The plantar fascia is an important structure in the foot, which helps, stabilizes the arch of the foot during motion and provides shock absorption when the foot hits the ground. Inflammation of the plantar fascia has been high in incidence, with multiple factors attributed to it. However, occurrence of the plantar fascia rupturing is not common. Corticosteroid injection to the plantar fascia has long been advocated as the major cause of this. Nonetheless, in recent literatures, corticosteroid injections have been shown to be safe and provide good results in treating pathologies of the plantar fascia [1]. There has been reports of high incidence of plantar fascia in active athletes [2, 3]. Chronic plantar fasciitis can also weaken the plantar fascia and eventually lead to its rupture. Early identification of this is necessary as the treatment protocol is different and more stringent.
A 37-year-old male medical practitioner, presented with acute pain to his right foot associated with swelling and a limp. He is an active athlete and his complains started while he was playing futsal (indoor football). While running, he suddenly felt a "pop" on his plantar aspect of his foot, and severe pain following it. He was not able to continue with the game and had great difficulty weight bearing on it. A few hours later he noticed his foot had become considerably swollen as compared to the left. On further questioning, he informed that he had been diagnosed with bilateral plantar fasciitis since 5 years ago and had history of multiple corticosteroid injections, the latest being 4 weeks prior to the injury to the same foot. This time around he returned to active sports 2 weeks after the injection.
Upon examining the patient, there was a diffuse swelling over the medial side of the plantar aspect of the affected foot (Figure 1). The medial arch also seemed to be loss with minimal bruising over the affected part. There was severe tenderness along the plantar fascia, mainly on the medial side of the foot and at its insertion over the calcanuem. Passive extension of the toes causes severe pain and he was not able to tip toe on the affected foot. At this time, it was highly suspicious that patient might have a rupture plantar fascia, hence was preceded with ultrasonography of the foot, which demonstrated a ruptured plantar fascia (Figure 2).
 Figure 1: swelling and minimal echymoses around the plantar aspect of the midfoot with loss of the medial arch. View Figure 1
Figure 1: swelling and minimal echymoses around the plantar aspect of the midfoot with loss of the medial arch. View Figure 1
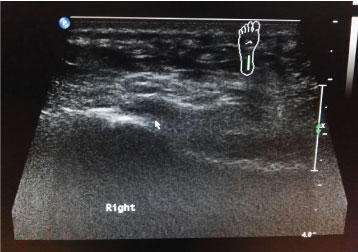 Figure 2: Longitudinal sonogram image of a 37-year-old man showing grossly thickened plantar fascia with hypoechoeic changes within suggestive of partial tear. View Figure 2
Figure 2: Longitudinal sonogram image of a 37-year-old man showing grossly thickened plantar fascia with hypoechoeic changes within suggestive of partial tear. View Figure 2
Patient had initially applied cold compression to the foot overnight following the injury. Following the confirmation of the diagnosis, the foot was immobilized with an above ankle boot cast with a medial arch support. Patient was not allowed weight bearing for 2 weeks and given anti-inflammatory for the whole period. At the end of 2 weeks he was treated with platelet rich plasma injection to the affected plantar fascia and was allowed partial weight bearing during this time. Stretching exercises and physical therapy were started concurrently. Exactly 1 month after the injury, patient was able to carry out activities of daily living without pain and return to active sports 8 weeks after the injury.
Plantar fasciitis has long been discussed as one of the most common foot pathology over the plantar aspect of the foot. Due to the repetitive stress to the fascia, it will eventually weakened it and lead to a rupture. First described by Leach, et al. in 1978, plantar fascia rupture is not common, and due the difficulty in diagnosing it has lead to the possible infrequency of this condition [4,5]. Incidence of acute rupture is not common. It's prevalence is commonly attributed to be an acute-on chronic injury, most commonly due to chronicity of plantar fasciitis and repetitive stress to the plantar fascia being the main contributing factor. Pai also reported spontaneous rupture due to degeneration of the plantar fascia occurring in an elderly [5]. Other risk factors that might contribute to a rupture are obesity, the degree of activity (standing at work for long periods of time), flat feet, decreased dorsiflexion of the ankle joint, and calcaneal spurs, in which some of it fits the patient.
The use of corticosteroid injection for the treatment of plantar fasciitis has been well documented to produce good results. However, it has always been widely known that corticosteroids injection will lead to rupture of the plantar fascia. Initial studies by Leach supported this [4]. Sellman then reported on 37 patients who had ruptures, all had history of previous corticosteroid injection [6]. On the other hand, recent literatures have provided extensive data into the safety of using corticosteroid in the treatment of plantar fasciitis. Kim, et al. reported out of 120 patients treated for plantar fasciitis, an average of 2.1 injections were given, with an interval of 3.7 months in between injections for a period of 2 years [1]. Out of the 257 injections given, only 3 were reported to have a plantar fascia rupture. In another retrospective analysis of 192 patients treated with corticosteroid injection, Kuwada reported no rupture occurred in them [3]. In that study, there were even 8 patients who received 8-10 injections with no plantar fascia rupture or tear, a similarity to our patient who had at least 5 injections to his foot.
Athletes, especially runners with plantar fasciitis are advised to totally avoid using corticosteroid injection as a mode of treatment [7]. The corticosteroid injection alone is not the culprit causing the patient's plantar fascia to rupture. However, the injection together with the early return to sporting activities soon after might have been the main reason why the incident happened to our patient. Both the steroid injection and the early return to sports, leads to an excessive overloading to an already weakened structure, ultimately resulting in the plantar fascia rupturing [3]. It is probably best to withhold resuming sporting activities for at least 3-4 weeks
Sonography is an important non-invasive diagnostic imaging modality for assessment of tendon and foot conditions, in particular the plantar aponeurosis. It is usually well tolerated by patients, cost-effective and provides good spatial resolution in superficial structures [1]. In normal healthy subjects, it appears as a homogenous echogenic band with internal linear interfaces or fibrillary pattern on longitudinal scans. In an inflamed and partially ruptured plantar fascia such in our case, the fascia will appear thickened, hypoechoeic with loss of the internal fibrillary pattern (Figure 2, X). Apart from sonography, MRI is proven as a standard imaging technique that is sensitive to diagnose pathological changes in a plantar fascia [8]. MRI also is excellent to rule our other differential diagnosis of subcalcaneal heel pain.
Treatment of plantar rupture has to be stricter and more protocol like [2]. Initial period of immobilization and no weight bearing has been advocated in multiple studies to produce good results. Initial ice application and NSAIDs will help reduce the inflammation from the acute rupture. Combination of a short leg boot cast with strict non-weight bearing crutches, immobilizes the foot and ankle helps in allowing the injured tissue to heal. Injecting the plantar fascia with plasma rich protein (PRP), accelerates the healing process as well. Although, relatively new in the treatment of plantar fasciitis, there are numerous literatures supporting the use of PRP in treating tendinoplathies. PRP is also safe and well tolerated by patients as reported by Wilson, et al. [9]. Surgical removal of the fibrotic tissue of the ruptured plantar fascia should be reserved as a last resort and only if previous conservative management of the ruptured plantar fascia fails.