Background: In sub-Saharan Africa, several neurosurgical diseases are rare in neurosurgical practice, in contrast to other climes. Poor diagnostic and health facilities are always blamed. More than six decades after the birth of neurosurgery in the region, those deficiencies and workforce have markedly improved in neurosciences. The aim of this study was to identify the uncommon cranial neurosurgical lesions and their frequency in the study centre.
Method: Search for rare pathologies was made of prospectively recorded database of 34,670 patients managed at the centre that served a large population of about 47 million black Africans of mostly Igbo ethnicity.
Results: The identified rare diseases included cavernoma (4), Moyamoya disease (0), epidermoid cysts (0), Rathke's cyst (1), chordomas (0), colloid cysts (1), pineal region tumours (4), Trigeminal Neuralgia (4), and vestibular schwannoma (5). There is no available explanation for these findings hence the importance of reporting our experience so that other researchers could make contributions. There are no previous reports on this subject from sub-Saharan Africa.
Conclusion: The rarity of certain neurosurgical pathologies in the study region is a research challenge. Identification of the cause(s) could be a major scientific breakthrough in epidemiology and prevention of diseases, but this would require international collaboration.
Rare diseases, Geographical neurosurgery, Trigeminal neuralgia, Vestibular schwannoma
There are several options for the sorting of diseases, but the one generally used in the classification is into common and rare types. When a disease has a prevalence of less than 5 per 10, 000, it is classified as rare. It is estimated that there are 5000-8000 rare diseases and many of them involve the nervous systemic [1].
It is now recognized that there are geographical variations in the incidence of many diseases[2]. In sub-Saharan Africa, several neurosurgical diseases are rare in neurosurgical practices in contrast to other climes. Diseases like trigeminal neuralgia and vestibular schwannoma dominate neurosurgical conferences, webinars, and neurosurgical literature. The experience in sub-Saharan Africa is different because there are very few mentions of these problems except for occasional case reports. Poor diagnostic facilities and scanty neurosurgical workforce are likely to be blamed for the failure to make the diagnosis. More than six decades after the birth of neurosurgery in the sub-region, those deficiencies have markedly improved in neurosciences. Time is therefore apt to determine if some diseases that neurosurgeons manage routinely globally are uncommon in our sub-region.
The aim of this study was to identify rare cranial neurosurgical pathologies in a tertiary hospital in sub-Saharan Africa that has the diagnostic facilities and appropriate workforce. To the best of the authors' knowledge, no study from sub-Saharan Africa has addressed this subject.
This is a retrospective analysis of prospectively recorded database of patients managed between January 2003 and 31st December 2021 at the study institution. Information was obtained from clinical records, CT, MRI, operating theatre, and pathology database of the hospital.
The hospital had consultant Neurosurgeons, Radiologists, Neurologists and Senior Neurosurgical Residents, throughout the period of the study. Although located at a city with a population of about 723,000 (2006 National Census), the hospital also serves as a referral centre for many States and provides cerebral angiography(CA), CTA and MRA services. The catchment population of mixed socio-economic status is over 47 million (Table 1). No autopsy search for pathologies was performed. The study was not concerned with management or outcome. Because this was a hospital-based study, diseases were classified as rare if the total number diagnosed during the 19-year period was ≤ 5. Ethical approval was obtained from the hospital for the study.
The rare neurosurgical pathologies discovered were in areas of neurovascular, oncology, and skull base. During the period of the study a fair volume of neurosurgical cases were managed at the hospital (Tables1 & Table 2). Trauma, tumours, spine pathologies and pediatric neurosurgery accounted for most of the cases. Further analysis of the mix of cases revealed that some diseases that are known to be common in other countries and races are rare. (Table 3). No cases of Moyamoya disease (MMD), chordoma, and epidermoid cyst, were encountered. Other pathologies that were uncommon included Cavernoma (4) [Figure 1], vestibular schwannoma (VS) (5) [Figure 2], Trigeminal Neuralgia (TN) (4), pineal region tumours (4) [Figure 3], colloid cyst of the 3rd ventricle (1), and Rathke's cyst (1). The characteristics of the rare tumours are shown in Table 3.
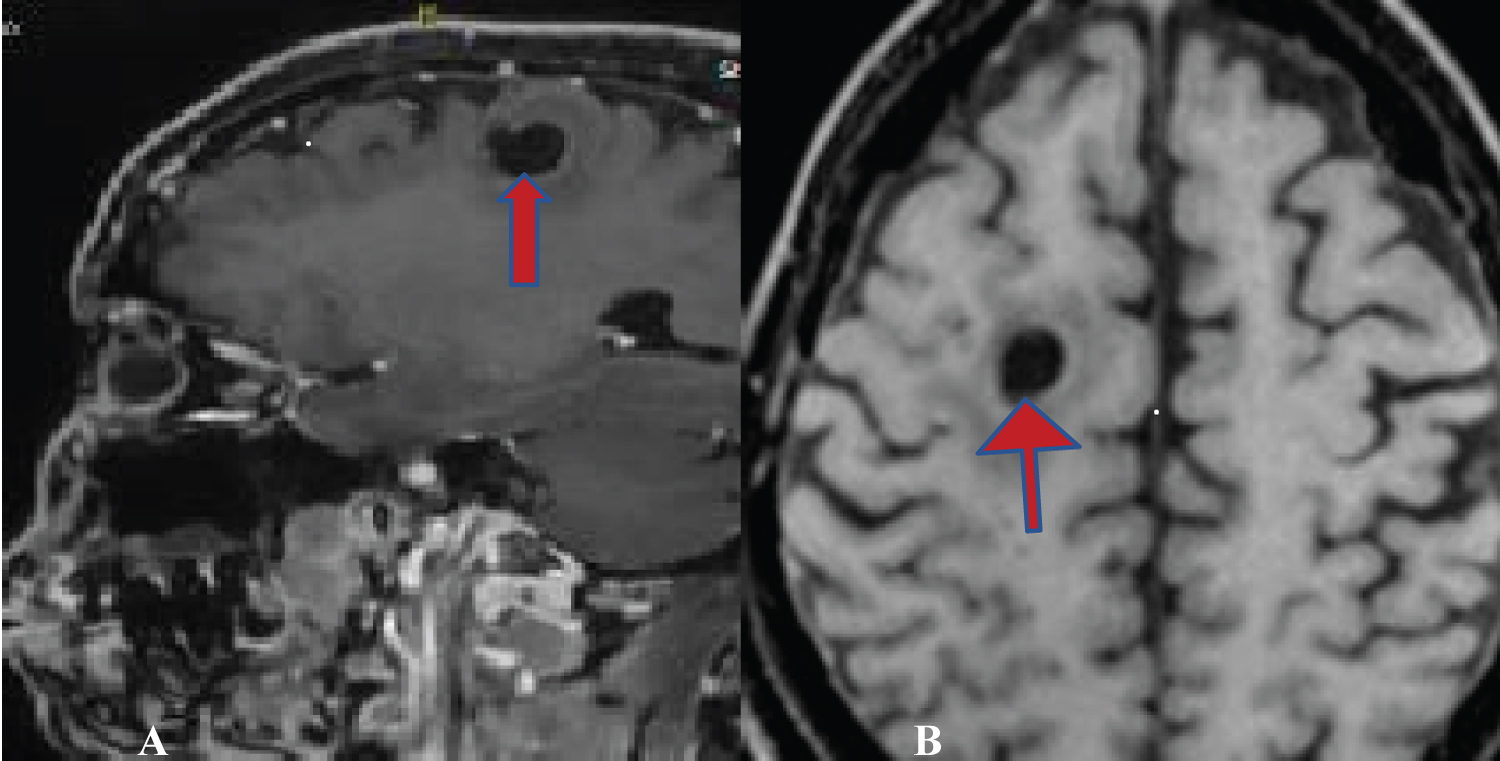 Figure 1: MRI images of Cavernoma (RED Arrows). A) Saggital TW1+ Contrast. B) Axial TW1. View Figure 1
Figure 1: MRI images of Cavernoma (RED Arrows). A) Saggital TW1+ Contrast. B) Axial TW1. View Figure 1
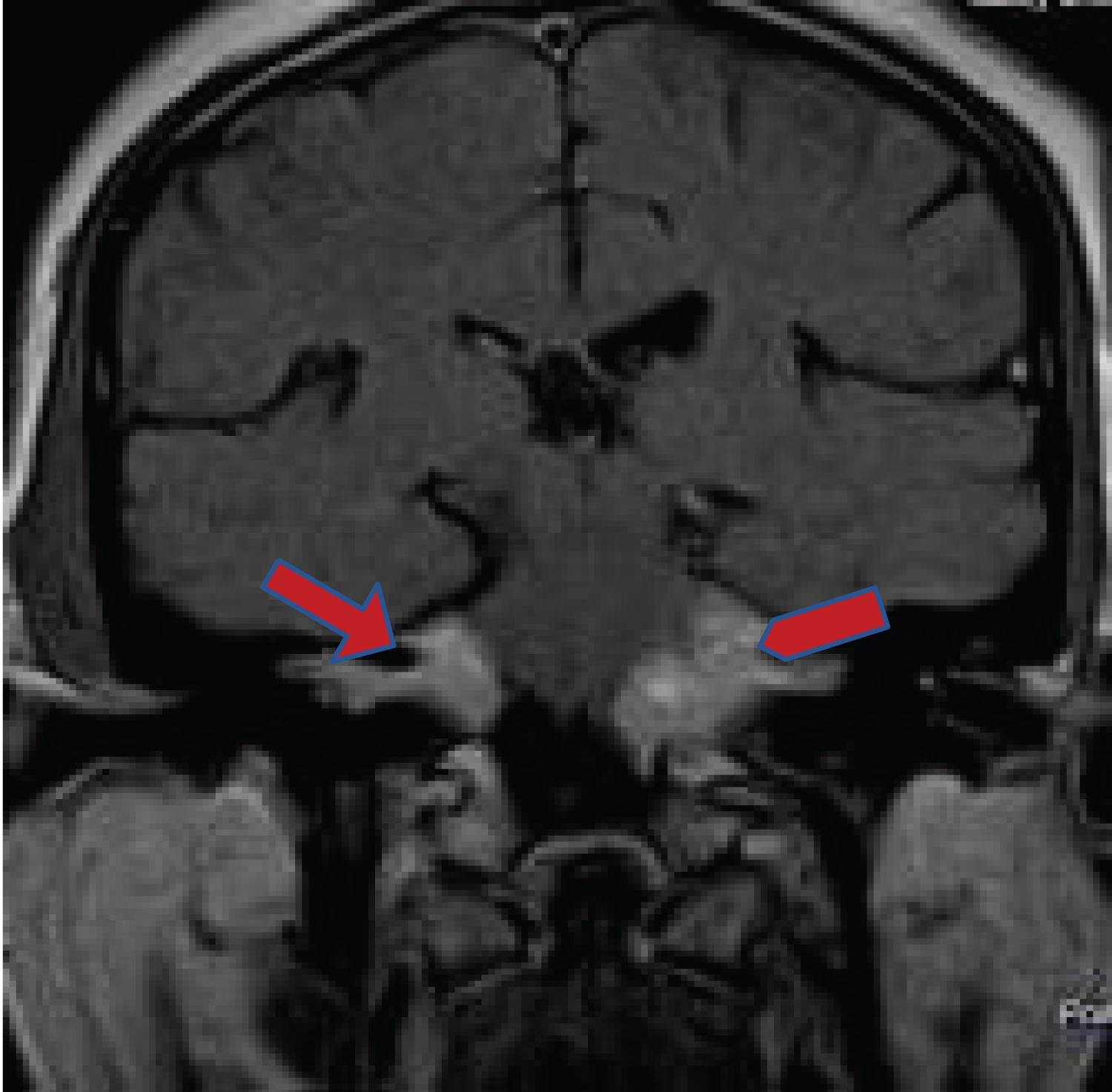 Figure 2: MRI Coronal TW1 Contrast showing enhancing C-P Angle tumours (red arrows) Bilateral Vestibular Schwannoma [NF2]. View Figure 2
Figure 2: MRI Coronal TW1 Contrast showing enhancing C-P Angle tumours (red arrows) Bilateral Vestibular Schwannoma [NF2]. View Figure 2
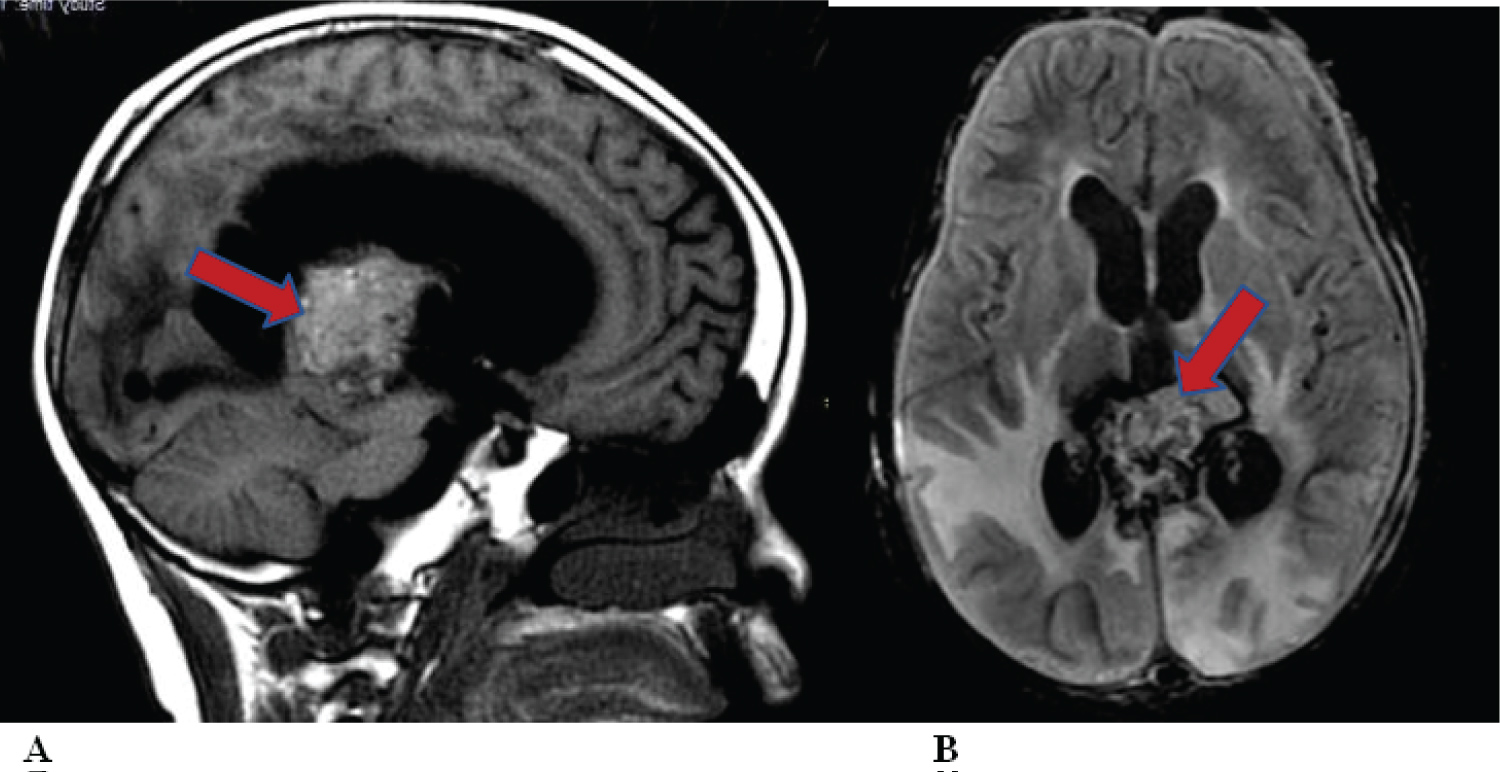 Figure 3: MRI BRAIN Showing Pineal region tumours (red arrows) causing hydrocephalus. A) Sagitta T1 Flair; B) Axial T2 FLAIR. View Figure 3
Figure 3: MRI BRAIN Showing Pineal region tumours (red arrows) causing hydrocephalus. A) Sagitta T1 Flair; B) Axial T2 FLAIR. View Figure 3
Table 1: Hospital clinical data 2003-2021. View Table 1
Table 2: Comparative list of select lesions (2003-2021). View Table 2
Table 3: Characteristics of the rare Lesions. View Table 3
The data presented here strongly suggest that some diseases appear to be rare in the study centre. The question then is what could be responsible for this? Poor facilities could not be blamed because the hospital has adequate diagnostic and management armamentarium that are of international standard. These include CT(16-slice and 64-slice), MRI (0.35T and 1.5T), as well as experienced specialists in radiology, pathology, neurology, and neurosurgery.
Cavernomas (Figure 1) are vascular abnormalities that primarily occur in adulthood and may present as cerebral haemorrhage, stroke, and seizures. They are preponderant in Mexican Americans and Hispanics. The true prevalence is unknown, but two MRI based prospective studies in different regions of USA reported prevalence rate of 0.44%- 0.46% [2-4]. It is therefore unclear why only four cases have been seen in our centre unlike other neurovascular diseases like AVM and aneurysms.
Moyamoya disease (MMD) which has not yet been reported from our sub-region is characterized by progressive stenosis or occlusion of the intracranial portion of the internal carotid artery and their proximal branches, resulting in ischemic or hemorrhagic stroke causing severe morbidity and even death. The prevalence of MMD in Japan is 3.16 cases per 100,000 people, while the incidence is 0.35, hence Japan is regarded as having the highest prevalence rate globally. Other Asian countries like China also have high prevalence rates [5,6]. Studies have shown a possible genetic association of MMD linked to chromosome 17 [6]. Interestingly, no case of MMD has been diagnosed in the study centre.
Global experience reports Vestibular Schwannoma (VS) as a common benign tumour of the vestibulocochlear nerve. It may be sporadic and unilateral but bilateral in neurofibromatosis Type II (NF-2) which is an inheritable disorder. A low frequency of VS was reported previously from the study centre, which accounted for 0.5% of intracranial tumours managed in the hospital [7,8]. Since the report that captured all three VS cases up till 2015, only two new cases have been added between (2016-2021), thereby supporting the rarity of this tumour in our region (Figure 2). Two of the five cases of VS were bilateral (NF-2). This is far less than 8% -9.9% of intracranial tumours reported from other countries [9]. The incidence of VS is currently about 3- 5 per 100,000 population for the sporadic variety [10].
Pineal Tumours (Figure 3) account for up to 1% of intracranial tumours in adults and 3-8% in children [11]. A single hospital in China reported 132 cases in 9.4 years [12]. In a prevalence MRI study 288 cases were discovered from about 14,500 MRI scans [13]. Only four cases (Males = 3, Females = 1) were diagnosed in our facility and constituted 0.4% of all intracranial tumours.
Review of skull base tumours at the study centre during the same period revealed no cases of epidermoid tumours or chordomas. Only one Rathke's cyst, and one radiologically diagnosed case of colloid cyst of the third ventricle were recorded. Although these tumours are rare in other parts of the world, published studies reported about 10 to 32 cases over about ten-year period for each of the pathologies, unlike the zero in the index study [14-17].
Trigeminal neuralgia is probably the most painful disease, typified by sudden, excruciating, short, and stabbing recurrent episodes of facial pain affecting one or more branches of the trigeminal nerve. Pain usually strikes unexpectedly but can be sparked by talking, eating, washing the face, brushing teeth, shaving, a light touch or even a cool breeze. Neurovascular compression at the trigeminal root entry zone is a causative anatomic abnormality that usually requires vascular decompression.
The frequency of TN is high in many parts of the world; hence it is a prominent topic in neurosurgery literature, and conferences. Frequency in the United States is 2.5 (males) and 5.7 (females) per 100,000 per year [18]. The incidence of TN was 100.21 per 100,000 person-years in Korea and is more common in females and the age group of 51-59 years had the highest prevalence of TN [19]. In contrast to the above frequency data, our study centre has managed only four cases of TN and three were females. Another bigger hospital in a different part of the country reported only 14 cases of TN thereby collaborating the rarity of this disease [20].
A possible reason for low frequency of some pathologies could be ignorance, leading patients to choose unconventional therapies like traditional and religious healers. The limited coverage of health insurance results in unaffordable out- of-pocket payment for healthcare. The relatively high volume of other diseases in our centre would suggest that although the above factors are significant, they cannot explain the situation.
The identified rare diseases are usually quite symptomatic, to the extent that victims would be compelled to see a doctor. It is difficult to imagine that any case of TN would dodge seeing a doctor. Skull base tumours are ultimately symptomatic producing serious neurological deficits including visual impairment, motor and sensory deficits and raised ICP, hence the patients would ultimately be referred for imaging and neurological/neurosurgical management.
The catchment population for this study is in Southeast Nigeria, which ranks as one of the most literate populations in Africa, hence healthcare awareness is therefore high. With the high CT and MRI volumes, even asymptomatic rare pathologies could be picked up in patients being investigated for other problems, but this has not been the case.
Genetic factors have been incriminated in the aetiology of the diseases listed. This is true of cavernomas, MMD, chordomas, some pineal tumours, and VS. Familial and inheritance factors have been confirmed for some of these lesions especially NF2. Trigeminal neuralgia shows high prevalence in some countries like Korea [18].
The role of environmental, dietary, and geographical factors is unclear. If other countries in sub- Saharan Africa confirm similar low frequency, researchers could then search for the factors responsible for protecting Africans. If, however, the variations are only in select communities or regions, then the search could be narrowed down to those areas. The rarity of these pathologies supports the view that geographical neurosurgery deserves more attention [2].
This is a single centre study but during the study period, the centre was the main referral hospital for neurosurgery for the sub-region. Out of pocket payment might have influenced the frequency as some patients might have avoided seeking for help.
Some neurosurgical pathologies that contribute significantly to high workload in most countries are rare in our centre located in sub-Saharan Africa. The rarity of these neurosurgical diseases in the study region poses a research challenge. Identification of the cause(s) would be a major scientific breakthrough in epidemiology and prevention of diseases.
The authors have nothing to declare and received no financial assistance. No conflicts of interest