Introduction: The application of external fixation devices consists of wires insertion through the skin and soft tissue to the bone. We examined the possible analgesic effect of stimulating an acupoint by the fixation wires which mimics the acupunctures treatment.
Material and methods: Retrospective work. Between 2015 to 2018 107 patients were treated with an external fixation for a tibial fracture. 33 patient files were found to be eligible for the review. Patients were retrospectively divided into two groups: The study group included patients with a wire inserted through the ST36 (Zu San li) acupoint location, the control group had the wire inserted elsewhere. Patient's record was reviewed for 5 days following surgery. Data collected included analgesic consumption and pain level recorded on a visual analog scale (VAS).
Results: 33 patients were included in the review. 20 patients in the study group and 13 served as the control group. In the study group VAS average was Mean (M) = 1.4853 ± 1.30 while in the control group M = 2.3885 ± 1.77 with no statistical relevance (P > 0.05). Only on day 4 the study group had less pain than the control: M = 0.40 ± 0.843, versus M = 2.57 ± 2.149 (Mann = Whitney Z = -2.413, P < 0.05). No statistical difference was found between groups in relation to analgesic consumption.
Conclusions: In patients suffering from a tibial fracture treated with an Ilizarov external fixation device, locating a wire in the anatomical location of acupoint ST 36 had no effect on analgesic consumption and a minimal effect on patients' pain levels.
External fixation, Acupuncture, Pain, Orthopedic, Chinese medicine
Tibial shaft fractures are the most common fractures of long bones, with an incidence of 26-100,000 per year. The average age of patients is 37, with a male-female ratio of 3.5:1 [1]. Tibial shaft fractures commonly occur following high energy impact (HEI) - motor vehicle or extreme sport accidents and war zone casualties. The use of an external fixator device (EFD) is indicated in conditions such as infected fracture, interruption of bone coverage, when the medullary is too narrow for intramedullary nail, or as a temporary treatment, when definitive surgery is delayed for some reason [1].
The EFD consist of wires and screws that are placed through the skin and into the bones, while the external pole is attached to a bar (unilateral), or wires that cross the bone and both external poles are attached to a ring (circular) (Figure 1).
 Figure 1: An Ilizarov external fixation device for treating a tibial fracture.
View Figure 1
Figure 1: An Ilizarov external fixation device for treating a tibial fracture.
View Figure 1
Surgeons determine the wire insertion sites according to fracture location, in consideration of the adjacent anatomic structures. The choice of the insertion site is critical, in order to avoid further damage to local tissue - nerves and vessels and to avoid fixating of tendons and muscular masses, which limit the adjacent joint’s range of movement. Referring to tibial fractures, in choosing the wires’ insertion site, the posterior compartments should better be spared as much as possible, in due to the muscular mass presents. The lateral aspect of the upper third of the shin contains the peroneal nerve and the posterior aspect containsthe popliteal artery. The lower third, on its medial posterior aspect contains the tibial nerve and tibial artery. As a result, the anterior aspect on the shin is commonly used as a wire insertion site [2]. This site is anatomically similar to the location of acupuncture point St 36 also known as Zu San Li. The acupoint is located on the anterolateral aspect of the tibia, 6 centimeters below the knee joint and 2 centimeters lateral to the anterior tibial crest [3]. According to The World Health Organization (WHO) ST36 is located on the anterior aspect of the leg, on the line connecting ST35 with ST41, 10 cm inferior to the depression lateral to the patellar ligament [4,5]. St 36 is one of the most commonly used acupoint in an acupuncture treatment, with variable indications such as neuromuscular pain, stomachache, pain syndrome, hypertension, diabetes and gastrointestinal disorders (Stuart S. Anatomical Atlas of Chinese Acupuncture Points. The Cooperative Group of Shandong Medical College and Shandong College of Traditional Chinese Medicine, 1990). Moreover, it is one of the most researched acupoint, with numerous studies examining its effect on various medical conditions [6-10].
Acupuncture has been used therapeutically in China for thousands of years and is growing in popularity throughout the developed world [9]. Acupuncture treatment is based on the insertion of fine needles in various anatomical points, called acupoint Acupuncture treatment is associated with significant changes in bioactive chemicals- including opioids, N/OFQ, serotonin, norepinephrine, glutamate receptors and transporters, cytokines, and signal molecules in peripheral injury sites, the spinal cord, and supraspinal structures [11,12]. Acupuncture is commonly used for pain management. Various studies have shown that acupuncture is safe and cost-effective compared to routine care [13-20]. It has been indicated that certain modes of acupuncture improved postoperative pain on the first day after surgery and reduced opioid use [15]. This study examines the possible analgesic effect of locating an EFD wire in the similar anatomical location of acupoint St 36, and the possibility of the EFD wire creating acupuncture like effect as a result of its anatomical location.
Upon searching literature, few authors suggest the complementary treatment of acupuncture for acute post orthopedic operation pain [13,15,18]. Only one study examined the possible effect of the EFD’s wires on acupoints (Verkhozina T., Solomin SL. Results Analysis of S-screws and K-wires Insertion through Acupuncture Points. unpublished data, 3 rd Meet ASAMI Int - Istanbul 2004), although, no studies were conducted with the goal of examining the possible pain relieve due to the insertion on the EFD’s wires through acupoints.
The study was approved by the Ziv Helsinki ethics committee. Data was collected retrospectively using the Ziv medical center archive. Patients’ records were reviewed between the years 2015 to 2018. A total of 107 patients treated with an EFD (the majority with Ilizarov EFD device) after tibial fractures were found. 13 patients’ files were excluded due to age limit (below 18 or above 80-years-old), 18 patients were excluded due to post-operation hospitalization that was shorter than 5 days, 36 patients were excluded for multi trauma injury, 8 cases were found to be recorded twice due to two separate admissions, thus, excluded and finally, 13 patients were excluded due to missing hospitalization data.
33 patient files were found to be eligible for the review. Males and females, aged 18-80, demographic data included Israeli citizens (Jews and Arabs) and 5 Syrians war casualties treated in the Ziv medical center, as well as one Thai immigrant.
All patients suffered from tibial fractures, open or closed, with no other major injuries. All patients were treated with an external fixator device, either as temporary or definitive treatment.
Following reviewing patients’ X-ray records (Figure 2), Patients were divided into two groups. The study group (SG) included 20 patients having one of the external fixation device’s wires inserted through the ST36 (Zusanli) acupoint location, the control group (CG) included 13 patients that had the external fixator device’s wire inserted elsewhere on the proximal anterior tibia, in a non-acupoint location. The exact insertion points were determined by the operating surgeon during the surgery, based solely on the specific requirements of each fracture, such as its extent, shape, and stability.
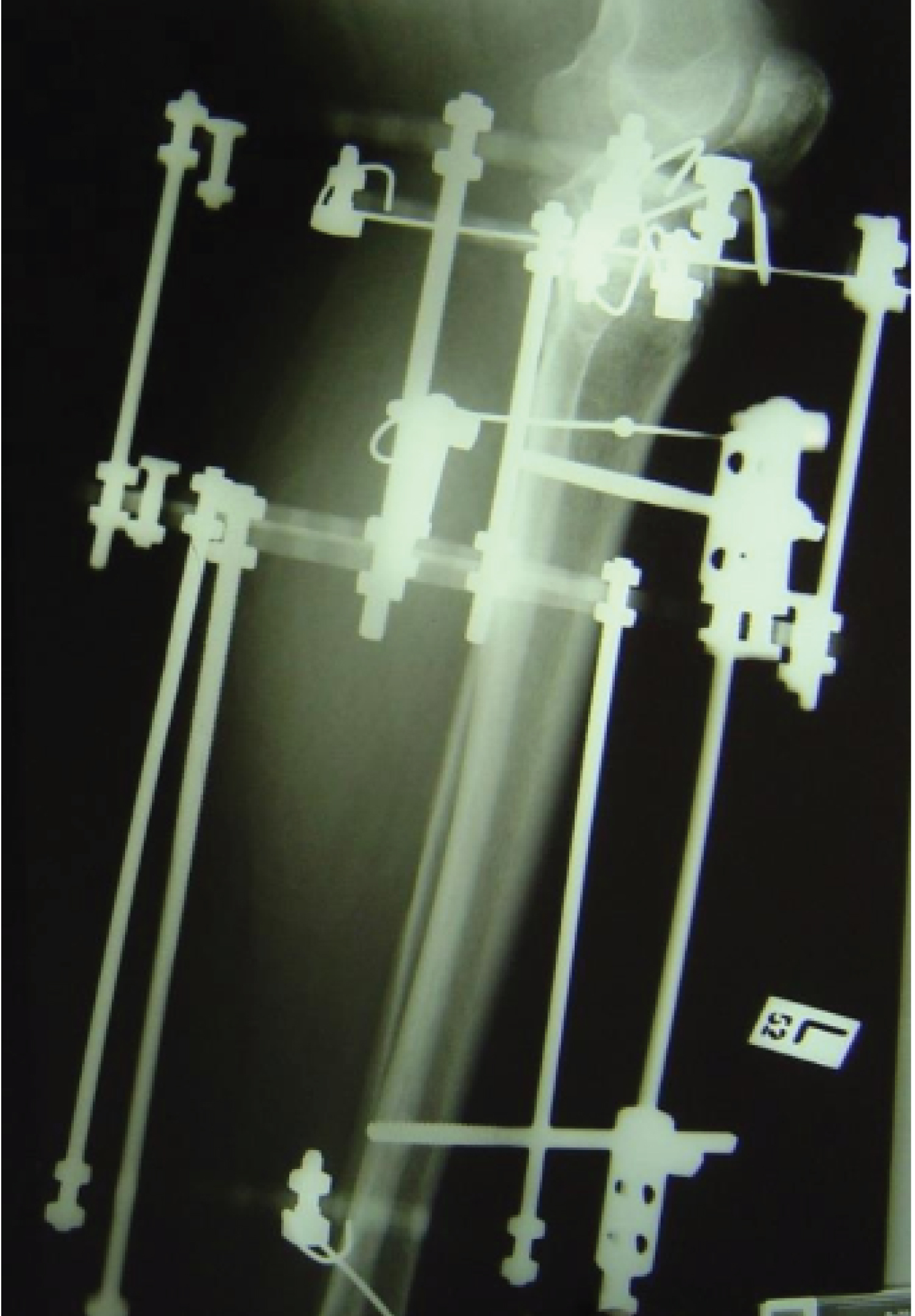 Figure 2: An example of a plain radiograph of an external fixation device placed on the tibia bone.
View Figure 2
Figure 2: An example of a plain radiograph of an external fixation device placed on the tibia bone.
View Figure 2
The SG included 14 males and 6 females. The average age was 42.5. The CG included 10 males and 3 females. The average age was 47.7. Patient's records were retrospectively reviewed for 5 days following surgery. Patients’ data collected for the study included Pain level and analgesic consumption. Pain level was measured by the use of a VAS (visual analog scale- 0 no pain, 10 Max pain). Pain level is taken three times a day as a standard practice in the orthopedic department. Patient's Analgesic consumption for 5 days following surgery was also reviewed, to be used as second parameter for patient's pain level.
The drugs that were registered include: Metamizole ( OPTALGIN ® ), Oxycodone, Oxycodone with Acetaminophen (Percocet ) , Oxycodone with naloxone controlled-release (CR) tablets ( Targin ) and Tramadol Hydrochloride (Tramadex OD PO, Tramadex IV).
Statistical analysis: For categorical variables, summary tables provided giving sample size, absolute, and relative frequencies. For continuous variables, summary tables provided giving arithmetic mean (M) and standard deviation (SD). Pearson’s chi-squared was applied for testing the correlations between the study groups for the categorical parameters. Pearson correlations provided the power of the correlation between the continuous variables. The independent sample t-tests groups or Mann Whitney non parametric test was applied to measure the differences between the study (control vs. cases).
P-value of 5% or less is considered statistically significant. The data was analysed using the SPSS version 25 (SPSSInc., Chicago, IL, USA).
Demographic data is presented in Table 1 and Table 2. Pain levels as measured by VAS are summarized in Table 3. No statistical difference was found between the control and study groups (2.3885 ± 1.77 for the CG and 1.4853 ± 1.30 for the SG, xxx P value) although a slight tendency towards the SG can be detected. Only on day 4 of hospitalization there was a statistical difference between the study groups (0.40 ± 0.843 among the SG and 2.57 ± 2.149 among the CG (Z = -2.413, P < 0.05. calculated by the Mann-Whitney U). Regarding analgesic consumption, no statistical difference was found in the total consumption (the number or times an analgesic drug was taken, regardless type or dose), among the SG, the average consumption was 8 ± 3.71 and among the CG the average was 9.31 ± 4.9 (Table 4). Observing each drug separately, no statistical correlation was demonstrated (Table 5). Some drugs were consumed more among the CG, whereas other drugs were higher among the SG.
Table 1: Demographic data. View Table 1
Table 2: Demographic data. View Table 2
Table 3: VAS. View Table 3
Table 4: The total consumption of analgesic drugs. View Table 4
Table 5: The consumption of each analgesic drug separately. View Table 5
The location of an external fixation device following a tibial fracture involves many anatomical considerations. The possible positive effect of inserting a surgical wire\nail through an active acupuncture point has yet to be studied.
Postoperative pain results from surgical trauma and is a significant challenge for healthcare providers. About 75% of patients experience moderate or severe pain following surgery [16]. The mainstay of treating postoperative pain is the use of opioid analgesics such a morphine, hydro morphine, meperidine, or fentanyl. However, these drugs are associated with a number of undesirable side effects which can delay patient recovery including nausea, vomiting, dizziness, sedation, and decreased gut motility [14]. A delay in opioid consumption can be considered a proxy of lower pain levels; it has been suggested that acupuncture led to a modest delay in analgesic requests, leading to possible benefits in the critical immediate time window following surgery. Similarly, Tedesco, et al. have found that acupuncture provides significant pain improvement in patients undergoing TKA and total hip arthroplasty in the first 2 days after surgery [15].
It is important to emphasis the differences between standard acupuncture treatment and the external fixation devices (Table 6 and Figure 3). Both the acupuncture needles and the Kirschner wires are made of stainless steel. However, the needle’s diameter is significantly smaller, as well as its depth or penetration. Moreover, the duration of stimulation is also to be noted. The acupuncture needle remains inserted for up to thirty minutes, while the external fixation devices stay in place for days or months.
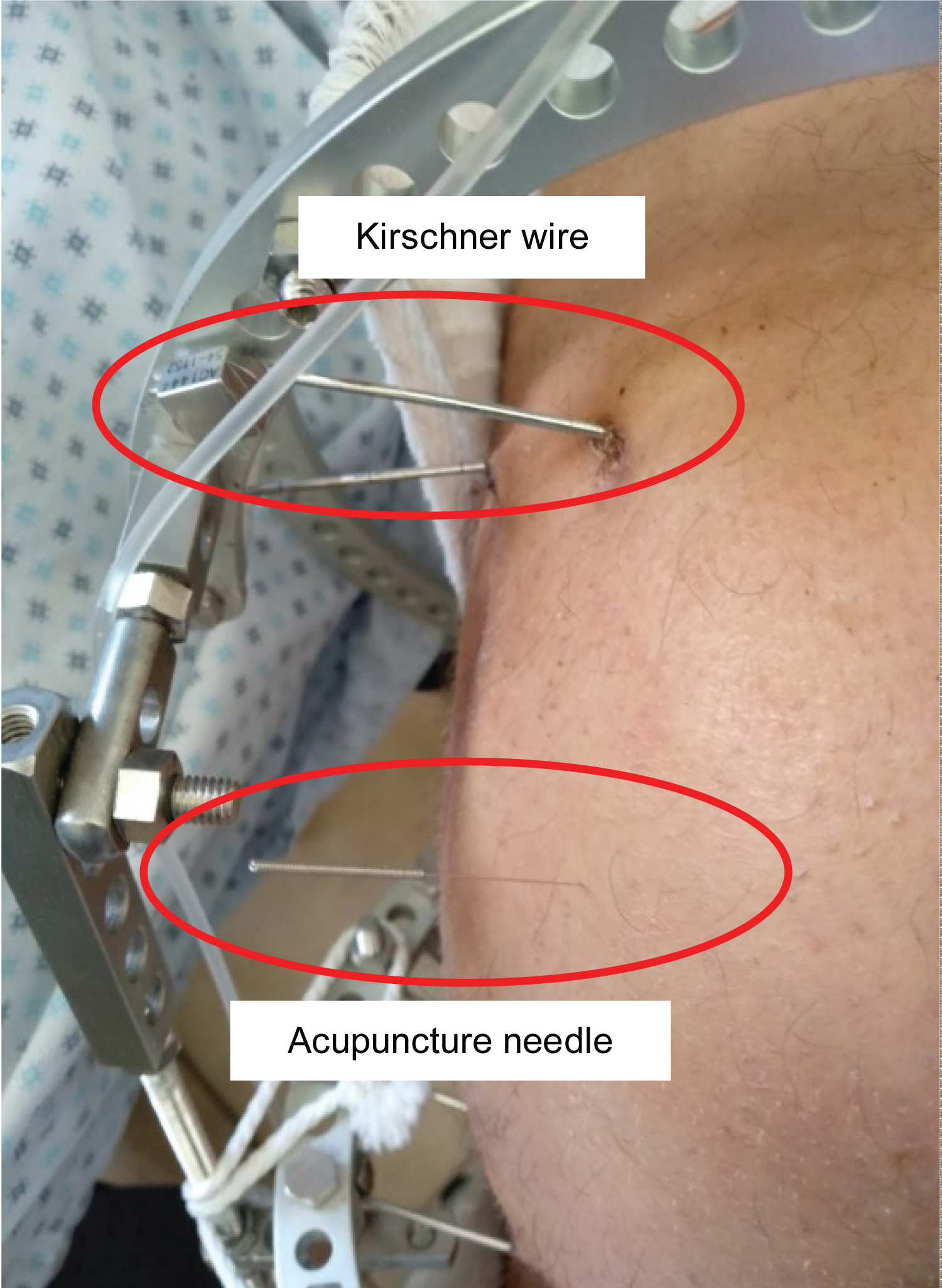 Figure 3: An acupuncture treatment to a patient with a tibial fracture fixated by Ilizarov. Enables the comparation between an acupuncture needle and a Kirschner wire.
View Figure 3
Figure 3: An acupuncture treatment to a patient with a tibial fracture fixated by Ilizarov. Enables the comparation between an acupuncture needle and a Kirschner wire.
View Figure 3
Table 6: Comparison between acupuncture and External fixation devices. View Table 6
Furthermore, the different effect of acupuncture and electroacupuncture (EA) should be taken in consideration [14].
Another difference to take in consideration is the fact that standard acupuncture treatment is performed by inserting needles in multi various locations in accordance with traditional acupuncture diagnosis, while in this study only one acupoint was stimulated. A method of acupuncture which stimulates only one acupoint (Single Needle Therapy, SNT) has been published in the literature [6-8,21-24], but it is clearly not the majority of clinical practices or studies. Having that said, Ceccherelli, et al. [25] examined the differences between 3, 5 and 11 needles treatment for painful cervical myofascial syndrome and found no clinically relevant differences among groups.
A further study, using a complementary full acupuncture in accordance with the ST36 stimulation by the wires may reveal new information.
This was a retrospective pilot study that examined a small sample of 33 patients. It is possible that performing an identical study with a larger patient sample could lead to clearer results, possibly with a higher P value. Furthermore, patients’ files were reviewed for only five days following surgery, with regard only to the acute postoperative phase. A longer follow up of the postoperative rehabilitation process could produce a more precise data.
In patients suffering from a tibial fracture treated with an EFD, locating an EFD wire in the anatomical similar site of acupoint St 36, did not lower patients pain levels or analgesic consumption.
According to the results of this study, stimulating the ST36 acupoint by inserting a wire does not have an analgesic effect.
Only on the 4 th day, the difference of the VAS score between the two groups was of statistical relevance. Upon researching literature, we did not find any specific effect four days following the acupuncture treatment. Therefore, we see it as a coincidental finding.
Statistical analysis was conducted by Basem Hijazi from Bar-Ilan University.
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
All authors made significant contributions to the conception, design, execution, or interpretation of the study.
The authors declare that there are no conflicts of interest.