Pectoralis major tendon ruptures are uncommon injuries that are most commonly seen in active males between 20-40 years of age. While the most frequently cited mechanism of injury is during bench press, other causes from activities such as contact sports have also been reported. With the rise in popularity of CrossFit, or high intensity variable functional training, practitioners may begin to notice an increase in other mechanisms of injury. In this clinical case we present a patient who ruptured his pectoralis major tendon while performing a CrossFit workout as a coach.
Z.M. is a 21-year-old right-handed male with no history of supplement use who presented to our clinic with a chief complaint of dominant right arm and shoulder pain as well as loss of mass and contour in the right chest wall. He reported that the initial injury occurred six weeks prior to presentation while performing a "muscle-up" during a CrossFit workout, a compound lift which is a combination of a pull-up and a dip. The patient initially felt a pop in the anterior shoulder that was accompanied by pain/bruising in the chest wall that was exacerbated by horizontal arm adduction. On exam in our Orthopaedic clinic, Z.M. had regained some of his shoulder ROM but the pain and weakness with adduction persisted. An MRI confirmed a rupture and retraction of the sternocostal head of the pectoralis major tendon. Given the chronicity of the injury, surgical repair was offered, and reconstruction was performed via the deltopectoral approach with use of suture anchors augmented by tubularized Achilles tendon allograft.
Subacute pectoralis major tendon ruptures are difficult problems for the athlete and surgeon alike. These are often recognized earlier and classically involves the bodybuilder who experiences immediate and intense pain in the arm, ROM difficulties and the classic chest wall bruising pattern. In this case, the mechanism of injury was unusual and delay in presentation required additional operative considerations. The muscle-up is perceived as an advanced maneuver in the weightlifting and CrossFit communities, which can lead to significant injury when performed repetitively. Practitioners should be aware of the potential injuries this exercise can cause and should educate their patients in regard to recognizing serious muscular trauma when it occurs.
The pectoralis major muscle is a large, broad-based muscle of the upper extremity responsible for adduction, internal rotation and elevation of the glenohumeral joint [1]. The muscle's two portions, the sternocostal head and the clavicular head, combine together then twist to form a common tendon that inserts lateral to the bicipital groove on the proximal humerus. Classically, rupture of the pectoralis major tendon involves the sternocostal contribution of the tendon and more commonly seen in bodybuilders and weight lifters [2]. The most implicated exercise in pectoralis major tendon rupture is the bench press as it places the muscle in a position of maximal tension when it is eccentrically loaded, extended, and externally rotated [1]. Other cited mechanisms of injury in the literature include contact sports such as football and wrestling [1]. CrossFit, or high intensity variable functional training, is a relatively new discipline in fitness that combines plyometric movements, such as squats, pull-ups, and muscle-ups, with high intensity interval training and load resistance [3]. This form of fitness emphasizes "constantly varied, high intensity, functional movement" performed repeatedly as a method of maintaining total body fitness [4]. Despite its growing popularity, little research has been done into the potential musculoskeletal risks that may be associated with this new trend [3]. Some sources have shown a lower rate of injury compared to traditional forms of exercise, while others have demonstrated a higher rate of injury, especially to the knees and shoulders [3,5]. These varied reports are due to the sparse data and likely under-reporting that exists on injuries within the CrossFit community.
In this case study, we will describe a subacute rupture of the sternocostal head of the pectoralis major tendon that occurred while the patient was performing muscle-ups during a CrossFit workout. A muscle-up is a combination exercise that involves combining a traditional pull-up and a triceps dip (Figure 1). This exercise in considered particularly difficult and is a favorite in many elite weightlifting circles.
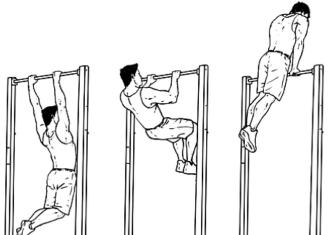 Figure 1: Muscle-up form; This image shows the proper technique for performing a muscle up. The muscle up is a compound exercise that is a combination between a pull-up and a dip.
View Figure 1
Figure 1: Muscle-up form; This image shows the proper technique for performing a muscle up. The muscle up is a compound exercise that is a combination between a pull-up and a dip.
View Figure 1
Z.M. is a 21-year-old right-handed male with no history of supplement use who presented to our clinic with a chief complaint of dominant right arm and shoulder pain as well as loss of mass and contour in the right chest wall (Figure 2). He reported that the initial injury occurred six weeks prior to presentation while performing a "muscle-up" during a CrossFit workout, a compound lift which is a combination of a pull-up and a dip. The patient initially felt a pop in the anterior shoulder that was accompanied by pain/bruising in the chest wall that was exacerbated by horizontal arm adduction. On exam in our Orthopaedic clinic, Z.M. had regained some of his shoulder ROM but the pain and weakness with adduction persisted. An MRI confirmed a rupture and retraction of the sternocostal head of the pectoralis major tendon. Given the chronicity of the injury, surgical repair/reconstruction with use of allograft was offered to which he was amenable since he wanted to return to athletic activity.
 Figure 2: Pre-operative exam; This is a pre-operative photo of the patient taken ~6 weeks post injury. Clinical exam showed ecchymosis of chest wall on his right side accompanied by loss of the axillary fold.
View Figure 2
Figure 2: Pre-operative exam; This is a pre-operative photo of the patient taken ~6 weeks post injury. Clinical exam showed ecchymosis of chest wall on his right side accompanied by loss of the axillary fold.
View Figure 2
Surgical Technique: A modified deltopectoral approach was utilized in which our 5-6 cm incision was curved slightly more medially toward the axillary fold to accommodate for the retracted tendon substance. The cephalic vein was identified and retracted/protected laterally along with the deltoid tendon to expose the clavicular head of the pectoralis major tendon. Deep and distal to the clavicular head, the sternal portion of the pectoralis major was identified and noted to have an 80% tear from proximal to distal was noted with the distal 20% remaining attached to the lateral aspect of the bicipital groove. Further dissection along the chest wall revealed the retracted tendon edge which was encased in fibrotic scar tissue (Figure 3). The tendon was freed from the adhesions and an attempt was made to reduce the tendon back to its native insertion on the humerus with the arm adducted and internally rotated. However, a gap of 2 cm remained between the tendon and its insertion which would necessitate use of an Achilles tendon allograft to augment the repair. A frozen Achilles tendon allograft was thawed and tubularized with 2-0 Ethibond suture to a dimension of 2.5 cm × 7 cm (Figure 4). This allograft was then secured in a running, locking stitch fashion with 2-0 Ethibond to the remaining, native pectoralis major tendon mass (Figure 5). Subsequently, three areas equidistant from one another along the lateral aspect of the biceps groove were decorticated with a high-speed 4 mm burr and three 2.9 mm double-limb Juggerknot (Zimmer-Biomet) all suture anchors were placed. The Maxbraid suture limb was then threaded through the allograft in a running, locking fashion and hand tied individually to secure the tendon back to its native footprint (Figure 6). After each suture was tied off individually, the graft was reinforced along its length with Fiberwire suture in a horizontal mattress fashion. The strength of our repair was then tested by cycling the arm through abduction/adduction and internal/external rotation where the repaired tendon was found to be secure without gaps. The wound was then irrigated with 250 cc of normal saline and local venous bleeding controlled by electrocautery prior to layered closure of the deltopectoral interval with 0 Vicryl, the deep dermal layer closed with 2-0 Vicryl and a running subcutaneous stich with 3-0 Monocryl for the skin.
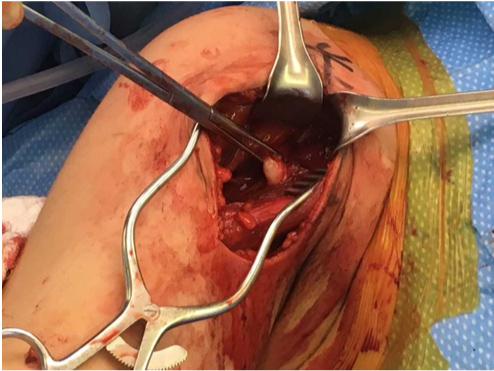 Figure 3: Retracted pectoralis major tendon sternocostal head; This image shows the retracted tendinous mass of the pectoralis sternocostal head taken intra-operatively.
View Figure 3
Figure 3: Retracted pectoralis major tendon sternocostal head; This image shows the retracted tendinous mass of the pectoralis sternocostal head taken intra-operatively.
View Figure 3
 Figure 4: Achilles allograft preparation; This image shows the prepared tendinous portion of the Achilles allograft used during surgery for pectoral tendon augmentation.
View Figure 4
Figure 4: Achilles allograft preparation; This image shows the prepared tendinous portion of the Achilles allograft used during surgery for pectoral tendon augmentation.
View Figure 4
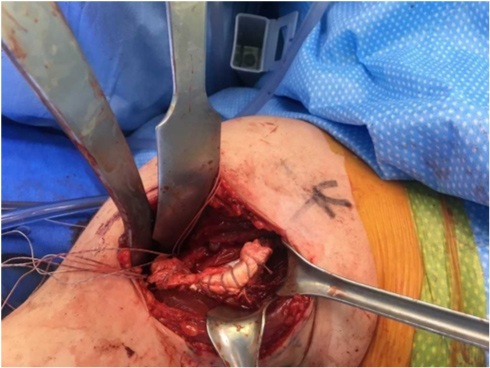 Figure 5: Allograft augmentation; This image shows suturing of the Achilles allograft onto the retracted and remaining sternocostal head portion of the pectoralis major tendon. The allograft was sutured onto the tendon using a running-locking stich using 2-0 Ethibond.
View Figure 5
Figure 5: Allograft augmentation; This image shows suturing of the Achilles allograft onto the retracted and remaining sternocostal head portion of the pectoralis major tendon. The allograft was sutured onto the tendon using a running-locking stich using 2-0 Ethibond.
View Figure 5
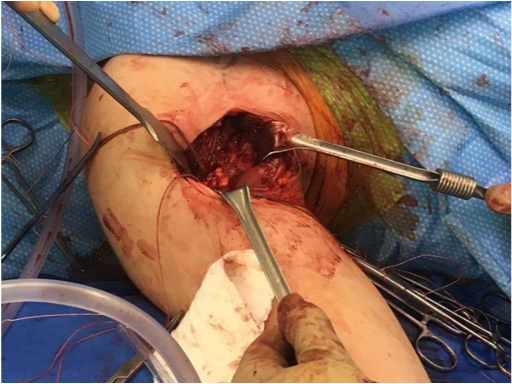 Figure 6: Completed repair; This image shows the augmented repair of the pectoralis major tendon post-fixation into the previously prepared trough using the Juggerknot 2.9 mm suture anchors.
View Figure 6
Figure 6: Completed repair; This image shows the augmented repair of the pectoralis major tendon post-fixation into the previously prepared trough using the Juggerknot 2.9 mm suture anchors.
View Figure 6
Follow up: Patient was last seen in October 2019 for his 5-month follow up. He states that he has been able to return to doing roughly 80% of his workouts, including pull-ups. Patient still is having some residual tightness with push-ups and has not returned to bench pressing or any other overhead weighted exercises. He has been compliant with formal physical therapy and continues to be active at the gym. On physical exam the right axillary fold is symmetric to the left side (Figure 7). Deltopectoral axillary fold incision is well healed and less hypertrophic. Range of motion is symmetric with negative Speed's test. Strength is 5/5 bilaterally with no neurological deficits.
 Figure 7: Post-operation exam; This image shows the patient three months post-procedure. Chest wall contour and mass of the pectoralis major muscle have returned to being symmetrical.
View Figure 7
Figure 7: Post-operation exam; This image shows the patient three months post-procedure. Chest wall contour and mass of the pectoralis major muscle have returned to being symmetrical.
View Figure 7
Pectoralis major tendon ruptures are rare injuries but have been increasing in prevalence with the rising popularity of weight training and lifelong fitness [1,2,6]. Most commonly, rupture of this tendon occurs in males between the ages of 20-40 years-old and often happens while performing the bench press, a popular exercise for many weightlifters [1,2,6]. In this case, the inciting incident was not the bench press or any other less-commonly reported mechanism, but rather unusual in that it was associated with an exercise performed during a CrossFit workout. The muscle-up is a compound exercise that combines the movements of a pull-up and a dip, and as such, it requires coordination of many muscles of the arm, shoulder and chest wall to be performed. This places the rotator cuff and pectoralis major under many of the same stresses that they are placed under during a bench press, particularly if the exercise is not performed with fluidity in motion. As the popularity of CrossFit rises and emphasis on the ability of the participant to perform compound lifts such as the muscle-up, practitioners may notice these types of injuries becoming more frequent. CrossFit is a relatively young discipline in the world of fitness and thus has not been extensively studied, but some researchers do note increased incidence of shoulder and knee injuries in patients who participate in this form of exercise [3,5].
This case study is important because it presents a new and different mechanism of injury for a pectoralis major tendon rupture. This unusual mechanism of injury may have contributed to both the late presentation of the patient as well as the degree to which the torn tendon was retracted. The degree of retraction resulted in the use of an allograft to supplement the tendon to add both length and strength to the native remaining tendon. Though still a rare injury and an even more unique mechanism, both may continue to become more frequent as the popularity of weightlifting and CrossFit continues to increase.
Subacute pectoralis major tendon ruptures are difficult problems for the athlete and surgeon alike. These are often recognized earlier and classically involves the bodybuilder who experiences immediate and intense pain in the arm, ROM difficulties and the classic chest wall bruising pattern. In this case, the mechanism of injury was unusual and the delayed presentation required additional operative considerations. The muscle-up is perceived as an advanced maneuver in the weightlifting and CrossFit communities, but can lead to significant injury when performed repetitively. Practitioners should be aware of the potential injuries this exercise can cause and should educate their patients in regards to recognizing a serious injury when it occurs.
Here we report a clinical case where the patient experienced a rupture of the sternocostal head of the pectoralis major tendon while doing a muscle-up, a popular exercise in the weightlifting and CrossFit communities. Subacute repair was performed using suture anchors to reattach the tendon remnant, augmented with an Achilles allograft for length and strength, along the original footprint of the tendon inserting into the proximal humerus.
This case report was written, and all images obtained with the knowledge and informed consent of the patient.
The author(s) declare that they have no competing interests.
This case report and literature review was performed by medical student WHM with editing and advice from MZ and CD. Surgery performed by MZ and CD and operative information obtained from MZ and CD.