Keutel syndrome is rare inherited disorder with mutations in the matrix G1a protein (MGP). Most of the patient is diagnosed in early childhood. They admitted to the hospital due to hearing loss, recurrent upper respiratory tract infections, chronic cough. In this case report Keutel syndrome is discussed in an adult patient.
Keutel syndrome, Spirometry, Asthma, Rare disease
Keutel syndrome is extremely rare autosomal recessive genetic disorder which is chacterazied by calcification of externalears, nose, larynx and trachea. Additionally recurrent otitis, hearingloss, nasal speech, frequent respiratory tractinfections, short stature, hypo plastic midfacial feature, mild intellectual disability, brachy telephalangism (shortening and broadening of the first to fourth distal phalanges), pulmonary arter stenosis and asthma like symptoms such as wheezing are other clinical features [1,2]. Genetical studies shows loss of function mutation on matrix GI a protein associated with defective mineral deposition resulting with abnormal calcification of skeletal and vascular tissues lead to primary pathological mechanism underlying the Keutel syndrome [3]. Due to the diversity of the clinical picture, patients can be seen in many different forms and therefore the diagnosis may be delayed. In this case report we aim to present patient Keutel syndrome diagnosed at adultage.
A 21-year-old female patient referred to the pulmonary disease department with complaints of frequent dyspnea and chronic cough episodes. In her medical history, she was diagnosed with asthma and regularly treated with broncho dilatators from childhood. In addition to that; hearing loss, recurrent otitis and respiratory tract infections, nasal speech, mild intellectual disability were significant. Her physical examination shows that mid face hypoplasia, receding chin, forehead sloping and prominent wheezing (Figure 1). There was no abnormal demonstration on chest x-ray. Computed tomography revealed diffuse cartilage calcification of tracheal rings as often seen on the routine (Figure 2). Also, pulmonary function test showing the plateu during inspirium and expiriumphases on flow-volume curve and FEV1/FVC result is 62% indicating obstructive respiratory disease with fixed obstruction pattern (Figure 3).
 Figure 1: Her physical examination shows that mid face hypoplasia, receding chin , forehead sloping.
View Figure 1
Figure 1: Her physical examination shows that mid face hypoplasia, receding chin , forehead sloping.
View Figure 1
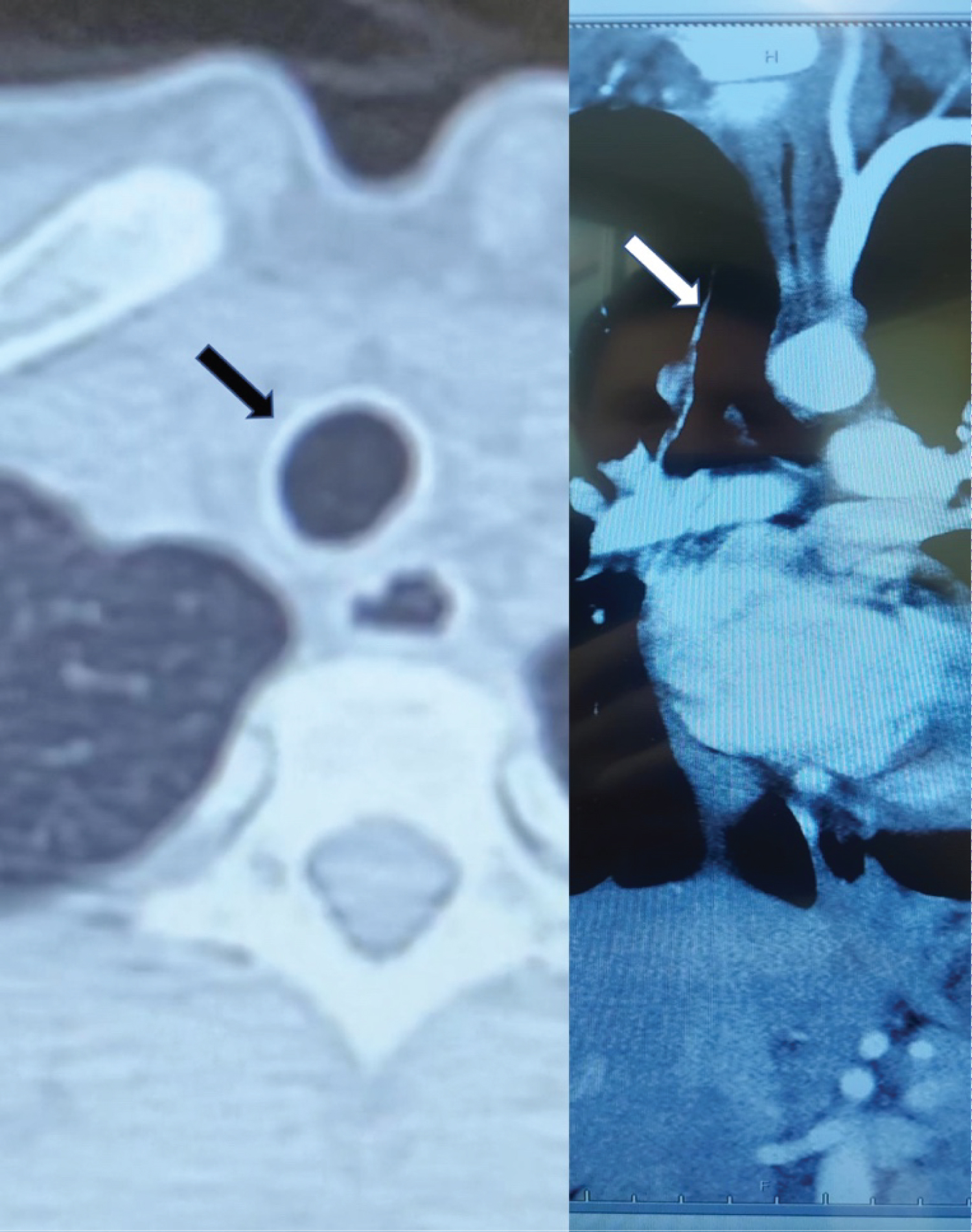 Figure 2: Computed tomography revealed diffuse cartilage calcification of tracheal rings as often seen on the routine.
View Figure 2
Figure 2: Computed tomography revealed diffuse cartilage calcification of tracheal rings as often seen on the routine.
View Figure 2
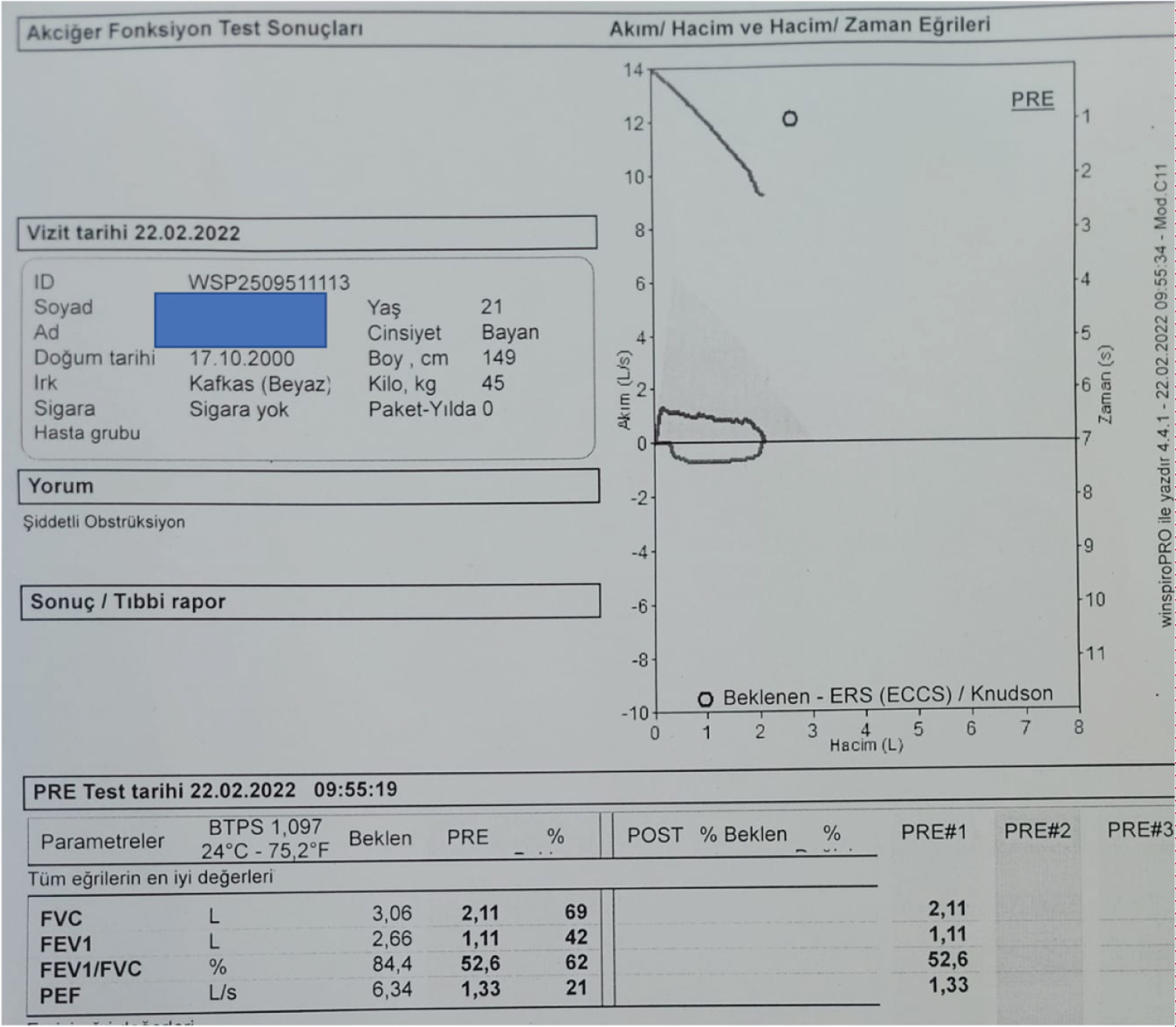 Figure 3: Pulmonary function test showing us plateu during inspirium and expirium phases on flow-volume curve and FEV1/FVC result is 62% indicating obstructive respiratory disease.
View Figure 3
Figure 3: Pulmonary function test showing us plateu during inspirium and expirium phases on flow-volume curve and FEV1/FVC result is 62% indicating obstructive respiratory disease.
View Figure 3
First case described in 2 siblings who have consanguineous parents in early 1970s [1]. Less than 100 Keutel syndrome studies has been reported in the literature that shows us how rare inherited disease is, all around world [4]. It affects multiple organs systems and degenaration tends to be more severe by increasing age In this context, we could encounter with variable clinical results in wide spectrum and quite hard to diagnose. Furthermore, due to existence of phenotypic variability and mild cases some patience of Keutel syndrome remain undiagnosed [5]. Symptoms seen in Keutel syndrome thought to be result of secondary to calcification, mainly. Seizure, epilepsy and developmental delay could be explained by intracranial calcification. Tracheobronchial calcification could be responsible for dypnea and cough by inducing trachea and bronchi stenosis and diminishing respiratory tract elasticity. Moreover, auricular and pinneal calcification tend to be reason of hearing loss [3]. Reported studies shows us the prevalence of Keutel syndrome is 1:1000000, very rare autosomal inherited disorder. Keutel syndrome is need to be considered in the patient who has severe asthma with facial anomalies and nasal speech. By spirometry and detailed clinical examination diagnosis can be easily made [1-8].
Keutel syndrome is rarest condition which is considered for differential diagnosis of severe asthma. In this case patient was unresponsiveness to appropriate treatment. No data has been found in published studies that flatten curves in spinometry diagnostic criteria of Keutel syndrome. Curve flatting during inspirium and expirium due to calcifications of tracheal rings resulting with diminishing of tracheal cartilage elasticity. This curve flatting is called as fixed obstruction, pathophysiological findings of Keutel syndrome, reported for the first time in this case report. Majority of reported cases in the literature supported by genetic mutations. Diagnosis could be easily made via physical examination, radiological studies and spirometry test without performing genetic conformation.
To conclude, Keutel syndrome should be considered in patient with severe asthma and other characteristics. Since many different etiologies of asthma can be seen, differential diagnosis need to be made very carefully. Despite, existence of phenotypical variety showing calcifications in the tissues (especially trachea) by radiological examinations, flatten curves in the spirometry test and no response to asthma treatment together with typical facial features should remind us Keutel syndrome.