Preslip capital femoral epiphysis, MRI, Pediatric hip
9-year-old presented with left thigh pain for several weeks. Physical assessment of gait noted external rotation of the left hip.
Anteroposterior and lateral radiographs of the hip demonstrated normal alignment. No fractures or dislocation. In particular, no femoral epiphysis slip was noted. The lateral view first interpreted as normal, although in hindsight there might have been subtle alignment irregularity (Figure 1).
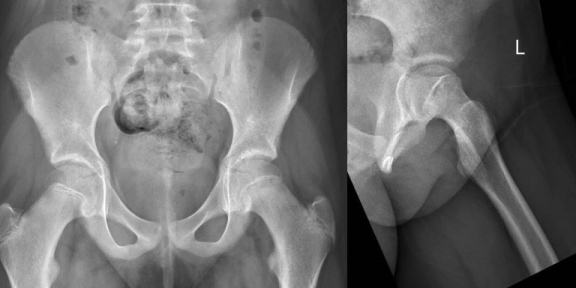 Figure 1: AP radiograph of the pelvis showing normal alignment of the left hip, kline's line (dashed line) intersect part of the femoral epiphysis. Lateral view, there is subtle abnormal alignment of the left femur at the physis with no overt slippage.
View Figure 1
Figure 1: AP radiograph of the pelvis showing normal alignment of the left hip, kline's line (dashed line) intersect part of the femoral epiphysis. Lateral view, there is subtle abnormal alignment of the left femur at the physis with no overt slippage.
View Figure 1
MRI was performed which showed high T2/STIR signal intensity with slight widening of the physeal line of the left hip with no slippage or subluxation of the femoral epiphyses. Mild bone marrow edema of the adjacent epiphysis and metaphysis noted. Minimal joint effusion noted. The acetabulum and contralateral hip were normal (Figure 2).
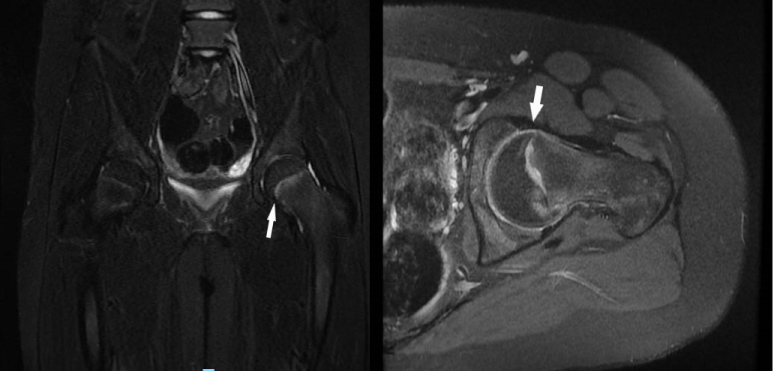 Figure 2: Coronal and axial STIR MRI shows high signal involving the physeal line on the left side with slight widening (arrow). No slippage of the femoral epiphysis. Minimal joint effusion. Mild surrounding bone marrow edema of the epiphysis and metaphysis. Normal right hip joint and proximal femur.
View Figure 2
Figure 2: Coronal and axial STIR MRI shows high signal involving the physeal line on the left side with slight widening (arrow). No slippage of the femoral epiphysis. Minimal joint effusion. Mild surrounding bone marrow edema of the epiphysis and metaphysis. Normal right hip joint and proximal femur.
View Figure 2
Slipped capital femoral epiphysis (SCFE) is a disorder of the adolescent hip that occurs more in males, in which there is a Salter-Harris 1 fracture. The femoral metaphysis commonly displaces anteriorly, superiorly and laterally in relation to the epiphysis [1].
Early detection is important as complications such as avascular necrosis (AVN) of the femoral head, chondrolysis or early development of osteoarthritis may occur [2].
AP and frog leg lateral radiographs are used as first line imaging investigation. Multiple signs are described such as widening and irregularities of the physis compared with the contralateral side; relative loss of height of the epiphysis on AP projections, loss of the anterior concavity of the femoral neck on lateral views, cystic changes at the metaphysis in chronic cases, Kline's line (drawn parallel to the superior margin of the femoral neck which, in healthy hips, usually intersects the epiphysis) may not intersect a portion of the femoral head [3].
Particularly in early cases of SCFE, MRI is sensitive. MRI detects early physeal changes of both preslip and SCFE even when radiographs and computed tomography are normal. MRI signs of an imminent slip include widening of the physis, bone marrow edema, joint effusion and synovitis. It is also useful in detecting complications, assessment of contralateral hip as well as post-operative evaluation of the affected sides in addition to ruling out other differential diagnosis [4].
Our case emphasizes the importance of MRI in cases of suspected preslip phase of slipped femoral capital epiphysis in order to obtain a definitive diagnosis and proceed with early intervention to achieve the best results possible.
None.
The authors have no conflicts of interest to declare.
There are no competing interests; no funding, grants or equipment provided for the project from any source; and no financial benefits to the authors. This article has not been presented in any form previously.
None.