Introduction: Synovial chondromatosis is a rare benign condition which involves synovial metaplasia and proliferation resulting in formation of multiple cartilaginous nodules in the synovium of the joints. Primary synovial chondromatosis is of unknown origin and presents between the age of 40 and 50 while secondary synovial chondromatosis is a result of degenerative change in the joint and presents later. Synovial chondromatosis usually presents in larger joints such as hips and knees. Presentation in smaller joints such as the ankle has also been reported.
Case summary: An 81-year-old female presented with a seven-year history of pain in her left ankle joint. She is a patient with known recurrent synovial chrondromatosis having had two excisional biopsies and synovectomy performed previously. After clinical and radiological assessment of her current presentation, a left subtalar fusion with excision of the cystic mass was performed. Histopathological study confirmed the findings of synovial chondromatosis with atypia.
Conclusion: Management of synovial chondromatosis involves complete excision of the lesion. In this patient who presented with recurrent ankle synovial chondromatosis, a subtalar arthrodesis was performed after excision with a hope that this would cause resolution of this condition.
Synovial chondromatosis is a rare benign condition that involves synovial lining of joints, synovial sheaths and bursae [1]. Metaplastic transformation occurs in the synovium and intra-articular cartilaginous nodules are formed [1]. These nodules detach and form loose bodies in the joint and may undergo secondary calcification [2]. Synovial chondromatosis mainly affects large joints with the hips and knees being more common while smaller joints are less frequently involved [3]. Synovial chondromatosis typically presents in the fourth to fifth decade of life [4] and patients generally present with pain, swelling and restriction of movements [5]. Management is mainly surgical which could either be open or arthroscopic [6]. The aim of this case report is to present a case of synovial chondromatosis in a female who had a subtalar fusion performed after excision of the lesion.
An 81-year-old female had ongoing pain in her left ankle for the past 7 years. It was initially thought to be an ankle sprain when she first presented and was managed non-operatively with analgesia and physiotherapy. She denies any trauma and has been able to weight bear and mobilise on her left leg. There was swelling in the medial aspect of the ankle and with repeated episodes of pain, a plain X-ray was performed. An ankle cyst was found and the patient underwent excision of this cyst. The excisional biopsy provided a diagnosis of synovial chondromatosis. The patient re-presented three years later with massive swelling, severe pain day and night, minimal mobility desperate for a solution. X-ray and MRI findings are seen below (Figure 1 and Figure 2).
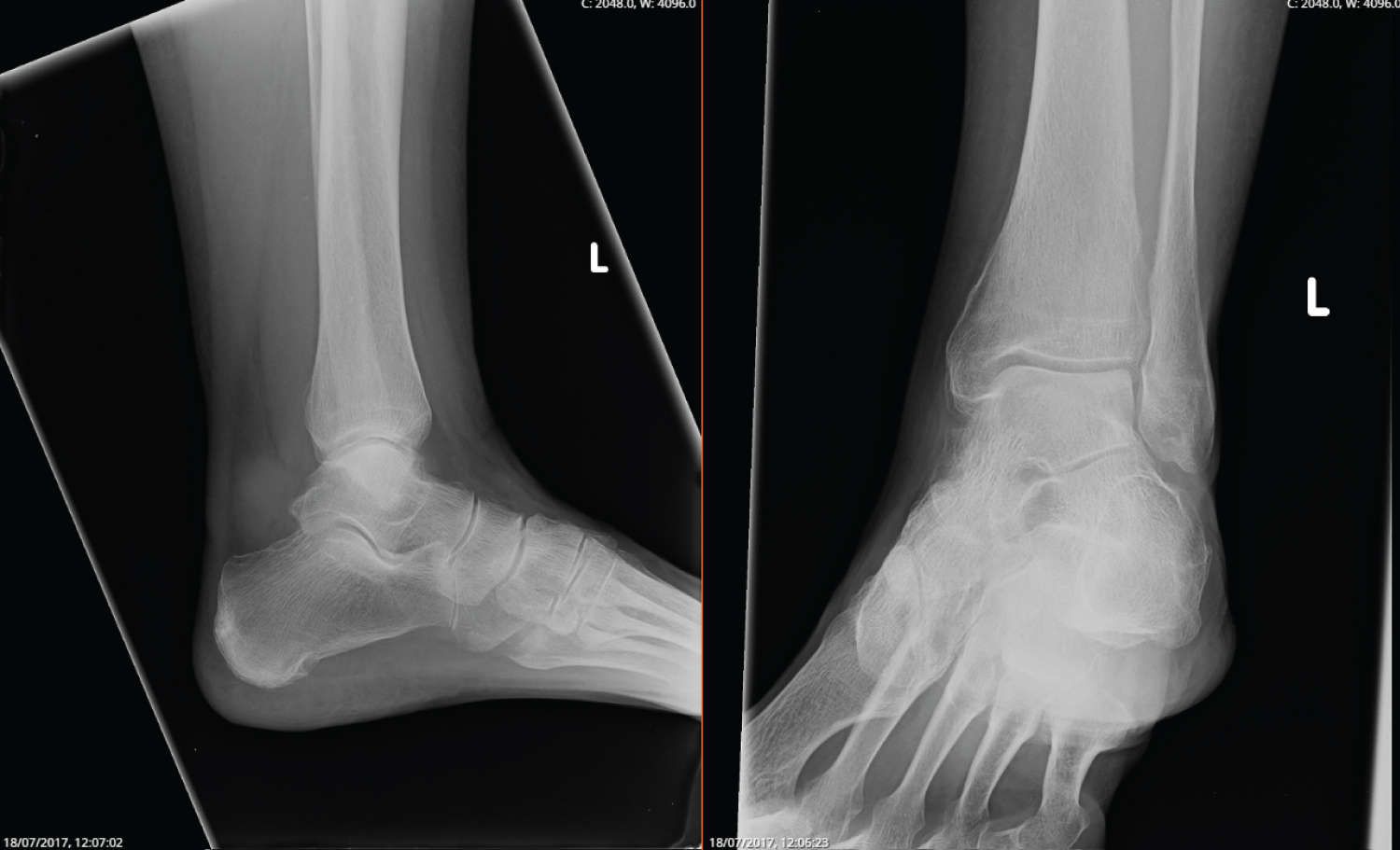 Figure 1: X-ray of the left ankle joint performed in 2017 showing edema and calcification of soft tissue. View Figure 1
Figure 1: X-ray of the left ankle joint performed in 2017 showing edema and calcification of soft tissue. View Figure 1
On examination, the patient's left ankle had reduced range of motion in flexion and extension as compared to the right. There was swelling of the left ankle with tenderness in the medial region with sural nerve paraesthesia on the lateral side of the foot. No other bony tenderness was present.
Surgical management was indicated in her case where an extensile lateral approach whilst visualizing the subtalar joint was utilised to excise the cystic mass. Two pieces of fibrous grey-white tissue 36 × 30 × 24 mm and 43 × 33 × 28 mm were removed during the procedure. Subtalar fusion was then performed with Acutrak headless compression screws (Figure 3a and Figure 3b).
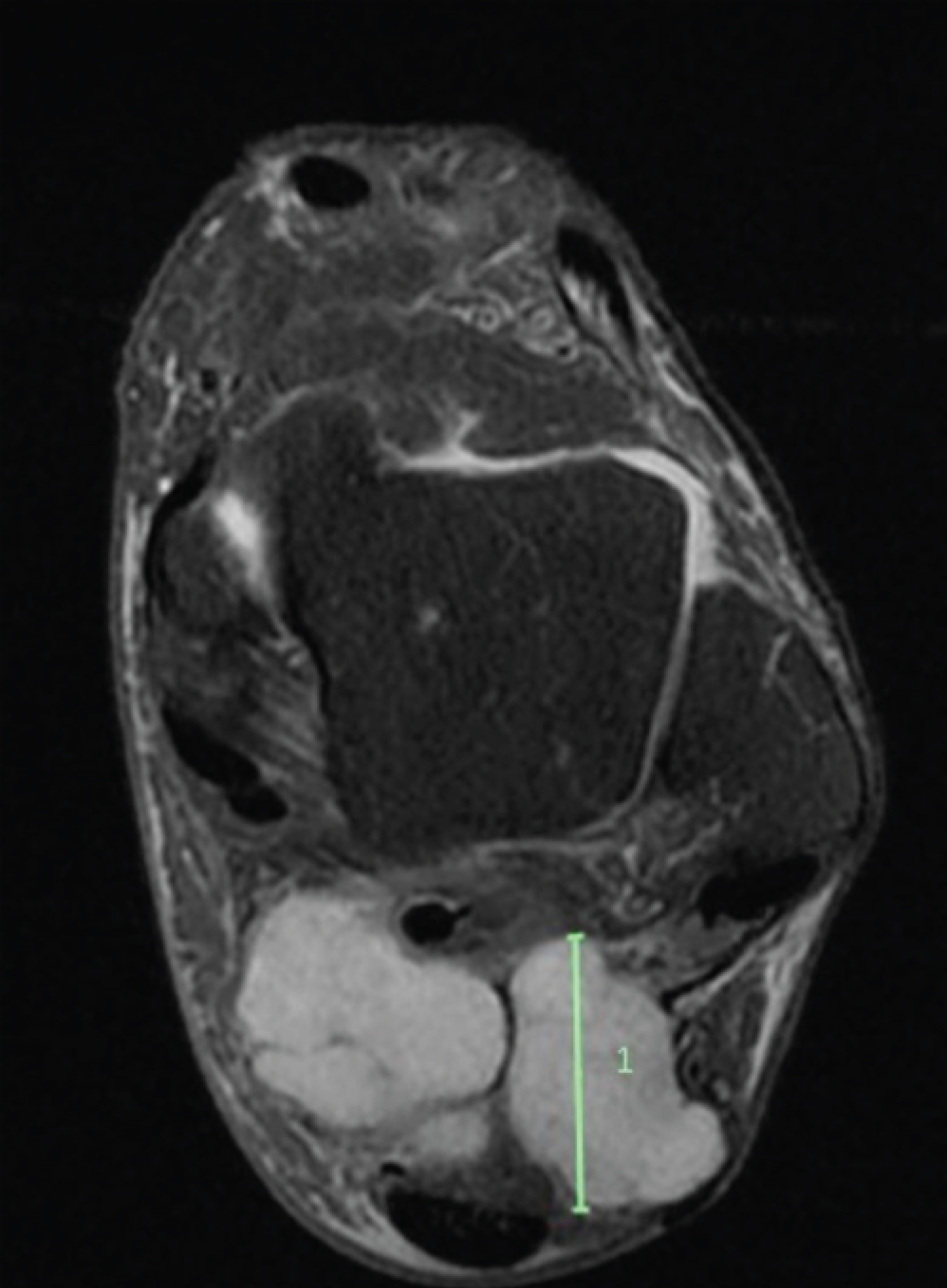 Figure 2: MRI performed in 2017 demonstrating the large cystic mass. View Figure 2
Figure 2: MRI performed in 2017 demonstrating the large cystic mass. View Figure 2
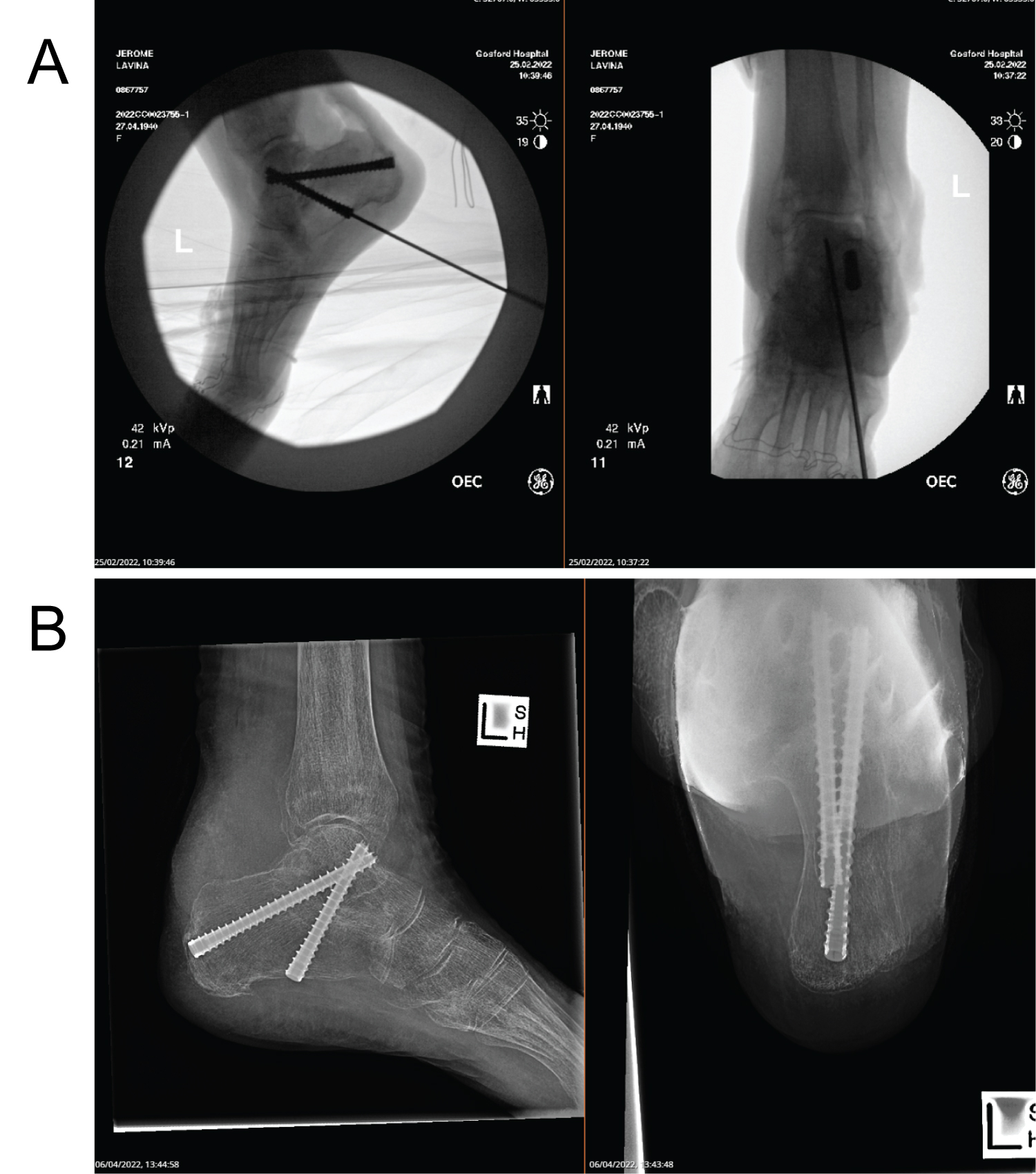 Figure 3: (a) Showing intraoperative insertion of Acutrak Screws; (b) Showing two Acutrak screws 7.5 mm each used for subtalar fusion post operation. View Figure 3
Figure 3: (a) Showing intraoperative insertion of Acutrak Screws; (b) Showing two Acutrak screws 7.5 mm each used for subtalar fusion post operation. View Figure 3
The excised tissues were sent for histo-pathological examination which found soft tissue chondroid lesions. Given her background of recurrent synovial chondromatosis, the histopathology report favoured the diagnosis of recurrent synovial chondromatosis with a large traumatic neuroma. Post-operatively the patient was placed in a short leg cast and was instructed not to weight bear on her left leg for 10 weeks. She was followed up at 2, 6 and 12 weeks.
Synovial chondromatosis is an uncommon metaplastic condition that involves cartilaginous bodies forming within the synovium and sub synovial connective tissues of large joints [1]. Milgram's study demonstrated 3 phases of disease process. Phase 1 involves metaplasia of synovium with active synovitis and absence of loose bodies. Phase 2 involves active synovitis with the formation of loose bodies, which are still cartilaginous. Phase 3 occurs when these loose bodies calcify and the synovitis subsides [7]. Imaging modalities such as X-ray, CT and MRI can be used in diagnosing this condition.
Surgery is considered the treatment of choice. Both open and arthroscopic procedures can be used to treat this condition [6]. The procedure is targeted towards removing loose bodies and to improve pain and function [8]. Total synovectomy is preferred over removing loose bodies alone as it has shown to reduce the chances of recurrence [9]. Recurrence rates after total synovectomy have been demonstrated by various reports to range from 3-23% [10-12], with another study reporting a higher rate of recurrence in the patients they followed up of up to 37.5% [13].
The patient in this case report had a total synovectomy and excision of the lesion performed. She had multiple presentations affecting her daily function despite having two prior excisions done. Therefore, it was discussed that to further reduce the chances of recurrence, a subtalar arthrodesis should be performed as well.
Complete excision of the lesion is the standard treatment for synovial chondromatosis, however arthrodesis seems to be the definitive treatment for recurrent synovial chondromatosis [14]. One case report showed a similar treatment strategy where after removal of all loose bodies, a subtalar arthrodesis was done. At the follow up after a year, the patient was pain free with a full range of motion and did not experience any recurrence [15].
The current presentation represents the third recurrence for the patient, where she complains of severe pain and loss of function when compared to her previous episodes so much so that she was willing to opt for surgical management. It was thought that a simple excision of the lesion would not suffice considering she still had recurrences despite two prior excisions. The main reasons for recurrence include incomplete removal of the synovium and loose bodies [16]. Therefore it was discussed that by performing an arthrodesis, the chondral surface and movement are removed and the synovium atrophies eventually disappear which no longer predisposes the patient to further disease progression. The patient suffered arthritis in her subtalar joint as well, likely degenerative associated with the recurrent synovial chondromatosis.Hence, the arthrodesis was performed to manage the arthritis as well [17].
To our knowledge, arthrodesis for the management of recurrent synovial chondromatosis in the subtalar joint has been rarely reported [15]. The patient has been followed up regularly, with no recurrence and great improvement in mobility and pain.
A case of synovial chondromatosis is described here which was treated with excision of the cyst with the addition of a subtalar arthrodesis. For patients with recurrent ankle synovial chondromatosis despite multiple excisions, fusion of the joint can be considered as a treatment option to prevent further recurrences.