Introduction: It has been shown in the literature that ankle fractures account for about 10% to 15% of all fractures, and that about 20% of all ankle fractures will require an internal fixation determined directly by a syndesmosis injury. Reported complications range from 1% to 36.5%, including short-term soft tissue infections. It has also been shown that the application of calcium sulfate beads added with antibiotics as a local method in the bone reduces the risk of infection and biofilm formation in this inaccessible area, since it fills spaces and helps in the treatment of localized and deep infections.
Clinical case: Present clinical case of a patient treated in the Division of Orthopedics and Traumatology of the Clinical Hospital ISSSTE Susulá. 59-year-old woman with a history of type 2 diabetes mellitus and systemic arterial hypertension with poor adherence to medical treatment, diabetic retinopathy and tako-tsubo syndrome, begins her condition suffering a forced inversion of the left ankle, which causes pain, deformity, increased volume at the ankle level, as well as ecchymosis in the medial malleolus with inability to walk, is medically evaluated by the traumatology and orthopedic service, where it is diagnosed with anterolateral dislocation of left ankle and ipsilateral trimaleolar ankle fracture, it is admitted to the service where open reduction and internal fixation is performed, After hospital discharge the patient is diagnosed with infection of the surgical wound and treated with calcium sulfate beads adding antibiotic resulting in improved symptoms and control of infection.
Discussion: The application of calcium sulfate beads medicated with antibiotic as a local method to bone has been shown to reduce the risk of infection and biofilm formation in this inaccessible area, since it is used to fill dead spaces and help in the treatment of localized and deep infections, Likewise, there is no deterioration of osteosynthesis material when pearls are placed when dissolved at 6 weeks, being an absorbable material has an advantage over other components that are required from its extraction.
Ankle fracture, Calcium sulfate beads monohydrated, Bone infection, Adjuvant in bone infections, Fracture complication
It has been shown in the literature that ankle fractures represent about 10% to 15% of all fractures [1-3] and that about 20% of all fractures will require an internal fixation determined directly by a syndesmosis injury, It is also the area with the highest incidence of fractures of the lower extremity with around 19.2% [4]. Similarly, reported complications range from 1% to 36.5%, including short-term soft tissue infections, wound healing complications and thrombotic events, as well as long-term complications such as avascular necrosis, defective consolidation, arthritis, pseudoarthrosis, chronic pain and instability [4].
Diabetes mellitus, advanced age and female sex have been identified as some of the main predictors of complications [1,3].
Infection in the surgical wound by ankle fracture is frequent ranging from 1.3% to 14%, and its incidence increases considerably in exposed fractures.
The main responsible microorganism described in the literature is Staphylococcus aureus [4].
Report a case of surgical wound infection treated with antibiotic-carrying calcium sulfate beads in a patient with ankle fracture treated for osteosynthesis.
59-year-old female age as a history of diabetes mellitus type 2 of 14 years of evolution in treatment with insulin and metformin, diabetic retinopathy of 4 years of evolution, systemic arterial hypertension of 30 years of evolution in treatment with valsartan, amlodipine and metoprolol, diagnosed with cardiac arrhythmia and tako-tsubo syndrome of 6 years evolution in treatment with acetylsalicylic acid and amiodarone, depression treated with fluoxetine of 10 years evolution, the patient suffers a forced reversal of the left ankle when stepping on an object on the floor, which causes pain, increased volume at the ankle level, as well as ecchymosis in the medial malleolus with inability to walk, is admitted to the emergency department and evaluated by the traumatology and orthopedics department, finding it conscious, oriented, cardiopulmonary system without compromise, abdomen without compromise, left lower extremity with edema +++/+ at ankle level, with evident medial deformity resulting in varus, medial and lateral ecchymosis, inability to support and walk, neurovascularly without alterations. Initial extension radiological studies were taken, with anteroposterior, lateral and oblique projections (with 10° internal rotation) of both ankles, showing lateral dislocation of the left ankle and ipsilateral trimaleolar ankle fracture with a posterior malleolus lesion surface of approximately 35% (images in Figure 1A and Figure 1B), under informed consent letter, the reduction of urgent luxation is performed in the emergency area by placing robert-jones boot type anti-edema dressing, as well as double splint, in "U" and "Posterior" with significant improvement in pain referred by the patient after reduction, it is admitted to the orthopedic and traumatology service of our unit, where it is performed 3 days after open reduction and internal fixation with a plate of "1/3 tube" 6 for lateral malleolus with 6 bicortical screws, two partial threaded screws in medial malleolus, 3 holes "1/3 tube" plate with 2 screws for the posterior malleolus, as well as positioning screw for the stability of tricortical synadesmosis (Figure 1C, Figure 1D and Figure 1E), with adequate postoperative evolution to be downloaded one day after the intervention with analgesic, anti-inflammatory and antibiotic treatment, and is scheduled after 2 weeks to check the wound and 6 weeks later to remove the situational screw, the patient goes to the emergency room up to 6 weeks later with left ankle volume increase, increased temperature and localized erythema in the ankle, as well as an average injury of approximately 7 × 3 cm in length with edges without vitality and exposure of subcutaneous and bone tissue, 10 cm long lateral wound with outflow of purulent diverted tissue material and exposure of osteosynthesis material (Figure 2A and Figure 2B), Control laboratories and wound cultures are requested and growth in Staphylococcus aureus cultures is reported, he is diagnosed with surgical wound infection, as well as osteomyelitis of the left ankle and is admitted for antibiotic and surgical treatment.
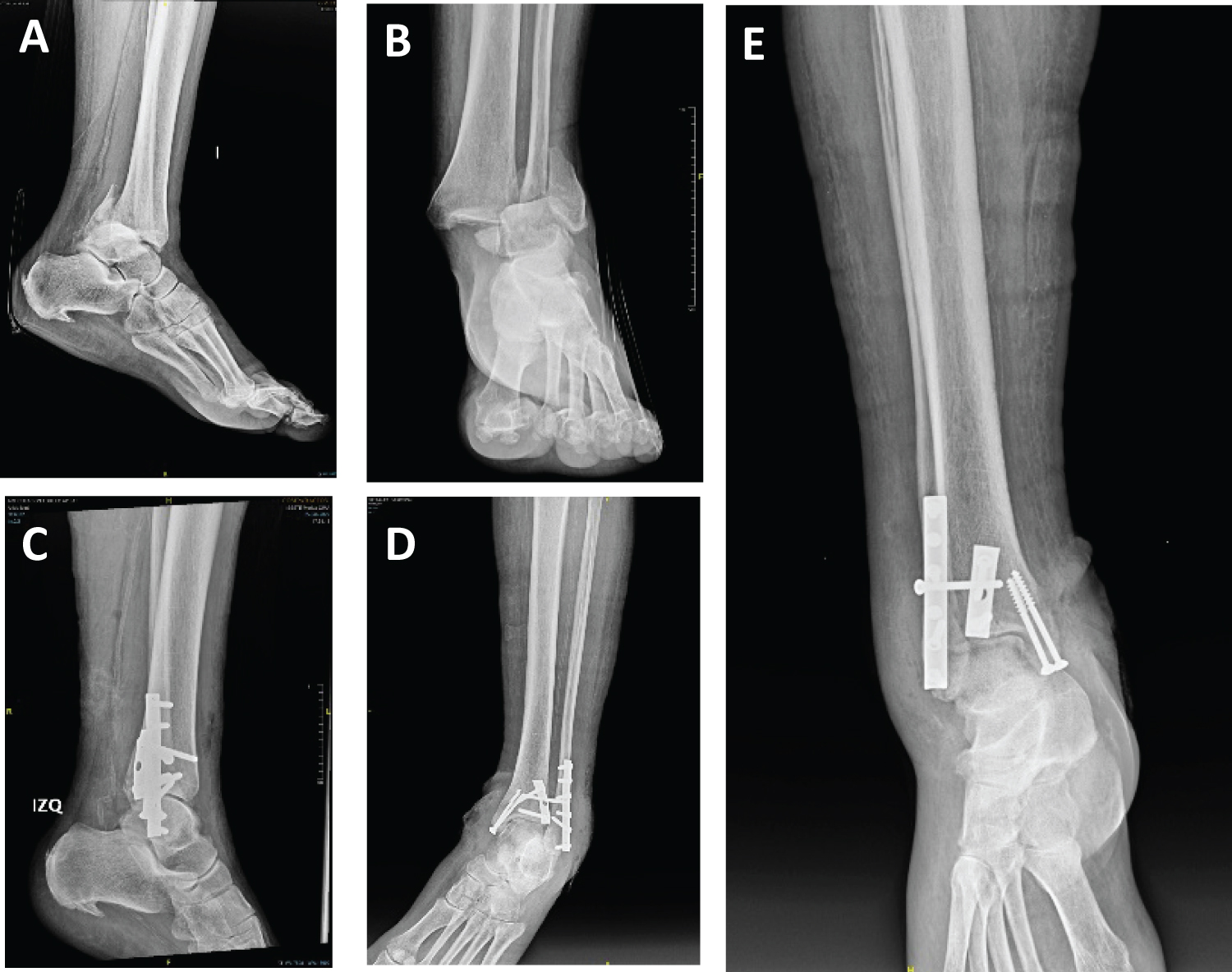 Figure 1: (A and B) Lateral and AP x-ray of the ankle showing anterolateral dislocation and Weber trimalleolar fracture C; (C, D and E) Lateral radiographs, 10° external rotation and AP of the ankle respectively where postsurgical reduction is observed using osteosynthesis material.
View Figure 1
Figure 1: (A and B) Lateral and AP x-ray of the ankle showing anterolateral dislocation and Weber trimalleolar fracture C; (C, D and E) Lateral radiographs, 10° external rotation and AP of the ankle respectively where postsurgical reduction is observed using osteosynthesis material.
View Figure 1
 Figure 2: (A/B) Clinical photos at admission, wound in dehiscent lateral malleolus with exposure of osteosynthesis material (A), devitalized tissue and dehiscent wound in medial malleolus; (C/D) Transoperative images of surgical cleaning, long peroneal tendon (C), surgical cleaning in medial malleolus (D); (E/F) Intralesional calcium sulfate beads are observed in the lateral and medial malleolus respectively; (G/H) Current clinical photos without infection data with healed wounds.
View Figure 2
Figure 2: (A/B) Clinical photos at admission, wound in dehiscent lateral malleolus with exposure of osteosynthesis material (A), devitalized tissue and dehiscent wound in medial malleolus; (C/D) Transoperative images of surgical cleaning, long peroneal tendon (C), surgical cleaning in medial malleolus (D); (E/F) Intralesional calcium sulfate beads are observed in the lateral and medial malleolus respectively; (G/H) Current clinical photos without infection data with healed wounds.
View Figure 2
For the approach of the patient was placed in supine decubitus, lateral opening of the scar area was performed and osteosynthetic material was extracted from the lateral malleolus, medial and posterior, a sample is taken and sent to pathology and the wounds are treated with excellent resistance and debridement until healthy tissue is observed (images in Figure 2C and Figure 2D), and the wound is irrigated with saline solution. The remaining wound is approximately 7 × 5 cm in the lateral malleolus and 10 × 7 in the middle malleolus, both with deep tissue exposure, begins a double antibiotic scheme according to the results of the cultures found as Staphylococcus aureus agent, with vancomycin plus tigercicline and wound cleaning every 48 hours. Joint management with the internal medicine service is requested for the control of blood glucose and the second surgical examination is performed 7 days after the first scarification, highlighting and eliminating the devitalized tissue, by taking part of the posterior tibial tendon for the culture sample, transoperationally added calcium sulfate beads with gentamicin and vancomycin ( Stimulan ) are requested and placed, the presence of purulent material during the procedure is not observed; gauze is placed and the limb is bandaged without closing the wound, it is re-treated for the third time with new surgical cleaning and scarification of the wound without evidence of the presence of purulent material, due to the quality of the tibial astragalin joint, it is removed and an external fixative is placed in a delta position on the medial face (Figure 3A and Figure 3B), calcium sulfate beads added with gentamycin and vancomycin (Stimulan) are placed again (Figure 2E and Figure 2F) and new culture samples are taken and negative 48 hours later, a decrease in acute phase reagents is observed until their negativization, with delayed closure of the wound by second intention, the negative pressure system is placed, after 4 months the closure of the wound is observed (Figure 2G and Figure 2H), as well as pseudoarthrosis data in the control plates (Figure 3C and Figure 3D), so the external fixative is removed.
 Figure 3: (A and B) AP and lateral ankle radiography showing reduction with external fixative sub-astragalin osteotomy and distal fibula, calcium sulfate beads placed transquirurgically. X-rays of PA and lateral (C and D) ankle, showing residual osteoarthritis subastragaline with resolved infectious process.
View Figure 3
Figure 3: (A and B) AP and lateral ankle radiography showing reduction with external fixative sub-astragalin osteotomy and distal fibula, calcium sulfate beads placed transquirurgically. X-rays of PA and lateral (C and D) ankle, showing residual osteoarthritis subastragaline with resolved infectious process.
View Figure 3
Ankle fractures are the most frequent result of one of the following four mechanisms, supination with external rotation in 45% to 75% of cases according to Lauge-Hansen, pronation with external rotation in 7% to 19%, pronation with abduction in 5% to 21% and supination with adduction of 10% to 20%, the classification of Denis-Weber has been taken as a reference that tells us at what height the fracture is with respect to distal tibiofibular syndesmosis, the most appropriate treatment and prognosis of them, dividing them into Weber A Infrasyndesmal, Weber B transyndesmal and Weber C suprasyndesmal, complications in ankle fractures that are associated with osteosynthesis material have been reported at advanced age (65 years) hypoproteinemia, peripheral neuropathy, open fracture, diabetic patients and low level of experience by the surgeon [3].
Diabetic patients generally have more postoperative complications than non-diabetics, unplanned secondary surgeries (including exceresis and debridement, arthrodesis and amputation) and poorer motor function [3].
The most frequently associated acute complication is infection of the surgical wound, which may decrease if the underlying disease is controlled, Also the treatment of bone infections and wounds where osteosynthesis material was used is modified by the result of cultures being the most frequently isolated etiological agent Staphylococcus aureus .
The application of calcium sulfate beads medicated with antibiotic as a local method to bone has been shown to reduce the risk of infection and biofilm formation in this inaccessible area, as it is used to fill dead spaces and assist in the treatment of localized and deep infections, Similarly there is no deterioration of osteosynthesis material when pearls are placed when dissolved at 6 weeks, being an absorbable material has an advantage over other components that are required from its extraction [5-9].
It is prepared with a mixture of calcium sulfate and antibiotic solution, all transopertoriamente, once formed the pearls are placed in the place that is agreed, Local antibiotic release has been evaluated as systematic in a Turner study found that tobramycin was undetectable in serum at 24 hours, but remained constant until 28 days locally [6- 11].
Currently our patient successfully fulfils the objective of initial treatment by achieving infection control and limb preservation.
None.
None.