Background: To evaluate the mortality rate of deaths from suicidal acts in Joinville (SC) from 2019 to 2020.
Methods: The data were collected using the information contained in the Violence Prevention Center base regarding the notifications from the Notifiable Diseases Information System (SINAN), information about the deaths was selected and divided in age, sex, marital status, schooling, neighborhood, place of death and code of the International Disease Classification applied. The variables were analyzed and detailed through the article.
Results: It was possible to identify that the main population profile of deaths by suicide occurred ‘in men in the age group of 30 to 39 years, single and whose death occurred in their own homes by hanging, strangulation and suffocation.
Conclusion: From the epidemiological profile studied in this article it becomes possible to elaborate prevention measures and offering refuge for individuals at risk to commit suicide.
Suicide, COVID-19, Prevalence
HIV: Human Immunodeficiency Virus; AIDS: Acquired Immunodeficiency Syndrome; COVID-19: Coronavirus Disease 2019; MIS: Mortality Information System; ICD-10: International Classification of Diseases 10th Revision BSI: Brazilian Statistics Institute; BCO: Brazilian Classification of Occupations; WHO: World Health Organization
Death by suicide is a serious public health problem worldwide and it is one of the main causes of death, surpassing deaths from malaria, human immunodeficiency virus (HIV)/acquired immunodeficiency syndrome (AIDS), breast cancer, wars and homicides. Every year, 703,000 people die by suicide worldwide. More than one in 100 deaths (1.3%) in 2019 was a result of suicide. It is the second leading cause of death among young people aged from 15 to 29-years-old [1].
Suicide is understood as any self-inflicted injury, which the intention is, even if in an ambivalent way, the death. In turn, the suicide attempt corresponds to the self-harm behavior with a non-fatal outcome, accompanied by evidence, either explicit or implicit, that the person intended to die [2].
It is important to situate suicide as a complex phenomenon with a multifactorial etiology. The factors involved in suicidal behavior range from adverse experiences in early life, genetic and cultural characteristics, to factors such as traumatic experiences and abuse of psychoactive substance. Social, economic and environmental issues also contribute to the suicidal act. The phenomenon affects families, communities and countries, generating disruptive impacts on people who are part of the victims' social bonds [3].
Furthermore, it is of great importance that there is an understanding that suicide corresponds to an individual experience, marked by the ambiguity between the search for death, as a form of ending the suffering, and the yearning for help.
In 2019, the majority of suicide deaths occurred in low and middle-income countries (77%). Of these, more than half of the cases (58%) occurred in individuals younger than 50-years-old. The deaths resulting from suicidal acts represented the fourth leading cause of death for both genders among young people, aged 15 to 29, followed by traffic accidents, tuberculosis and interpersonal violence [4].
In a study that gathered data in the period between 1996 and 2019, it was observed that there were 222,232 deaths from suicidal acts in Brazil, with an average of 9,260 deaths annually. This equates to 25 suicides per day, and one every hour. Analyzing suicide mortality among Brazilian states, it was proved that all states in the southern region of the country had suicide rates above the national average. The states of Rio Grande do Sul and Santa Catarina stand out, with the highest suicide rates in the country [5].
It is important to emphasize that suicide and self-violence are stigmatized and underreported events. The stigma in relation to the topic, as well as to mental health, often makes it difficult for people to look for help, which could prevent fatalities [6].
A responsible approach to the phenomenon of suicide is more related to a factor of prevention than to a risk factor, and may even contribute to break the stigma that surrounds them [7]. Among the prevention strategies, it is necessary to involve leaders, managers and health professionals in the planning of strategic actions, in the definition of interventions aimed at prevention and in the intersectoral articulation, creating support networks for the community [8].
In 2020, because of the Coronavirus pandemic, measures were implemented by many countries to slow the spread of Coronavirus Disease 2019 (COVID-19). Regulations ranged from physical/social distancing to the total blockade of cities. Emerging research points to the consequences for the mental health from COVID-19 as different from previous pandemics, with symptoms of anxiety, depression and stress being common [9].
The findings of the present study aim to explore the prevalence of suicide in the city of Joinville, Santa Catarina (Brazil), between 2019 and 2020 and the epidemiological profile of individuals who practiced suicide in the mentioned period. It is hoped that, from this information, can be provided the theoretical basis for the implementation of actions by health professionals, contributing with subsidies for suicide protection and prevention programs.
This is a descriptive study on the epidemiological profile of individuals who died due to suicide in the city of Joinville, from 2019 to 2020. The city of Joinville is located in the Northern region of the State of Santa Catarina and has an estimated population of 604,708 inhabitants, with a population density of 457.58 inhabitants per square kilometer, whose residences are located mostly within the urban perimeter. The secondary sector imposes a majority of the activities related to the economic sector, with a 10.01% share of manufacturing sector and 6.47% of services (JOINVILLE MUNICIPALITY, 2021).
Through the data available in the Mortality Information System (MIS), through the DATASUS, it was possible to identify the number of deaths by suicide, considering the self-harmed injuries, ICD-10 (International Classification of Diseases 10th Revision) X60 to X84), which took place in Joinville during the years 2019 and 2020. The numbers of deaths by suicide occurring in national, regional and state territory were also collected from the DATASUS.
Such deaths were categorized according to the 10th edition of the International Statistical Classification of Diseases and Related Health Problems (ICD-10). Information such as gender, age, education, relationship status, occupation, neighborhood, most common methods of suicide and location of death were similarly extracted from the MIS. With this information, was made a descriptive analysis of the sociodemographic profiles (gender, age, education, relationship status and occupation) and occurrence (means and place of death) of deaths.
The global mortality rate was obtained by dividing the number of deaths by suicide by the resident population of Joinville. Specific mortality rates by gender (male and female) were calculated by dividing the number of deaths by gender by the total male or female population in each year studied. Mortality rates according to age (15 to 19; 20 to 29; 30 to 39; 40 to 49; 50 to 59; 60 to 69; 70 to 79 and 80 years or older) were obtained by dividing the number of deaths in each age group by the total population in each corresponding age group in each period. The mortality rates specific by region of Joinville were calculated by dividing the number of deaths found in the neighborhoods by the population of those neighborhoods.
The sociodemographic data were extracted from the Brazilian Statistics Institute (BSI). The classification according to the occupation of each case was determined according to the Brazilian Classification of Occupations (BCO) and subdivided into 9 major occupational groups.
This research was approved by the Research Ethics Committee of the University of the Region of Joinville (UNIVILLE), as stated in Opinion No. 4,547,509 and Certificate of Presentation of Ethical Appreciation (CPEA) 10197519.00000.5366.
In the years 2019 and 2020, there were 95 deaths by suicide in the city of Joinville, with 44 occurring in 2019 and 51 in 2020. Taking into consideration the population projections for the years in question, can be calculated the specific suicide mortality rates, that ranged from 7.45 deaths to per 100,000 inhabitants in 2019 and 8.53 deaths per 100,000 inhabitants in 2020.
By analyzing the profile of individuals who attempted suicide in the aforementioned period, can be verified that the majority were male (80%) and single (42.1%). Regarding to the level of schooling, the majority cases of suicide occurred by individuals who completed high school prevail (31.5%), followed by incomplete higher education (27.3%) and those who attended the 5th to 8th grade (23.1%).
The mortality rate in men in the year 2019 was 11.61 deaths per 100,000 inhabitants, rising to 14.18 deaths per 100,000 inhabitants in 2020. For females, 2019 presented a rate of 3.35 deaths per 100,000 inhabitants, falling to 2.98 deaths per 100,000 inhabitants in 2020 (Figure 1).
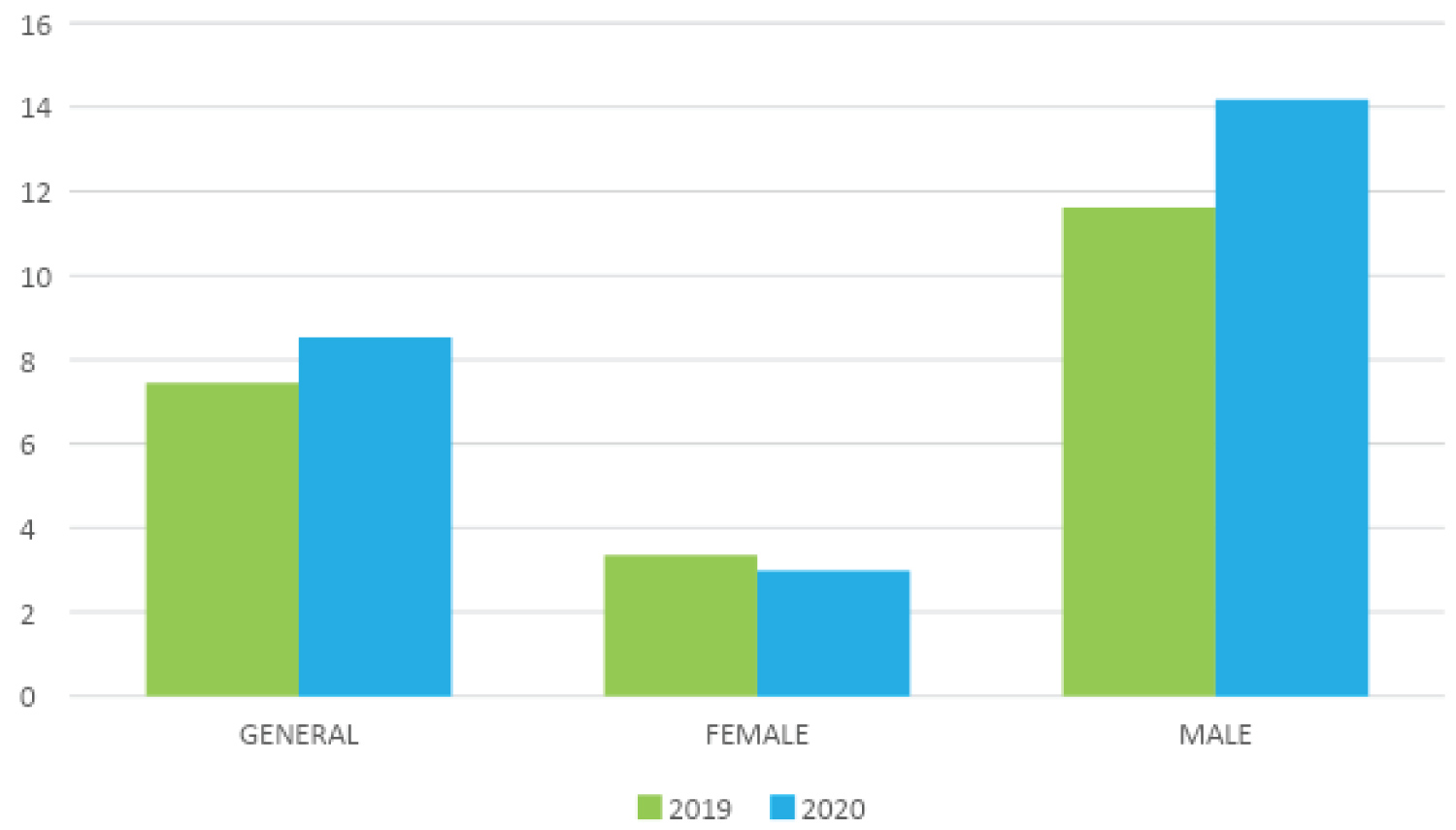 Figure 1: Suicide mortality rates per 100,000 inhabitants found in Joinville in the years of 2019 and 2020.
Figure 1: Suicide mortality rates per 100,000 inhabitants found in Joinville in the years of 2019 and 2020.
Source: Baptista, et al., 2022; data extracted from the MIS and BSI.
View Figure 1
Regarding the age group, it was possible to verify that there was a higher occurrence of deaths in the age from 60 to 69-years-old (n = 11) and from 30 to 39-years-old (n = 13) if we analyze the absolute numbers of 2019 and 2020 respectively. However, when we look at the specific mortality rates, it can be seen that in 2019, the most prevalent age group was 60 to 69-years-old (23.4 deaths per 100,000 inhabitants). For the year of 2020, the data indicate that the most prevalent age group was 70 to 79 years (30.8 deaths per 100,000 inhabitants). When comparing the 2019 data with the 2020 data, it was possible to observe an increase in the rates related to the younger age groups, from 15 to 39-years-old, a decline among people aged 40 to 69 years and a substantial increase in rates involving elderly people aged over 70-years-old (Table 1).
Table 1: Mortality rate per 100,000 inhabitants calculated by age group in 2019 and 2020. View Table 1
When the analysis included, in addition to the age group, the gender of the individuals, it was found that in the male gender, there was a predominance of events in the age group from the age of 60-years-old in 2019 and from the age of 70-years-old in 2020. In males, there was also a substantial increase in rates in 2020 compared to 2019 in the 20-39 age groups and those over 70. There was a reduction in mortality rates in the 15-19 and 60-69 age groups (Table 2).
Table 2: Mortality rates per 100,000 inhabitants according to gender and age group. View Table 2
Among females, in 2019, the most prevalent age group was from 70 to 79-years-old, while in 2020 the women over 80-years-old had the highest mortality rates. Of the 8 age groups present in the data collected, 5 showed a reduction in mortality rates in 2020 when compared to 2019 (Table 2).
Regarding the occupations of each case, there was a higher occurrence of deaths in workers in the production of industrial goods and services (34.7%) such as bricklayers (n = 10) and machine operators (n = 5), followed by mid-level technicians (12.6%), such as sales representative autonomous (n = 4). It is worth noting that there were cases of suicide among students (n = 6), corresponding to 6.31% of all cases in the years studied.
When observing the place of death, the number of suicides that occurred at home prevails (65.2%), followed by deaths in other unspecified places (15.7%), hospital (12.6%) and finally in public (6.3%). Analyzing the ICD-10 applied to death records, it is found a majority in deaths due to hanging, strangulation and suffocation by ICD-10 X70 (73.6%), followed by self-intoxication (9.4%) and shooting by firearm (8.4%).
The analysis of the place of residence of each individual showed that both in 2019 and in 2020, the rural region had the highest rates, with 40.7 deaths per 100,000 inhabitants. In 2019, the second region with the highest mortality rate was the center north with 16.6 deaths each 100,000 inhabitants. In 2020, in addition to the rural area, the southwest and west regions stand out with 21.7 and 18.3 deaths per 100,000 inhabitants respectively (Figure 2).
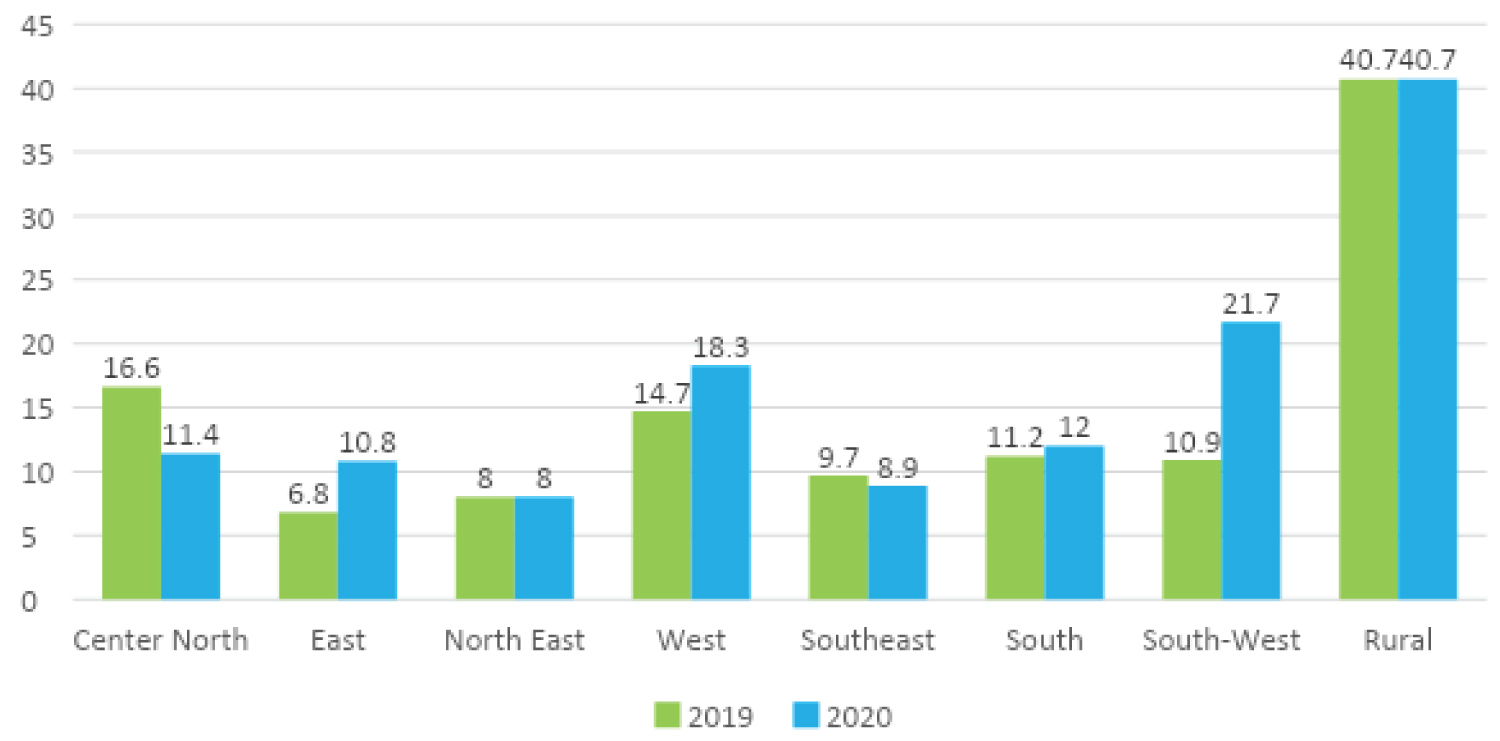 Figure 2: Suicide mortality rates per 100,000 inhabitants according to the regions of Joinville in the years 2019 and 2020.
Figure 2: Suicide mortality rates per 100,000 inhabitants according to the regions of Joinville in the years 2019 and 2020.
Source: Baptista, et al., 2022; data extracted from the MIS and Joinville Municipal Health, 2021.
View Figure 2
According to the World Health Organization (WHO), every 40 seconds a person dies by suicide worldwide, while suicide attempts are estimated to occur once every two seconds [1]. The numbers are alarming despite the literature showing that the phenomenon can be preventable and avoidable. The consonance of prevention instruments is essential and must unite public health policies that involve doctors, nurses, health workers, psychologists, social workers, teachers, media workers, in addition to institutions to support the population.
As demonstrated by Plucinski A, et al. [10], Joinville showed a reduction in rates of suicide mortality from 8.4 deaths per 100,000 inhabitants in 2016 to 7.2 deaths per 100,000 inhabitants in 2018. The present study showed that the city maintained its rates at 7.45 deaths per year per 100,000 inhabitants in 2019, rising to 8.53 deaths per 100,000 inhabitants in 2020. Therefore, it can be inferred that there was a brief increase in cases and that this increase corresponds approximately to the same number of deaths per 100,000 inhabitants in 2016.
The increase in this rate may be related to the continuity of the state of social isolation imposed by the COVID-19 pandemic that started in 2019 and lasted until the year of 2020. Social isolation is described in the literature as a risk factor for suicidal behavior along with economic vulnerability, increased fear, reduced physical activity and exacerbated use of alcohol, these being risk factors for depression, anxiety and other psychiatric disorders [11].
In the pandemic, several studies indicated a trend of increasing suicide, mainly in the young population, in countries of different incomes (JOHN, 2020). Dubé, et al. [12], in their recently published meta-analysis, showed that the results suggested increased event rates for suicidal ideation (10.81%), suicide attempts (4.68%) and self-harm (9.63%) during the COVID-19 pandemic when compared with event rates from pre-pandemic studies, illustrating a real impact on mental health of the population in the period [13].
Related to this, it is worth emphasizing that the mental disorders most frequently associated with suicidal behavior are: depression, bipolar disorder and dependence on alcohol and other psychoactive drugs. In addition to these, schizophrenia and some personality characteristics represent important risk factors, and the same is aggravated when one of these conditions coexist [14].
As described in the present study, in 2019 it is much more prevalent the mortality rates in the population aged 60-70 years-old. In 2020, young people aged 20-39 years-old and elderly people aged 70-79 years-old were the groups that showed the biggest increase in mortality rates. This may illustrate that the social isolation of coexistence may have resulted in major impacts on the health of these populations. For Pappis, et al. [15] the young people are influenced by integrating institutions, such as the family and the school, which generate security for them. The fragility of these institutions determines less attention in training of these subjects, which can generate feelings of isolation, loneliness, insecurity, anxiety, sadness among others that lead to depression. In addition, the stress generated by a loss or an interpersonal conflict is present in 70% of suicide cases among young people [16].
On the other hand, the elderly is influenced by the aging process itself, which is characterized as being dynamic, progressive and irreversible, linked to biological, psychological and social factors. Symptoms of depression associated with tension, agitation, guilt, dependence on others to perform daily tasks, inflexibility, impulsiveness, changes in eating and sleeping habits, chronic organic disorders, having low self-esteem, being distant or having little contact with the family are some of the various risk factors for suicide in old age [17].
By analyzing what was demonstrated in this study, it was also possible to identify the higher prevalence of cases of suicide among males (80%). This fact can be explained by this population tend to reach the goal of death by choosing more violent and lethal means than the female gender, as for example hanging and the use of firearms [18]. In our study in Table 2, the profile of the man over 60-years-old is illustrated. However, after the beginning of the pandemic, there was an increase in the population aged 20-40 years regarding mortality rates.
Composing the epidemiologic profile presented, it was verified that 42% of cases are attempted by single people. This data is in line with what Gomes, et al. [18] evidenced in the period from 2013 to 2017 in Rio Grande do Sul. The authors report that people without partners do not have the protective factor, that consists of an affective bond. In addition, the profile traced in this work demonstrates that the rates are bigger among students who completed high school prevail (31.5%), followed by of those who attended incomplete higher education (27.3%) and those who attended the 5th to 8th grade (23.1%). The influence of schooling is not much discussed in the literature, but some studies stand out that, in addition to the employment situation and the family income, the low schooling is one of the criteria that determine the economic and social status, causing distinct concern levels, stress and frustration [16].
Regarding the methods chosen for suicide, the current research pointed to the highest rates per hanging, strangulation and suffocation (73.6%), which coincides with the rate presented by Lovisi, et al. [19], who showed that 47% of deaths from 1980 to 2006 occurred for the same reason described. The authors also realized that the preferred methods of men to attempt suicide are hanging (58%), followed by firearm shooting (17%) and pesticide poisoning (5%). Among women, the most used method is hanging (49%), followed by poison by gas (9%) and jump from height (6%).
The analysis described in the present study enables a better understanding of the subject through mapping the epidemiological profile of suicides in the city of Joinville, contributing in an accurate way to plan preventive actions for the local population. Among this population, vulnerable groups should be considered with greater political focus in terms of public protection and social solidarity.
This study was not supported by any financial sources. No conflict of interest to this article was reported. The authors declare that each author have equal contribution to the manuscript.
There is no funding.
All authors have contributed to the work and manuscript writing equally.