Breast cancer is the most common cancer worldwide and in King Saudi Arabia as well. This study aimed to determine the demographic characteristics and histopathological profile of females with breast cancer attending King Fahad hospital at Albaha-KSA.
Retrospective descriptive study conducted in King Fahad Hospital at Albaha in the period between Jan 2014 through Dec 2018.
We obtained data concerning the demographic and histopathological profile of 48 female patients with breast cancer during the study period.
48 patients ranging in age from 28-86 years (mean 52 years) were included in the study with the peak incidence age in the 5th decade. In 54.2% of cases, the tumor was left-sided. Infiltrating ductal carcinoma (IDC) was the most common type (37 cases; 77.1%) and mucinous is the least one (1 case; 2.1%). Approximately two-thirds of cases were grade 1 and 2 (33 cases; 68.8%). Six (12.5%) cases had tumor size ≤ 2 cm, 20 cases (41.7%) had tumor size of 2-5 cm, while 4 cases (8.3%) had tumor size more than 5 cm. In 31.2% of cases nodal metastases were negative, (31.2%) showed nodal metastases while in (37.5%) of cases lymph node metastases were not assessed.
Our study showed that the peak incidence age of breast cancer was the 5th decade of life while Infiltrating ductal carcinoma (IDC) was the most common histological type.
Breast cancer, Histopathology, Albaha, KSA
"Breast cancer is the most common cancer among women and one of the most important causes of death among them" [1]; therefore, it is critical that efforts in prevention and early diagnosis of breast cancer must be implemented everywhere [2]. Due to improved therapeutic and diagnostic tools and the evolution of breast cancer management in the developed countries, a marked reduction in the mortality rate of breast cancer is seen in these countries [3]. Population awareness about breast cancer, breast self-examination, and mammography screening are the other issues that may positively be influencing the incidence and mortality of the disease [4]. The incidence rate of breast cancer varies among different parts of the world, reflecting variation in race and ethnicity [5,6]. "Incidence varies from 27 per 100,000 in Middle Africa and East Asia to 92 per 100,000 in Northern America" [1]. "1.7 million new cases are predictable mostly in the developing countries by the year 2020" [4], and expected to reach 3.2 million by 2050 [7]. A review article conducted by Saggu, et al. in KSA reported that 1,152 cases are newly diagnosed in the year 2008, 1,308 in the year 2009, 1,473 female BC cases in the year 2010 [1]. The 2015 annual report of the Saudi National Cancer Registry shows that 1979 new cases of breast cancer were diagnosed which comprises 16.7% of all cancer reported among Saudi nationals, and 30.1% from all cancers reported among females of all ages [9]. Moreover, Alghamdi IG, et al. in his published work regarding the incidence of the disease in Saudi Arabia stated that the incidence of breast cancer in Albaha is approximately 2.0-6.8 per 100,000 women [10]. A study published by Elbasheer, et al. highlighting mortality of breast cancer stated that, "571000 deaths from BC reported by the WHO in the year 2015, while in 2018 the disease represented 24.2% of all cancers and 15% of deaths due to cancer among females" [11]. Data from clinical practice analyzing the epidemiology and histopathological profile of breast cancer is limited from our area. Therefore we aimed to study the profile of Saudi female patients with breast cancer attending King Fahad hospital at Albaha, KSA.
Many risk factors can predispose to breast cancer. The age of menopause over 50 years is associated with an increased risk of breast cancer [11-13]. The role of genetic factors in breast cancer arises from the fact that 40% of hereditary breast cancer cases occur due to mutations in the BRCA1 and BRCA2 genes inherited through the dominant autosomal pattern [14]. Moreover, "hormonal contraceptives, postmenopausal hormone therapy, obesity, alcohol consumption, smoking, diabetes, and radiation contribute to the incidence of breast cancer" [15].
This is a retrospective descriptive study conducted in King Fahad hospital at Albaha, department of Surgery. All breast cancer cases diagnosed from 2014 through 2019 were included. Data of all breast cancer during the study period were retrieved and then reviewed, from hospital records and histopathology reports. The study authors obtained ethical approval from the research ethical committee of faculty of medicine-Albaha University. Data collected include age, site of the affected breast, type of specimen, histopathological types, grades and lymph node, and margins status.
Statistical analysis Data managing was carried out using the Statistical package for social sciences (SPSS version [16]).
Of the 48 cases studied we found that 35.4% of the patients were aged (40-49 years), whilst 2.1% were of 20-29 years-old, as shown in Figure 1.
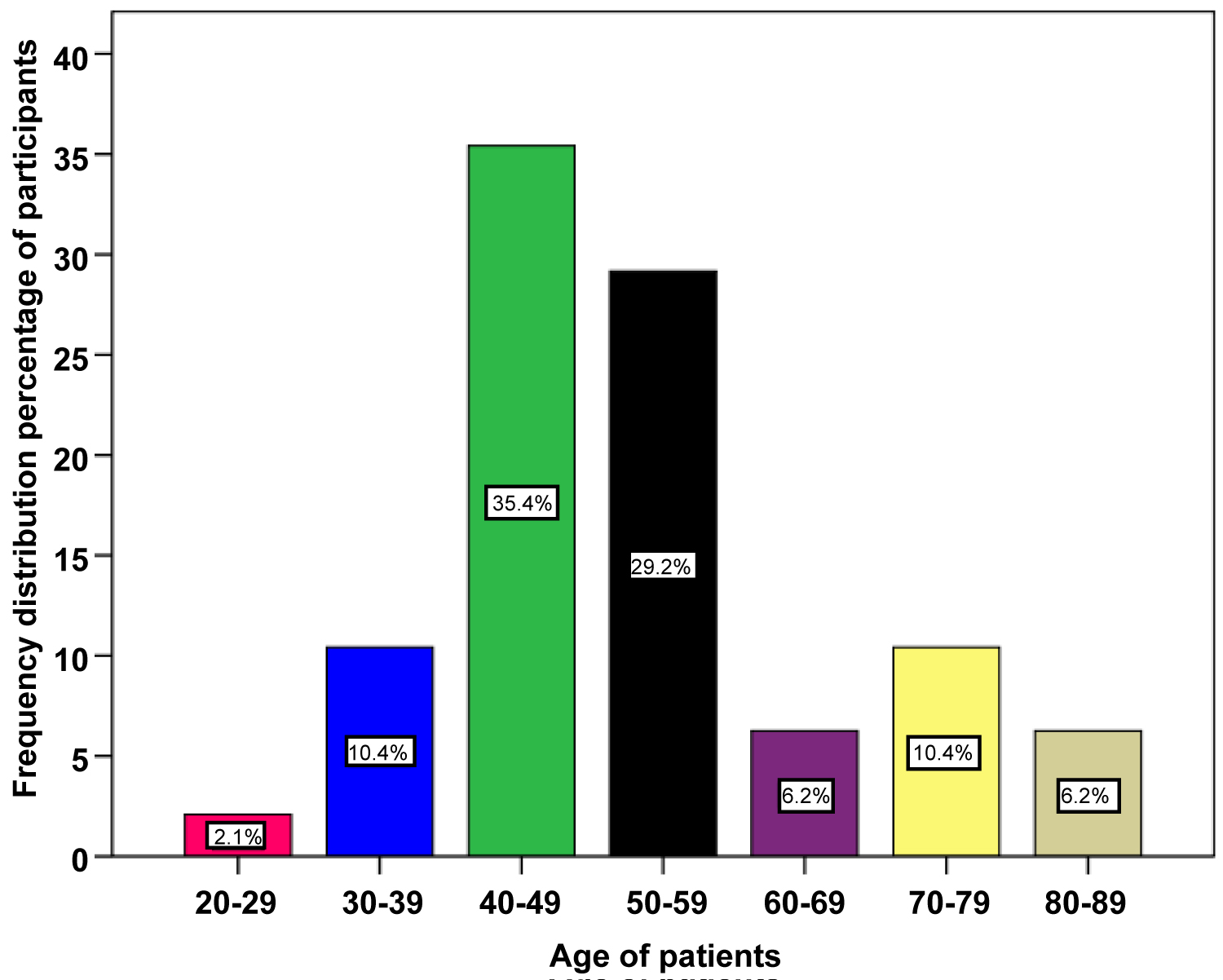 Figure 1: The Frequency distribution of ages of female patients with breast cancer.
View Figure 1
Figure 1: The Frequency distribution of ages of female patients with breast cancer.
View Figure 1
The left-sided tumor was 54.2% while the right one comprises (45.8%) of the cases. Based on the type of biopsy 17 cases (35.4%) were mastectomy specimens, 18 cases (37.5%) were tru-cut needle biopsy, while the rest types were wide local excision, quadrantectomy and lumpectomy specimens (Table 1).
Considering the histopathological types of breast cancer cases registered, Infiltrating ductal carcinoma (IDC) was the most common type (37 cases; 77.1%), followed by Invasive lobular carcinoma (ILC) (6 cases; 12.5%), while mucinous carcinoma was the least type (1 cases; 2.1%) (Table1).
Table 1: Demonstrates the frequency distribution percentage of the types of biopsy, histopathological types and tumor size among female patients with breast cancer (n = 48). View Table 1
Of the 48 cases studied and based on Nottingham modification of Bloom Richardson system, 9 cases (18.8%) were Grade I, 24 cases (50%) were Grade II, while 15 (31.2%) of cases showed Grade III (Figure 2).
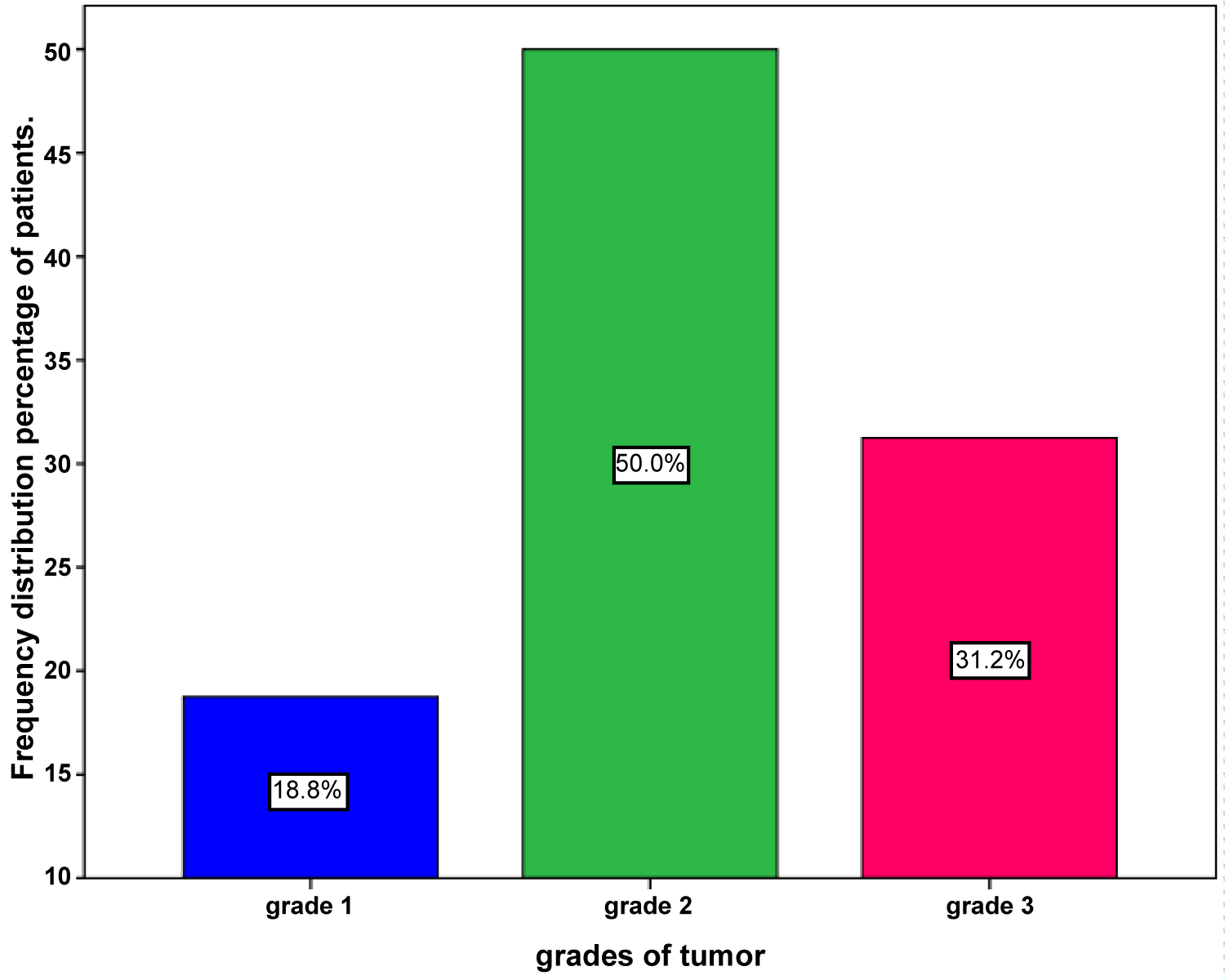 Figure 2: The distribution of different grades of female breast cancer.
View Figure 2
Figure 2: The distribution of different grades of female breast cancer.
View Figure 2
Six (12.5%) cases had tumor size ≤ 2 cm and were considered as (pT1), 20 cases (41.7%) had tumor size of 2-5 cm and were categorized as (pT2), while 4 cases (8.3%) had tumor size more than 5 cm and were classified as (pT3) (Table 1). Moreover, in all cases diagnosed based on tru-cut needle biopsy the tumor size was not assessed (18 cases; 37.5%).
When analyzing lymph node status, we found that 15 cases (31.2%) were negative for the malignancy (pN0), 15 cases (31.2%) showed nodal metastases while in 18 cases (37.5%) diagnosed on tru-cut needle biopsy, lymph node metastases were not assessed. Of the lymph nodes involved by tumor cells, 8 cases (16.7%) were classified as pN1 (metastases in 1 to 3 regional lymph nodes), 3 cases (6.2%) were categorized as pN2 (metastases in 4 to 9 regional lymph nodes), while 4 cases (8.3%) were described as pN3 (metastases in 10 or more regional lymph nodes) (Figure 3).
 Figure 3: The characteristics of lymph nodes status among female with breast cancer.
View Figure 3
Figure 3: The characteristics of lymph nodes status among female with breast cancer.
View Figure 3
In the present study, we investigated data of all female patients with breast cancer, attending King Fahad Hospital in Albaha area in the last 5 years concerning demographic and histopathological profile. Our study showed that peak incidence age of breast cancer was the 5th decade (40-49 years) and the majority of the cases occurred between the 5th and 6th decades (66.7%) with the mean age of 52.78 years. Our result is consistent with 68% by Takalkar, et al. in western India, moreover, Anwar, et al. in KSA stated that women having an ages between 30-59 years were associated with a higher rate of breast cancer incidence as compared to young women of ages less than 30-years-old [16,17]. This finding was also reported in Saudi Arabia by Alghamdi, et al. who ensured that the incidence of the disease increases with age with the peak incidence observed in the middle-age females [10]. Accordingly, the conduction of national screening programs for middle-age females is beneficial for early detection and intervention of breast cancer cases. Our analysis demonstrated that in 26 cases (54.2%) the tumor was on the left side, a finding that is also reported by Alotaibi, et al. in Saudi Arabia. Sughrue, et al. and Hartveit F, et al. as cited by Alotaibi, et al. explained this predominance by the fact that mothers prefer to use their right breast during breastfeeding [18]. Moreover, right-handed women check their left breast more often for lumps, increasing the chances of early treatment. In this study, we found that Infiltrating ductal carcinoma (IDC) was the most common type (37 cases; 77.1%), which is similar to the Saudi national registry report 2015 (79.2%) and Merdad, et al. study in Saudi Arabia (76%) [19]. However this was higher compared to (67.74%) in Nepal by Pradhan A, et al. [20]. Invasive lobular carcinoma (ILC) comprises (6 cases; 12.5%) and it was comparable to 11% by Merdad A, et al. [19]. Nevertheless, our result regarding medullary carcinoma (4 cases; 8.3%), and mucinous carcinoma (1 case; 2.1%) was incompatible with that of the annual report of the Saudi National Cancer Registry 2015 (0.1% for mucinous and 0.8% medullary type). This variation is probably attributed to the small size of our study samples. As published by Pradhan A, et al. Rakha EA reported that grade is an important determinant of breast cancer outcome and complimentary to lymph node (LN) stage [20]. On assessing the tumor grades we observed that the majority of the cases were Grade 2 and 3 (81.2%). This trend is approximately compatible to 76% by Merdad, et al. in Saudi Arabia [19]. Our study has also stratified the patient in whom lymph nodes status was assessed. We observed that in 31.2% of cases, the lymph nodes were negative for tumors while positivity was detected in a similar percentage. Our result was consistent with 30% without lymph node involvement in a report conducted by Al Diab, et al. in KSA and incompatible with 42% negative and 51% positive lymph node in Merdad A, et al. in KSA as well [19,21]. This discrepancy could be related to a considerable number of patients in our study whom diagnosed on tru cut needle biopsy, therefore, their lymph nodes status was not assessed. Tumor size is a crucial factor for the prognosis of breast cancer cases, moreover, it has been implicated in the Nottingham prognostic index and the TNM staging system [22]. Out of the 62.5% of cases in which their sizes assessed, we found that the majority (41.7%) had tumor sizes ranging between 2-5 cm (pT2), while only 8.1% of cases their sizes were more than 5 cm (pT3). This was in agreement with 56% by Al-Kuraya K, et al. in Saudi Arabia [23] and (54.84%) in Nepal by Pradhan A, et al. [20] and (51.9%) in Nigeria namely, by Adesunkanmi AR, et al. [24] and Oluogun WA, et al. who stated that, the majority of cases presented with their sizes ranging 2-5 cm (pT2) [25].
This study was done to analyze the histopathological profile of female breast cancer in Albaha at King Saudi Arabia. We concluded that the peak incidence of the disease was in the fifth decade of life, hence educational awareness should be lunched for this group of women. Infiltrating ductal carcinoma was the most common type of breast carcinoma. Most of the cases showed tumor size between 2-5 cm and exhibited Grade 11 of Nottingham modification of the Bloom Richardson system.