Introduction: Chilaiditi syndrome is a rare entity, with a worldwide incidence ranging from 0.025% to 0.28%, and it tends to affect males more frequently than females, with a ratio of 4:1. This paper explores and presents a rare medical case of Chilaiditi syndrome, emphasizing its rarity and complexity in diagnosis and treatment.
Case report: We present the case of a 52-year-old female patient who consulted a pulmonologist due to dyspnea and occasional abdominal discomfort. After diagnostic investigations, the incidental finding of Chilaiditi syndrome was identified on a chest X-ray, confirming the uncommon nature of this condition in clinical practice. The patient was subsequently referred to a surgical clinic for further evaluation and assessment of the need for surgical treatment.
Discussion: In the majority of cases, conservative treatment proves to be highly effective, successfully managing the condition in nearly all patients. Surgical intervention is typically reserved for cases where symptoms persist despite conservative treatment or when complications such as ischemia or perforation are suspected. Invasive surgical procedures, including colon resection, hepatopexy, colonopexy, right hemicolectomy, sigmoidectomy, and subtotal colectomy, have been performed successfully in managing this condition.
Chilaiditi syndrome, Dyspnea, Chest X-ray, Treatment
Chilaiditi's sign, a rare anomaly, is incidentally detected on chest or abdominal radiographs [1]. This sign was first described by the radiologist Demetrius Chilaiditi in 1910. It represents a radiological finding where a coiled segment of the colon or small intestine is situated between the liver and the diaphragm [2,3]. When this condition results in gastrointestinal symptoms, it is referred to as Chilaiditi syndrome [2].
Chilaiditi syndrome is a rare entity, with a worldwide incidence ranging from 0.025% to 0.28%, and it tends to affect males more frequently than females, with a ratio of 4:1 [1,2,4]. This condition is most commonly observed in the elderly population, where it has an incidence rate of approximately 1% [5].
The presence of the suspensory ligament and the colon's fixation normally prevent its interposition between the liver and the diaphragm [2,6]. Variations in this anatomical arrangement can lead to the pathological interposition of the colon, as observed in Chilaiditi syndrome [2]. Additionally, other factors that may predispose individuals to the development of Chilaiditi syndrome include congenital malposition of the intestine, colonic gaseous distension, a reduced liver size due to cirrhosis or hepatectomy, ascites resulting from increased intra-abdominal pressure, significant weight loss in obese patients, and chronic constipation caused by colonic elongation [2].
In patients with Chilaiditi syndrome, the most common symptoms are gastrointestinal in nature. However, it is worth noting that this condition can also lead to less common symptoms, such as dyspnea [7].
Awareness of this phenomenon and its inclusion as a potential differential diagnosis is crucial to avoid unnecessary laparoscopic interventions. Typically, the treatment of Chilaiditi syndrome is non-surgical and involves measures such as rest, fluid supplementation, nasogastric decompression, enemas, adopting a high-fiber diet, and the use of stool softeners [3,6].
Complications of Chilaiditi syndrome may involve perforation of the cecum, subdiaphragmatic appendicitis, and volvulus of the cecum, ileal flexure, or transverse colon [4].
We aim to present illustrative views of this rare medical condition. This clinical case serves as a reminder to healthcare professionals about the possibility of encountering this rare syndrome, which can sometimes present with symptoms and signs that may be misinterpreted.
A 52-year-old female patient sought consultation with a pulmonologist due to dyspnea, suspecting an exacerbation of her long-standing bronchial asthma. Alongside dyspnea, the patient also reported occasional abdominal pain, constipation, and abdominal distension. The patient's medical history included bronchial asthma, which had been under treatment for an extended period, and arterial hypertension. Upon examination, the patient was conscious, oriented, afebrile, and experiencing dyspnea. Notably, her abdomen appeared elevated to the chest level and was soft upon palpation, with slight tenderness noted in the right hypochondrium. Initially, a chest X-ray was requested by the pulmonologist to assess the primary pulmonary condition, and incidentally, this X-ray revealed the presence of an air collection beneath the right hemidiaphragm (Figure 1).
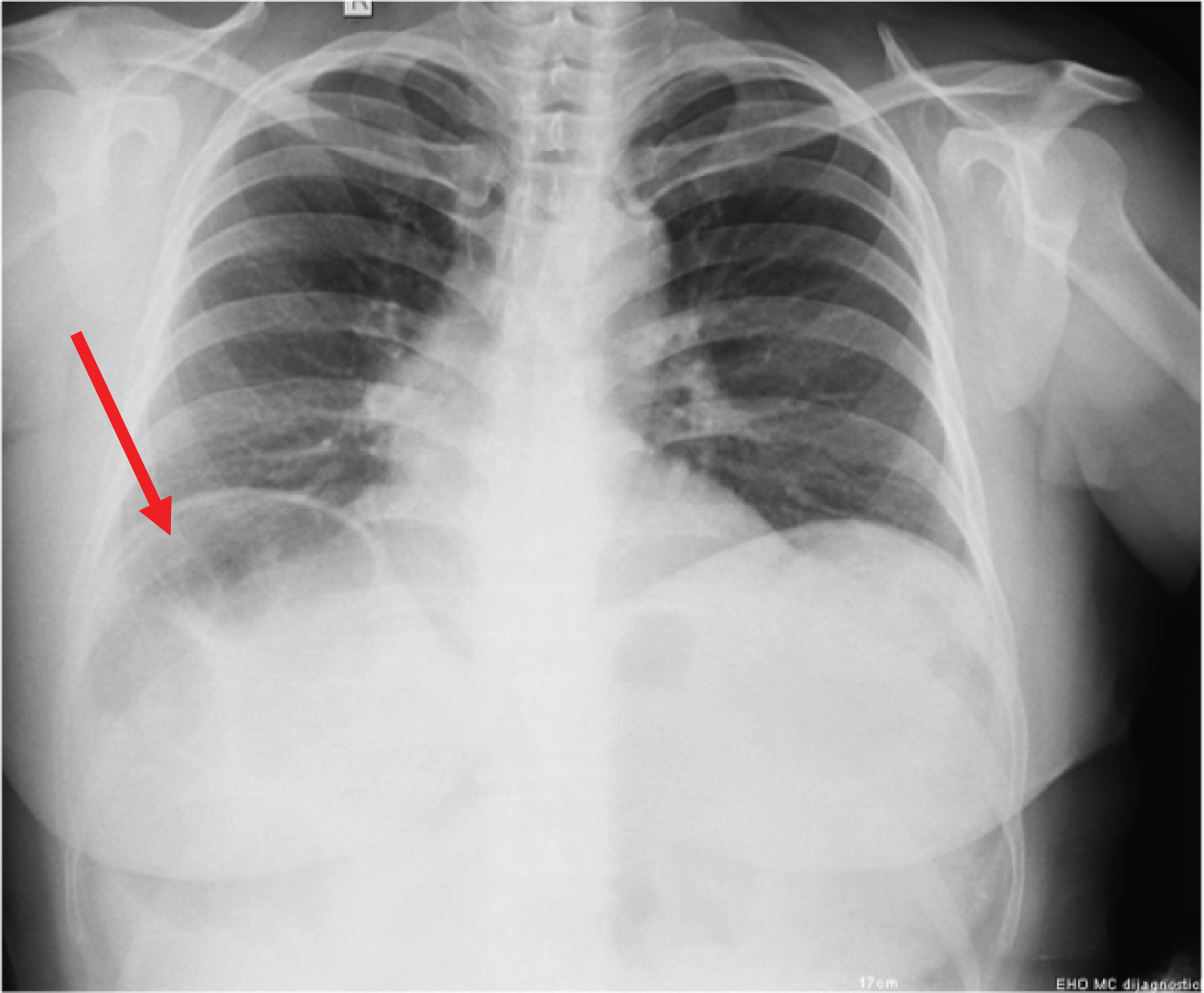 Figure 1: Chest X-ray demonstrates an air collection beneath the right hemidiaphragm.
View Figure 1
Figure 1: Chest X-ray demonstrates an air collection beneath the right hemidiaphragm.
View Figure 1
Following the confirmation of an air collection beneath the right hemidiaphragm, the patient was promptly referred to the surgical clinic. Standard laboratory results fell within normal reference ranges. The patient underwent conservative treatment, which included intravenous rehydration, administration of laxatives, and received guidance on maintaining a hygienic diet and getting adequate rest. Subsequently, the patient was discharged for continued home-based care. After undergoing this therapeutic regimen, the patient's overall health condition showed improvement.
Chilaiditi's sign, initially observed by Cantini in 1865 and later named after Demetrious Chilaiditi, who reported three cases of incidental radiological findings involving the interposition of the colon between the liver and the right hemidiaphragm in 1910 [1]. This sign is characterized as an incidental radiological finding, typically presenting as a crescent-shaped shadow below the diaphragm on the right side [8]. The estimated incidence of Chilaiditi's sign underscores its rarity, with reported rates ranging from 0.025% to 0.28% worldwide, and it tends to affect males more frequently than females, with a ratio of 4:1 [1].
In our presented case, the patient initially consulted a pulmonologist due to complaints of dyspnea and occasional abdominal pain. Notably, the patient had a well-documented history of long-term treatment for bronchial asthma. Initially, the dyspnea was attributed to a potential exacerbation of the pre-existing bronchial asthma. A standing lung X-ray was performed during the evaluation, and it was during this examination that Chilaiditi's sign was incidentally discovered as an unexpected finding. This discovery led to the patient being referred to a surgeon for further abdominal examination and management.
This clinical report pertains to a female patient, a circumstance that is considered quite rare. This rarity is reminiscent of a similar case reported by Ali, et al., who also described an elderly female patient in their study [5].
In addition to dyspnea, the patient reported experiencing abdominal pain and bloating, which aligns with the clinical manifestations described in the study by Basile, et al. [4]. The association of these clinical manifestations is consistent with the findings from the research conducted by Sofii, et al. [6].
The chest X-ray, which focused on the heart and lungs, did not reveal any significant abnormalities. However, it did show a distended bowel filled with gas in the visualized part of the abdomen, which corresponds to the findings obtained by Omran, et al. [1]. Additionally, on the same image, an elevation of the diaphragm was observed, which is consistent with the radiological finding reported by Karaman, et al. in their clinical presentation [3].
In this particular case, the patient received conservative treatment, including intravenous rehydration and the administration of laxatives. Additionally, guidance was provided on maintaining a hygienic diet and getting adequate rest. This treatment approach mirrors the method employed by Sofia, et al. in their treatment of patients with the same syndrome [6].
In the majority of cases, conservative treatment proves to be highly effective, successfully managing the condition in nearly all patients [6]. Surgical intervention is typically reserved for cases where symptoms persist despite conservative treatment or when complications such as ischemia or perforation are suspected [6]. Invasive surgical procedures, including colon resection, hepatopexy, colonopexy, right hemicolectomy, sigmoidectomy, and subtotal colectomy, have been performed successfully in managing this condition [8].
As Chilaiditi syndrome is an exceptionally rare condition, one of the limitations of this study is its reliance on a single patient's experience. Additionally, because CT is considered the diagnostic method of choice for Chilaiditi's sign, the fact that the patient declined to undergo a CT scan represents a limitation in this presentation. Obtaining imaging data through CT could have provided more comprehensive insights into the condition and further supported the diagnosis.
In summary, Chilaiditi syndrome's rarity underscores the importance of timely recognition, interdisciplinary collaboration, and ongoing research to enhance our understanding of this intriguing medical condition and improve patient care.
This paper explores and presents a case of Chilaiditi syndrome, a rare medical condition that requires careful diagnosis and treatment. Through this case study, we emphasize the importance of rapid recognition and timely management of this uncommon occurrence, as well as the need for further research to expand our understanding of this condition and enhance patient care.
As Chilaiditi syndrome is an exceptionally rare condition, one of the limitations of this study is its reliance on a single patient's experience.
No funding was received.
Not applicable.
Consent to publish obtained.
The authors declare that they have no competing interests.