagnosed with unilateral cervical radiculopathy of mechanical origin of not less than three months with a positive response to Spurling's test. However among those patients, those with history of vertebro-basilary artery insufficiency, history of cervical surgery or arthroplasty, also those that presented with malnutrition, fever and tumors were excluded from the study. Purposive sample technique was used to recruit 47 patients with cervical radiculopathy using a formula for a study comparing two means according to Rosner, [11] (24 for SNAGS and 23 for MCT).
Instruments use in the study includes; Visual Analogue Scale (VAS), Neck Pain Disability Index (NDI) Questionnaires, inclinometer: cervical traction kit: A 0.45 kg over-the-door cervical traction unit with calibrated weights made from United Kingdom; stadiometer: this consists of height meter and weighing scale made by Seca, United Kingdom to measure the height and bodyweight of subjects respectively, weighted 250 kg,. The pre-eligibility tests carried out to screen all participants were: Skin rolling, cervical mobility tests and range of motions, Spurling's diagnostic Tests and X-ray. The participant's weight, height, cervical range of motion, pain intensity and neck disability were measured pre-treatment, 3rd and 6th week of treatments using appropriate instruments.
Subjects allocated into two groups SNAGS and MCT using simple randomization protocol of fish and bowl method. In this method, an envelope contained 47 small paper wraps was used. Twenty four were inscribed with SNAGS group and 23 with MCT. Once a subjects came to the research centre and found eligible, he was asked to pick a paper from the envelope, and all subjects that picked SNAGS were in SNAGS group while subjects that picked MCT was in MCT grouped Figure 1.
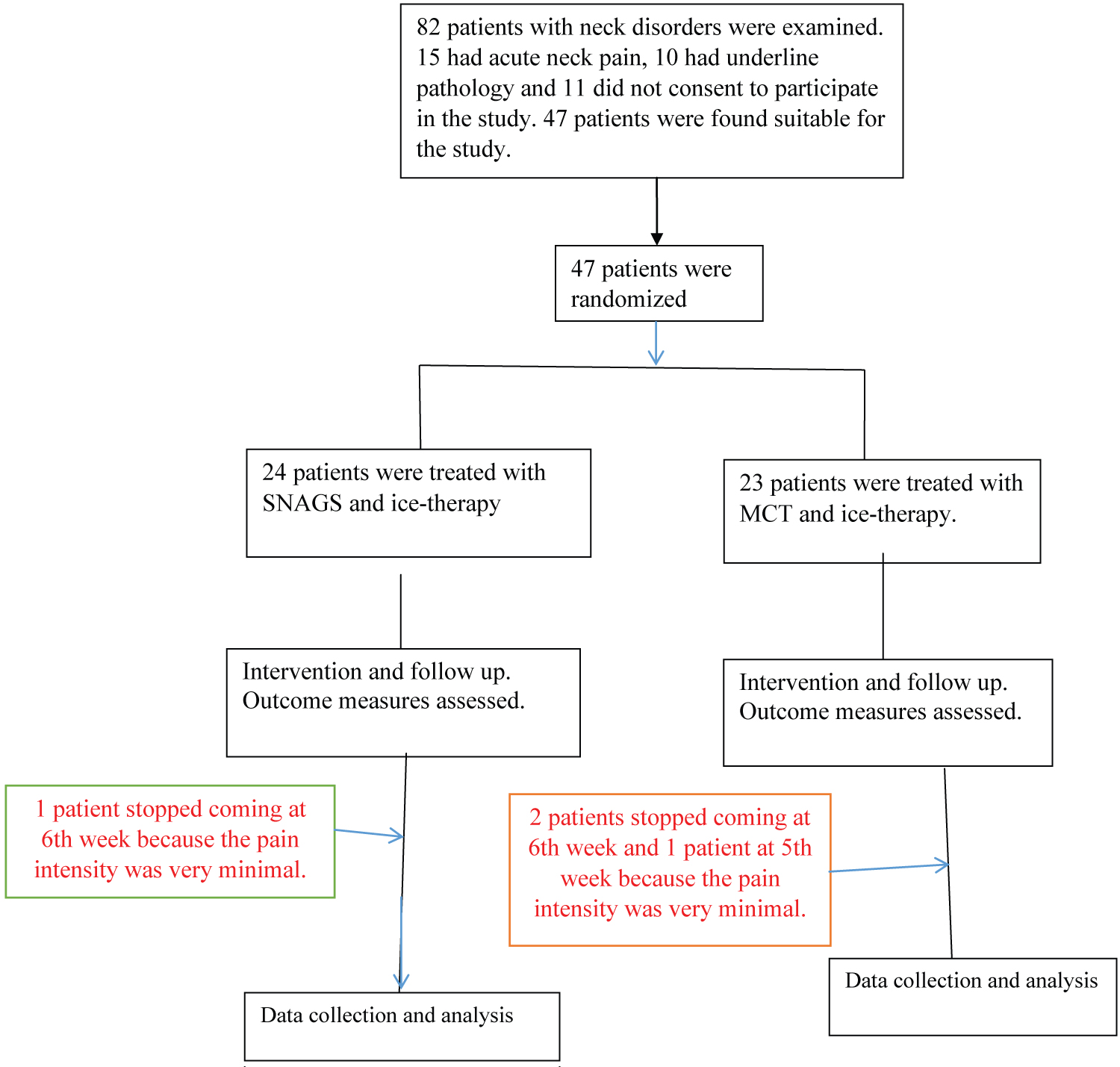 Figure 1: Flow chart for the Randomised Controlled Trial (RCT).
View Figure 1
Figure 1: Flow chart for the Randomised Controlled Trial (RCT).
View Figure 1
For SNAGS group, Sustained Natural Apophyseal Glides (SNAGS) with active arm movement: Each subject in this group was given SNAGS on cervical vertebra with simultaneous active mobilization of arm movement (MWM) [12]. Subject was in a sitting position. the researcher placed one thumb reinforced over the other on the spinous process of the implicated cervical vertebra, then applied pressure anteriocranially on the spinous process, the pressure was sustained for 60 secs maximum [13,14] as the patient concurrently performs shoulder abduction of the affected upper limb [15]. On each visit SNAGS was used twice a week for six weeks.
Patient was on sitting position. A strap was affixed under the chin of the patient. This chinstrap was then connected over a pulley to the weights. The chinstrap was connected to calibrated weight that was held aloft over a door way via pulleys. The weight was measured in kilogram to 10% of the patient's total body weight [16]. Sustained cervical traction was applied by means of a halter, aiming to give equal pull on the chin and the occiput using a simple rope and pulley system that can be suitably loaded. The patient's head was positioned in a slight extension (approximately 25° angle of pull). Patient was instructed to observe a gentle pull on their head and neck when the traction was applied and it was important to relax when traction effect is felt. On each visit MCT was applied for 15 minutes twice a week for six weeks [17].
Cryotherapy - in form of 0.5 kg ice pack was placed for 7 minutes on the posterior aspect of the neck; each subject was in a prone lying position with pillow under the chest and the head supported by a small, rolled towel in a neutral position. Ice pack was placed from neck base (behind the ear) to supra clavicular and scapular regions for 7 minutes according to Algafly [18].
Pain intensity: The initial pain intensity was measured using Visual Analogue Scale (VAS), a 10 cm baseline, the beginning indicating no pain while the end of the line indicates worst pain, patient was asked to indicate where the pain was in relation to the two extremes, measures from the left hand side. This was measured pretreatment, third week of treatment and sixth week of the treatment project.
Neck disability: This was measured with the Neck Pain Disability Index (NDI) questionnaire. The questionnaire was given to the patient to fill at the baseline in order to assess the level of disability according to Fairbanks, et al. [19], it contains 10 items, 7 related to activities of daily living, 2 related to pain, and 1 related to concentration [20]. Each item was scored from "0 to 5" interpreted as "no pain at the moment to the worst pain imaginable", respectively and the total score was expressed as a percentage, with higher scores corresponding to greater disability. Westaway, et al., [21] identified the minimum detectable change as 5 (10 per cent points) in a group of 31 patients with neck pain. Stratford and colleagues, identified the minimum detectable change to be 5 (10 per cent points) in a group of 48 patients with neck pain and arm pain [22]. This was measured pretreatment, third week of treatment and sixth week of the treatment project.
Cervical range of motion: Cervical Right Side Flexion and Right Rotation were measure using inclinometer because the radicular pain of almost all the patients was towards right side, there was no restriction toward left side. The Outcome Measures were applied 3 times, pre-treatments, 3rd and 6th week treatments. This was measured pretreatment, third week of treatment and sixth week of the treatment project.
SPSS version 23.0 (SPP Inc., Chicago, Illinois, USA) was used to analyze the data. A P value of 0.05 was considered as statistically significant. The data was analyzed using descriptive and inferential statistics. Independent t test, was used to compare the physical characteristics between the two groups; repeated measured ANOVA was used to compare the pre-treatment, 3rd week and 6th week mean values of PI, DI cervical range of motion in flexion and rotation in SNAGs and in MCT groups. Repeated measured ANOVA was used to compare the pre-treatment, 3rd week and 6th week mean values of PI, DI cervical range of motion in flexion and rotation between SNAGs and in MCT groups. Post hoc analysis using LSD was carry out where appropriate.
Presented in Table 1 are the mean values of weight, height and BMI for SNAGS and MCT group. The means values of weight, height and BMI were 78.39 ± 14.06 kg 01.71 ± 00.08 m, and 26.85 ± 04.89 kg/m2 respectively for SNAGS while that of MCT group were 75.87 ± 16.21 kg, 1.70 ± 00.08 m and 26.32 ± 05.77 kg/m2 respectively. There was no significant difference (P > 0.05) in any of the variable when the two groups were compared.
Table 1: Comparison between physical characteristics of the subjects in SNAGS and MCT groups. View Table 1
Presented in Table 2 is Repeated measure ANOVA comparing the mean values of the pre-treatment, 3rd and 6th week treatment of participants in SNAGS Group. The results revealed that there was significant difference in the PI of pre-treatment, 3rd and 6th weeks treatment (F = 521.35; p < 0.001). The results revealed that there was also significant difference in the NDI of pre-treatment, 3rd and 6th week treatment (F = 102.55; p < 0.001). Considering the cervical range of motion, there was significant increase in right flexion (F = 16.86; p < 0.001) and right rotation (F = 31.35; p < 0.001) when the pre-treatment, 3rd and 6th week of cervical range of motion in SNAGS Group were compared.
Table 2: Summary of repeated measure ANOVA with Post hoc analysis comparing the pre-treatment, 3rd and 6th weeks values of PI, NDI and CRM of SNAGS group (N = 24). View Table 2
Presented in Table 3 is Repeated measure ANOVA comparing the mean values of PI and NDI of the pre-treatment, 3rd and 6th weeks treatment of subjects in MCT Group. The results revealed that there was significant difference in the PI of pre-treatment, 3rd and 6th week treatment (F = 989.68; p = 0.000). The results also revealed that there was significant reduction when the pretreatment ND was compared with 3rd week and 6th week treatment (F = 102.55; p = 0.000). Considering the cervical range of motion, there was a significant increase in right flexion (F = 17.80; p < 0.001) and right rotation (F = 23.95; p < 0.001) when pre-treatment, 3rd and 6th week of cervical range of motion of MCT Group were compared.
Table 3: Summary of repeated measure ANOVA with Post hoc analysis comparing the pre-treatment, 3rd and 6th weeks values of PI, NDI and CRM of MCT group (N = 23). View Table 3
Presented in Table 4 is repeated measured ANOVA comparing the mean values of the pre-treatment, 3rd week and 6th week of PI, NDI, cervical range of motion in flexion and rotation of participants in SNAGS and MCT groups. There was no significant difference in pretreatment (p > 0.05), outcome measures when the SNAGS and MCT groups were compared. However, SNAGS reduces PI significantly (F = 8.83, p < 0.000) than MCT at 6th week whereas MCT reduces NDI significantly (F = 2.15, p < 0.000) more than SNAGS at 6th week of intervention. Considering the cervical range of motion, there was a significant difference in 6th week treatment of right side flexion (F = 11.10; p < 0.0001) and right rotation (F = 18.47; p < 0.001) cervical range of motion when SNAGS and MCT Groups were compared.
Table 4: Shows comparison between pre-treatment, 3rd week and 6th week values of PI, NDI and CRM of SNAGS group and MCT group (N = 47). View Table 4
Shown in Table 5 is the interaction effects of pain intensity, right flexion and rotation on neck disability and the interaction effects of each of the variable on each other. There was a significant (F = 10.54, p < 0.001) interaction effect among the variables, however, only pain intensity displayed a significant effect on neck disability (F = 10.000, p < 0.001). There was no significant interaction effects on pain intensity and right side flexion (F = 1.56, p > 0.05).
Table 5: Interaction effects among PI, ND and CRM in the two group (N = 47). View Table 5
The purpose of this study was to evaluate the effects of SNAG and MCT on pain intensity, disability and range of motion of patients with cervical radiculopathy and to examine which one can be more effective.
It was observed from the study that sustained natural apophyseal glides SNAGS was found to produce significant reduction in pain intensity. This supported the report of Nikeeta, [23] that SNAGS produced instant relief in mechanical induced neck disorder with pinched nerves (radiculopathy). The reduction in pain intensity could be deduced to the fact that SNAGS produces sympatheoexcitatory effect which is instrumental to the production of analgesic response in C5/6 [24]. Abdelgalil, compared and reported effectiveness of both high velocity low amplitude manipulation (HVLA) and sustained apophyseal glides on pain and range of motion in patients with mechanical neck pain, the instant reduction observed was deduced from the instant release of nociceptive as suggested by Melzack and Wall [25,26]. A significant reduction in neck disability was also observed as a result of SNAGS intervention in this study. This is in consonant with result presented by Kumar, where he concluded that SNAGS was a useful manual therapy technique for achieving faster result as measured in terms of ROM, NDI and pain at available end ranges in neck disorders compared with other conservative physiotherapy techniques [27].
Mechanical cervical traction was also found to produce significant reduction in pain intensity in this study, this was in accordance with study conducted by Cleland, et al., Ojoawo, et al. and Abid, et al., where MCT produced significant reduction in pain intensity in cervical radiculopathy and improvement on neck disability [10,28,29]. The significant reduction observed was due to decrease in radicular symptoms. Traction distracts cervical neural foramen and decompresses the affected nerve root; cervical traction consists of administering a distracting force to the neck in order to separate the cervical segments and relieve compression of intervertebral disks on the nerve roots Abid [29].
However, comparing the mean values of the pre-treatment, 3rd week and 6th week of PI and NDI of participants in SNAGS and MCT Groups, there was no significant difference in pretreatment, PI and NDI. Indicating that the PI and NDI of the two groups were comparable. SNAGS reduces PI significantly than MCT whereas MCT reduces NDI significantly more than SNAGS at 6th week of intervention as observed in the study. The better reduction of pain intensity by SNAGS more than MCT could be due to instant analgesic effect of SNAG explained by pain gate theory Mendell [30]. The gate control theory of pain, proposed by Melzack and Wall [26] stated that spinal nociceptive transmission neurons receive inputs from low threshold mechanoreceptors, but this input is gated by feed-forward activation of inhibitory neurons located in the substantia gelatinosa of the dorsal horn. It has been hypothesized that the force of manipulations activate both the deep and superficial mechanoreceptors, proprioceptors and nociceptors, resulting in strong afferent impulses to the spinal cord, inhibiting central pain transmission. Vigotsky and Bruhns [31] theorized that manipulation also releases endogenous opioids (encephalis and endorphins) which decreased pain sensation. SNAGS which is a derivative manipulation, the high velocity low amplitude force causes rapid separation of two joint surfaces (cavitation) resulting in stretching of the periarticular tissues, thereby releasing intra and extra-articular adhesions [12]. The cavitation also stimulates joint nociceptors and mechanoreceptors which in turn stimulate the Golgi tendon organs, resulting in somatic afferent receptor activity. The combination of these events rather than the cavitation are what make manipulation effective in breaking the pain cycle, resulting in a decrease in pain and muscle spasm and an increase in joint mobility and soft tissue inflexibility [12].
While traction increases intervertebral disc spaces more than SNAGS resulting in freer cervical range of motion and neck functions. Physiological effects of the manual traction include decompression of articular, neurological and vascular structures; soft tissue lengthening and mechanoreceptors stimulation to provide pain relief and reduction of the muscular tonus [31,32]. In a related study, Abid, et al., [29] found that patients with non-specific neck pain treated with SNAGS and followed by intermittent electrical cervical traction was more effective in reduction of pain and enhancement of function, as compared to those patients treated with SNAGS manual physical therapy techniques alone.
It was observed in the study that SNAG and MCT were effective in reducing cervical range of motion significantly. A study conducted by Elnaggar, et al., [33] revealed that CT reduced neck and arm pain substantially, there was an important improvement in function of the nerve as well as mobility of the neck. In addition, the finding in our study was in tandem with the study conducted by Voltonen, et al. [34], they inferred that traction abased muscle spasm and the electrical activity of muscle was decreased substantially which led to relaxation of the muscle and pain relief and increase range of motion. Cervical traction distracts cervical vertebrae apart, the cervical joint capsule is stretched and the foramina were opened as reported by Krause, et al., [27]. Therefore the range of motion is increased with MCT.
Study have shown that manual therapy including SNAG may released trapped meniscoids, breakdown adhesions, and diminishing distortion in the intervertebral disc, these were brought the alteration of segmental biomechanics [35,36]. Also, a new position of stable equilibrium in the cervical region can be achieved by SNAG, this could be resulted from a relatively large vertebral motions and restoration of segment thought capable of buckling, [37].
SNAG reduces mechanical stress or strain on soft and hard spinal tissues by providing sufficient energy to restore a buckled segment to a lower energy level [38]. Gillette in his proposal mentioned that spinal manipulative therapy possess mechanical thresholds lower than the peak force delivered during a manipulation, and because the receptor types are responsive to dynamic and/or static components of a mechanical stimulus the procedure was able to activates all known mechanosensitive, somatosensory receptors [39]. These were the reasons why SNAGS can effectively reduce cervical range of motion. Considering the interacting effects of the variables, it was observed that there was a significant interaction between pain intensity and neck disability. It could be inferred from the finding that increase in pain intensity will have significant increase in the neck disability of the patient. When there was pain in any part of the body definitely there will be dysfunction of that part of the body. Interestingly, there was no significant effect on pain intensity and right side flexion and rotation, neither did disability has any effect on the range of motion. The implication is that, patient may not have full range of motion and yet it may not significantly affect the function of the cervical region especially some activities in the neck disability questionnaire.
In conclusion, it can be deduced from the study that SNAGS is effective in reducing pain intensity, disability and increasing cervical range of motion in patients with cervical radiculopathy; MCT is also effective in reducing pain intensity, disability and increasing cervical range of motion in patients with cervical radiculopathy but SNAGS effect reduces pain intensity more than MCT while MCT effect reduces disability and increases range of motion than SNAGS.