Computed Tomography (CT) scans promote a higher dose deposition than conventional radiology exams. These tests contribute significantly to the increase in the patient and collective dose, being a public health concern worldwide. There is a great need to improve protocols to seek lower doses while maintaining the diagnostic image quality. The development of phantoms allows the testing of different acquisition protocols. For this, the phantoms must present an absorption characteristic of the X-ray beam similar to the represented patient. In this study were tested two cylindrical head phantoms of polymethylmethacrylate (PMMA). One CT head phantom is the head standard test with 16 cm in diameter and the other head phantom developed is smaller at 12 cm in diameter. Both phantoms are 15 cm long. Different acquisition protocols were performed on a GE CT scanner, LightSpeed VCT model with 64 channels. The central slice of the phantoms was irradiated successively, and using a pencil ionization chamber, to obtain the CT air kerma indexes in PMMA (Ck,PMMA,100) and CT dose indexes (CTDI). From these results, the CT Dose Index values weighted and volumetric (CTDIw, CTDIvol) were obtained for 10 cm scans of the central region of the head phantoms, in helical mode. The scans were performed using different voltage values (80, 100 and 120 kV) and charge (mA.s). Absorbed dose values (CTDIvol) using routine protocols for head scans ranged from 39.22 to 49.67 mGy. Proposed optimized protocols varied from 20.89 to 31.93 mGy and reduced the absorbed dose by up to 57.94% in the smallest phantom, with 12 cm in diameter.
Computed tomography, Phantom, Dosimetry
Computed Tomography (CT) is one of the most used exams for radiologic diagnostic in medicine. It is a very fast test that can produce high quality images. However, the increasing demand for CT had a considerable impact on doses provided to patients and on the exposure of the population as whole, being a public health concern worldwide [1,2]. According to UNSCEAR report the use of CT contributed with 62% of the collective dose from diagnostic radiological tests [3]. Many factors collaborated to the increased demand for CT scans, including the constant technological evolution of the equipment associated to greater availability and a relative tendency to decrease exam costs [4,5].
Patients undergoing CT scans can range from neonates to oversized adults. However, radiation doses in CT are generally measured in cylindrical PMMA phantoms, that represent a standard adult patient. These phantoms are designed to simulate a head, 16 cm in diameter, and a body, 32 cm [6,7].
It is difficult to obtain reliable quantitative values of patient doses from any measurements performed in these standard phantoms, because patients have sizes and body compositions that can differ markedly from the phantoms, such as pediatric and obese patients. The development of phantoms allows testing different acquisition protocols [8,9]. For this, the phantoms must have an X-ray beam absorption characteristic similar to the represented patient.
The increasing demand for CT scans in pediatric patients is mainly due to the high rates of traumatic injuries from car accidents, falls on bicycles, blunt trauma, traumatic brain injury, as well as a significant increase in the incidence of childhood neoplasms, being the CT images used in the diagnostic process. Therefore, acquisition protocols should be used that determine the reduction of the radiation dose without compromising the diagnostic quality [10,11].
The risks of stochastic effects increase in children due to the tissue radiosensitivity allied to the long-life expectancy. The dose deposited in a pediatric patient is directly related to the energy that was retained during the process of exposure to ionizing radiation [12,13].
In this study, two CT head phantoms were used, the standard head phantom and another with smaller volume to observe the dose distribution and to obtain the dose index (CTDI). Also, different acquisition protocols were tested using different values of X-ray tube supply voltage (80, 100 and 120 kV) and load (mA.s).
The experiment was conducted using a GE CT scanner, LightSpeed VCT model with 64 channels. For the development of this work, experimental measures have been obtained using two head phantoms, both made in polymethyl-methacrylate (PMMA). These phantoms were constructed by the research team of the Center for Research in Biomedical Engineering (CENEB) of the Federal Center for Technological Education of Minas Gerais (CEFET-MG), being a representative of a standard adult and a pediatric patient's head. The standard adult head phantom is cylinder with 16 cm in diameter and 15 cm in length. This phantom is considered the default for the dose reference in head CT scans. The pediatric head phantom is cylinder and has a dimension of 12 cm in diameter and 15 cm in length, representing a smaller head, like a pediatric patient.
This cylindrical phantom has five openings for positioning the dosimeters, one central and four at the peripheral openings, which are displaced from each other by 90°. The openings are 1.27 cm in diameter and 15 cm in length. The center of the peripheral openings is 1 cm from the edge of the phantom. The Figure 1 shows an illustration with the measurements of the adult and pediatric phantoms made with PMMA.
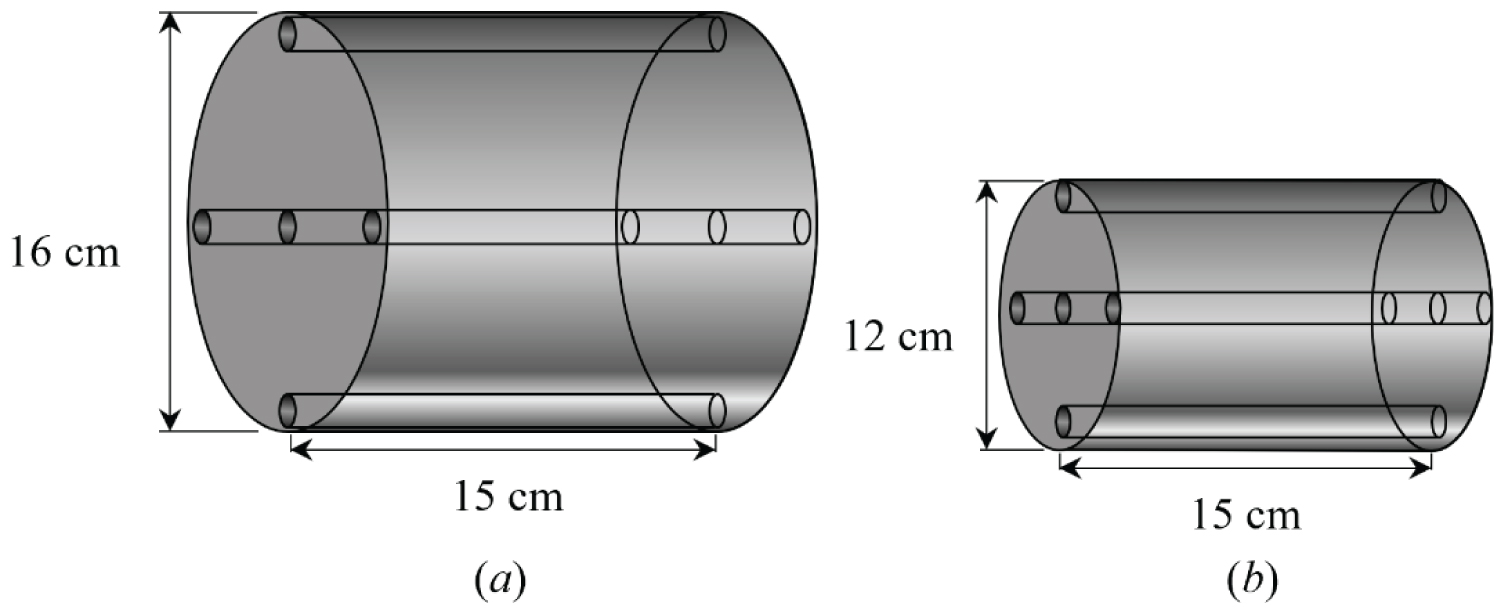 Figure 1: Head phantoms dimensions: (a) Adult standard and (b) Pediatric.
View Figure 1
Figure 1: Head phantoms dimensions: (a) Adult standard and (b) Pediatric.
View Figure 1
The standard adult head phantom is considered for dose reference in head CT scans. Therefore, all head CT scans performed on a given equipment are accompanied by a report that informs an estimated value of patient absorbed dose (CTDI) based on the scan of this phantom. The Figure 2 shows the image of these phantoms placed in the isocenter of the gantry of the CT scanner.
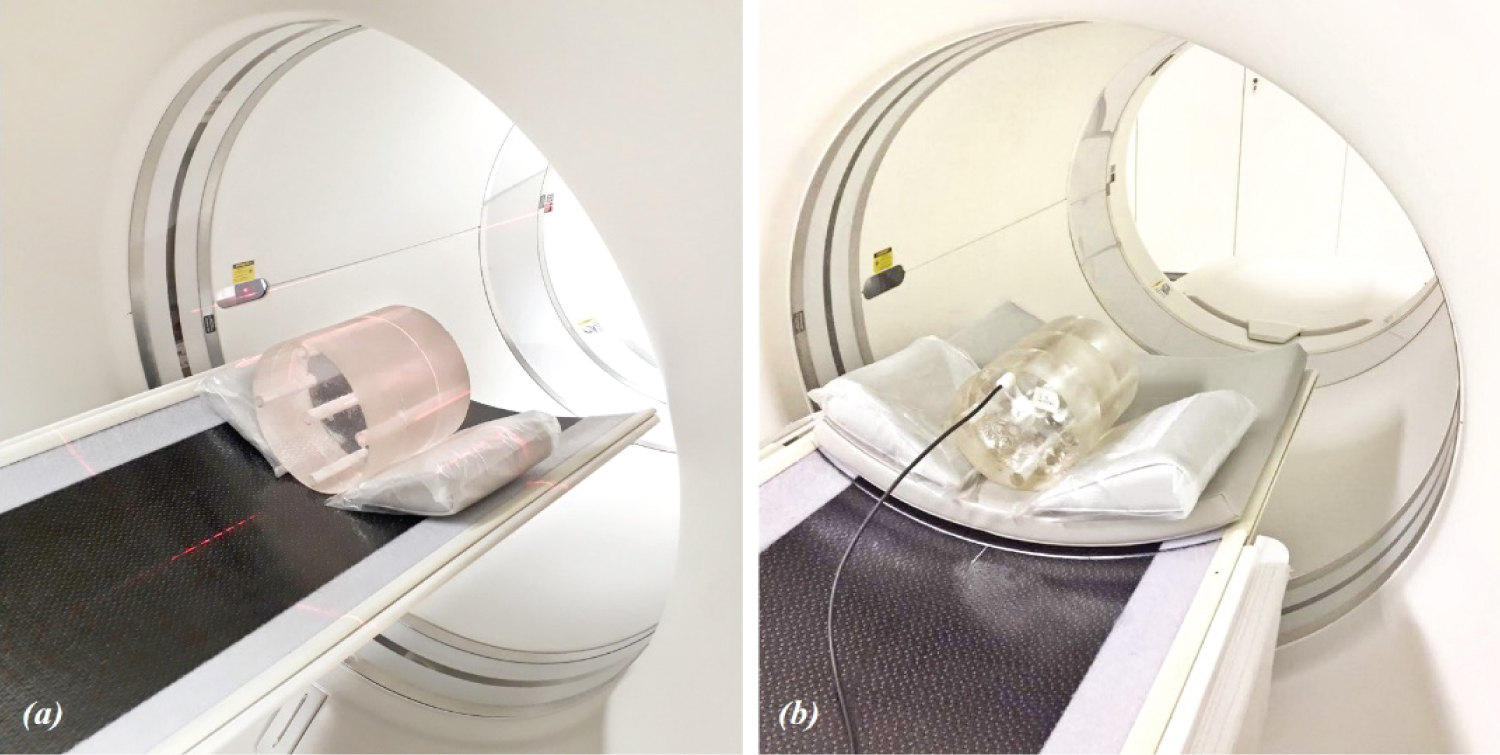 Figure 2: PMMA head phantom images: (a) Adult standard and (b) Pediatric.
View Figure 2
Figure 2: PMMA head phantom images: (a) Adult standard and (b) Pediatric.
View Figure 2
Dose measurements have been performed by positioning the head phantom in the isocenter of the gantry and aligning the openings like as the positions 3, 6, 9 and 12 of an analog clock, through the help of the CT scanner lasers. The phantom openings are filled with PMMA rods which must be removed one by one for the positioning of the pencil chamber, targeting the dose measurements in the five regions.
A pencil ionization chamber RADCAL ACCU-GOLD model 10X6-3CT was used to measure a CT air kerma in PMMA (Ck, PMMA,100) in each opening of both phantoms. First, a scout was made in order to check the correct alignment of the phantoms as well as to demarcate the central slice position. Furthermore, the central slice of the phantoms was irradiated successively. For each chamber positioning, five measurements were performed, getting a minimum of 25 measurements for each protocol and for each phantom. In the central slice irradiations, the remaining openings were filled using PMMA rods. From these results, the CT Dose Index values, weighted and volumetric (CTDIw, CTDIvol), were obtained for 10 cm scans of the central region of the head phantoms, in helical mode. The CTDIw and CTDIvol were calculated according to the Eq. 1 and 2 [13,14]:
where, CTDI100, central is the dose index value found at the central position and CTDI100, per is the average dose index value at the peripheral positions of the head phantom. The scans were performed using different voltage values (80, 100 and 120 kV) and charge (mA.s). In order to obtain the CT Dose Index (CTDI) values from the air kerma values the measurements were adjusted using a conversion factor (Fc) air/PMMA. The Fc used are 1.0418, 1.0324, and 1.0106 for the X-ray beam generated with 120, 100 and 80 kV, respectively [14-16].
The protocol for irradiation the phantom central slice, in axial mode, used the following parameters: Current of 100 mA, charge of 100 mA.s, tube rotation time of 1s, beam thickness of 10 mm and three voltage values (120, 100 and 80 kV).
Helical scans of 10 cm in length were also performed in the central region of the head phantoms, aiming to define a current value adjusted by the equipment's automatic exposure control (auto mA), using the different voltage values. Usually, in the initial slices of the scan there is an adjustment in the current value (mA) in the first slices irradiated and after these adjustments the current stabilizes, since all the slices of the phantom have the same size.
With the current reference value defined based on the current recorded in the central slice, new scans were made to test fixed current values, lower than the value suggested by the automatic current control scan. For each current value tested, noise was calculated in the image of the central slice and the best current value was determined for each phantom and voltage.
The protocols used in the scans of the central region of the phantom used pitch values closest to 1, that is available in the CT equipment. Table 1 shows the CT head scanning protocol used in the service routine, regardless of the patient's size or age.
Table 1: Routine protocol of CT head scan. View Table 1
In order to validate the quality of the CT images, a noise analysis of the central slice image was performed in each helical CT scan, aiming at maintaining the diagnostic quality of the images. The noise value had its maximum acceptable limit of 1%, considering that the phantom is homogeneous [15-17]. This noise limitation, using a homogeneous material, implies in the generation of diagnostic images of the human body. Then, as a control parameter for testing new protocols, it was defined that the noise threshold in the central slice image should be 1% to guarantee the diagnostic quality of the patient's image.
Four regions of interest (ROI) were selected in the image and were analyzed. The noise (N) was calculated as the percentage value of the standard deviation in relation to the average value of the Hounsfield scale (HU) through Equation 3.
Table 2 shows the average values and standard deviation of punctual and weighted air kerma in PMMA (Ck,100,PMMA and Cw) and absorbed dose (CTDIw) that were obtained from Ck,100,PMMA measured in the five positions of the phantoms, using the parameters defined for the central slice (10 mm) irradiation with the charge fixed in 100 mA.s.
Table 2: Values of Ck,100, PMMA, Cw and CTDIw in mGy standard deviation for head phantoms. View Table 2
The protocol using the voltage of 120 kV has the highest absorbed dose value recorded in position 12 of 21.39 mGy in the adult phantom and 25.26 mGy on the pediatric phantom. The minimum value happened in the position 6 for both phantoms with the 80 kV voltage, with the value of 5.84 mGy in adult and 7.72 in pediatric phantom. The proximity between the doses at points 3 and 9 indicates the good positioning of the object in the gantry isocenter.
Analyzing the measurements obtained, the pediatric phantom has dose values always higher, since the other parameters of central slice irradiation is the same. The cut area of the pediatric phantom is smaller than the adult, promoting a higher dose deposition. Also, with the voltage of 80 kV the values are always the lowest since the other parameters used were the same. Since average energy of the beam of 80 kV is lower, promoted smaller doses deposition. Although, the 120 kV voltage generates the highest dose depositions.
Table 3 shows the results of absorbed doses (CTDIvol) and standard deviation obtained when it was used the routine and optimized protocols in both phantoms with the use different voltage values and optimized charge in the X-ray tube during the scans of the central region of the phantoms. In optimized protocols, the optimized charge value (mA.s) was adjusted to the point where the noise in the central slice was less than 1%. The other parameters: Pitch, tube rotation time, beam thickness and image reconstruction were the same of the routine protocol (Table 1).
Table 3: Routine and optimized protocols. View Table 3
In the tests for new protocols, it was decided to use same pitch of 0.984 of the routine protocol, which is the closest possibility to the value 1 available in this CT machine.
The absorbed doses of the new protocols tested in the adult standard head phantom varied from 28.87 to 31.93 mGy, with the lowest dose occurring with the Opt. 3 protocol that use a voltage of 80 kV and 420 mA.s. The noise value verified in the central image of this scan was 0.978%, which is the established criterion for maintaining the diagnostic quality of the image. The Opt. 3 protocol promoted a dose reduction in the patient of 27.68%, with the absorbed dose going from 39.92 to 28.87 mGy.
In the pediatric phantom with 12 cm, the lowest absorbed dose was 20.89 mGy for the Opt. 6 protocol of 80 kV, 240 mA.s. The noise value verified in the central image of this scan was 0.929%, which is the established criterion for maintaining the diagnostic quality of the image. The Opt. 6 protocol promoted a dose reduction in the pediatric phantom of 57.94%, with the absorbed dose going from 49.67 to 20.89 mGy. Also, the absorbed dose in the routine of the pediatric phantom had a dose of 19.63% higher than the adult phantom. The Figure 3 shows a graphic with the absorbed dose values (CTDIvol) for the adult and pediatric phantom considering the different protocols defined in Table 3.
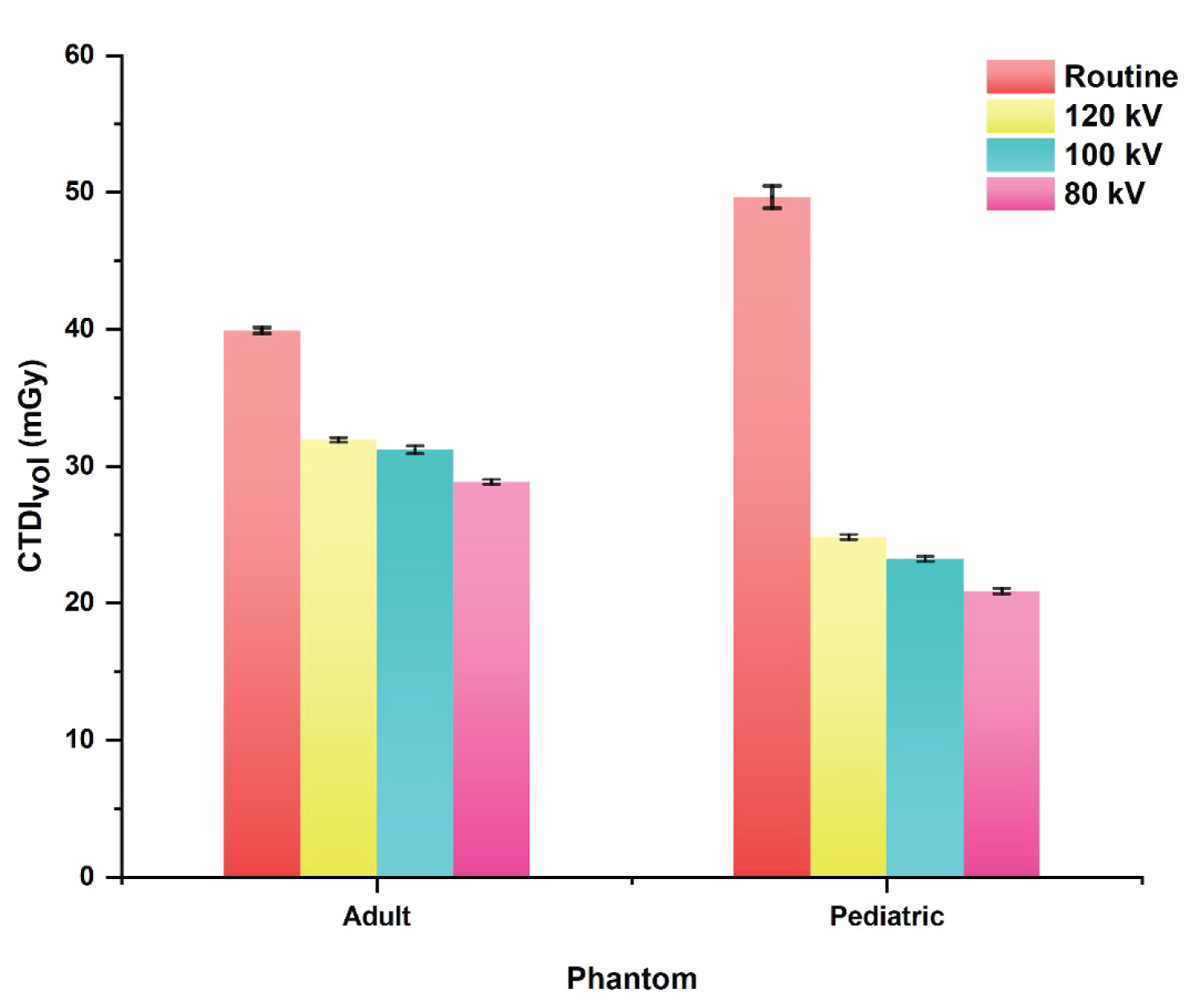 Figure 3: CTDIvol values for adults and pediatric head phantoms obtained with routine and optimized protocols.
View Figure 3
Figure 3: CTDIvol values for adults and pediatric head phantoms obtained with routine and optimized protocols.
View Figure 3
Observing the absorbed dose values obtained for the tested protocols, it is verified that the adult and pediatric phantom had a better CT scan with the voltage of 80 kV. The optimized protocols selected with the low absorbed dose obtained noise values below 1%, being a good alternative to be used aiming the reducing of absorbed dose of the patient and maintaining the diagnostic quality of the image.
It is also worth noting that the tested protocols showed in Table 3 were selected among several others tested with the variation of the mA.s value until a noise low than 1% was obtained in the analysis of the image of the central slice. The mA.s and pitch variation cannot be chosen randomly, since there are discrete values in the CT equipment menu that are possible to be tested.
Patients undergoing CT scans can range from newborns to large adults. However, CT radiation doses are usually measured on PMMA phantoms representing a standard adult patient. It is difficult to obtain reliable quantitative values of patient doses from any measurements performed on this standard head phantom because patients have body sizes and compositions that may differ from the standard phantom, as is the case for pediatric patients, small women, and patients bigger and obese. Therefore, the development of the phantoms used in this work allows representing different sizes of patients and testing different acquisition protocols for head scans.
This work highlights relevant information on dose reduction in adult and pediatric head CT scans, being of great importance to argue for the adoption of optimized protocols without losing the diagnostic image quality.
This study was financed in part by the Coordenacão de Aperfeicoamento de Pessoal de Nível Superior - Brasil (CAPES) - Finance Code 001. Also, this work was supported by the FAPEMIG.