Introduction: Epidemiological studies suggest that proximal humerus fractures are very common, representing 4-10% of all fractures. This proportion is increased when surgical intervention cases are examined, as approximately 30% of proximal humerus fractures are treated surgically.
Clinical case: 38-year-old male, who was admitted for severe pain and functional limitation of his left shoulder. No background of importance to the case. He suffered a car accident while driving his motorcycle, lost his balance and fell, suffering a direct impact on his left shoulder, causing pain, edema and functional limitation. Upon arrival, he was conscious, oriented, cooperative, calm, cardiopulmonary system without compromise, abdomen without compromise, left upper extremity with presence of edema +/+++ in the shoulder, ecchymosis, incomplete range of motion. Crepitus are palpable at the time of examination, without distal neurovascular compromise.
Discussion: The autogenous fibula is a source of bone grafts for the treatment of bone defects. Its advantages include easy access, absence of immune rejection, and considerable strength. However, its disadvantages include the requirement of an additional surgical incision, postoperative pain in the harvested bone area, and the risks of bleeding, infection, and nerve injury. Using structural bone grafts comprising autogenous fibula for the treatment of severe proximal humeral comminuted fractures can re-establish medial support of the proximal humerus and increase fixation strength. Fibular allograft and shoulder arthroplasty are also effective treatments for proximal humerus comminuted fractures among elderly individuals. However, these procedures cannot be performed in all regions. Compared to the aforementioned treatments, the use of the autologous fibular segment is more convenient and less expensive.
Proximal humeral fractures, Fibular segment, Structural bone grafting, Fibular autograft, Bone graft
Epidemiological studies suggest that proximal humerus fractures are very common, representing 4-10% of all fractures. This proportion is increased when surgical intervention cases are examined, as approximately 30% of proximal humerus fractures are treated surgically. As the population ages, the incidence of proximal humerus may continue to rise and the need for surgical treatment may gradually increase. As such, appropriate treatment strategies are essential to reduce the risk of poor prognosis and loss of self-care ability in these populations. The use of the locking plate technique for treating proximal humerus fractures has gained traction, but postoperative adverse outcomes and complications remain common. These include varus displacement, screw cut-out, and avascular necrosis of the humeral head. Intramedullary nailing, compared with eccentric fixation of plates, has the intrinsic advantage of resisting varus and rotational stresses and is theoretically more favorable for maintaining fracture reduction, especially when varus deformity is present. However, this technique is still associated with some complications such as iatrogenic rotator cuff injury and nonunion of the fracture. There are many studies about proximal humerus plate or nail treatment, but few have tested which internal fixation method is better for varus or valgus fractures [1-3].
38-year-old male, who was admitted for severe pain and functional limitation of his left shoulder. No background of importance to the case. He suffered a car accident while driving his motorcycle, lost his balance and fell, suffering a direct impact on his left shoulder, causing pain, edema and functional limitation. Upon arrival, he was conscious, oriented, cooperative, calm, cardiopulmonary system without compromise, abdomen without compromise, left upper extremity with presence of edema +/+++ in the shoulder, ecchymosis, incomplete range of motion, crepitus are palpable at the time of examination, without distal neurovascular compromise.
Radiographic and tomographic studies are performed on the left shoulder where soft tissue edema is observed, bone disruption at the level of the humeral head in the surgical neck area, as well as disruption and displacement of the greater and lesser tuberosity, varus angulation and posteromedial impaction. It is diagnosed as a fracture of the left proximal humerus Neer type IV/AO11b1.1 (Figure 1 and Figure 2).
 Figure 1: True anteroposterior radiograph of the left shoulder showing bone disruption of the surgical neck, greater and lesser tuberosity.
View Figure 1
Figure 1: True anteroposterior radiograph of the left shoulder showing bone disruption of the surgical neck, greater and lesser tuberosity.
View Figure 1
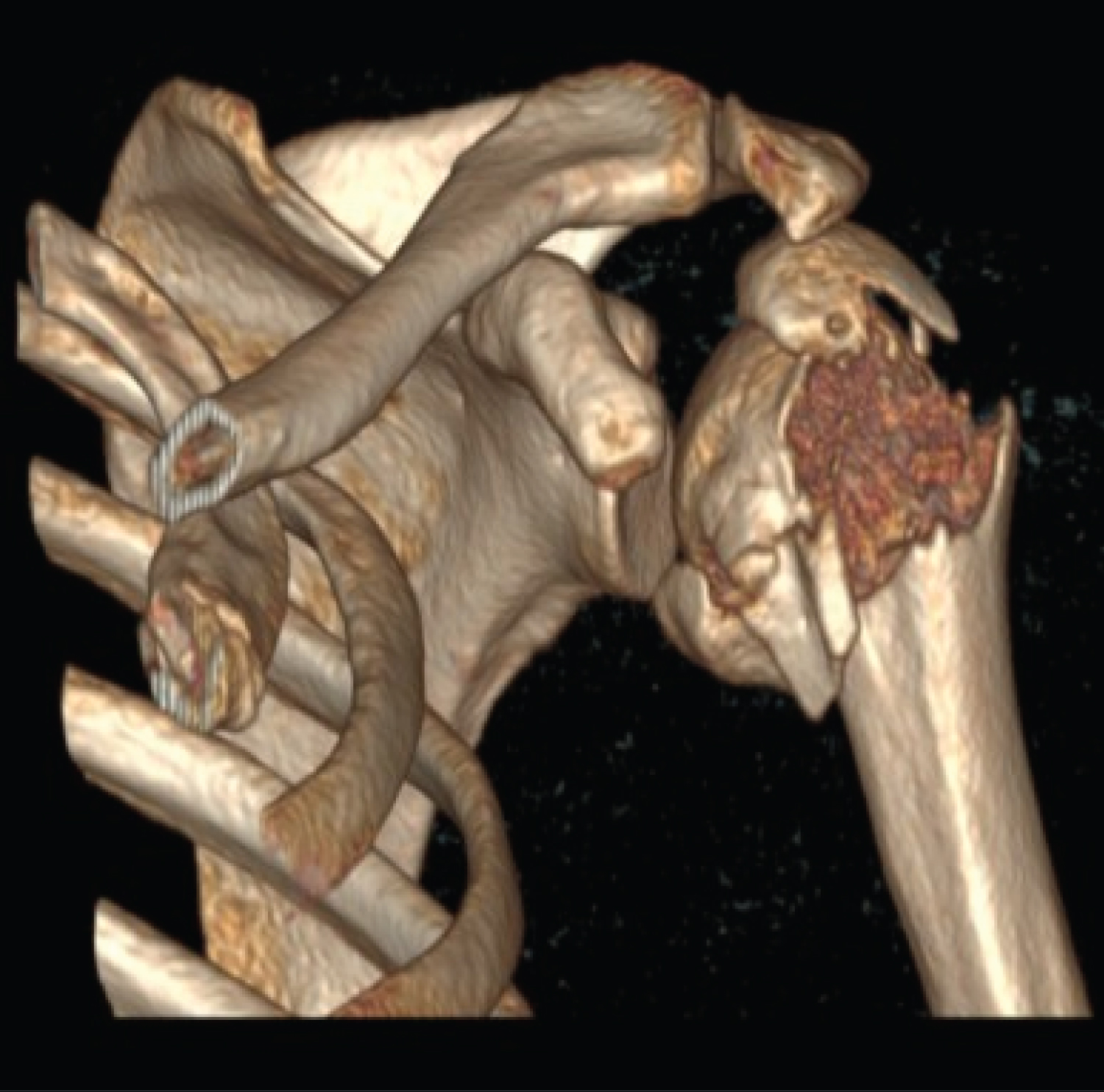 Figure 2: 3D reconstruction of the left shoulder where bone disruption and displacement of the surgical neck, greater and lesser tuberosity is observed, with posteriomedial impaction.
View Figure 2
Figure 2: 3D reconstruction of the left shoulder where bone disruption and displacement of the surgical neck, greater and lesser tuberosity is observed, with posteriomedial impaction.
View Figure 2
The procedure is performed with the patient in a supine position. A deltopectoral approach is performed with prior marking of anatomical references (from the coracoid process to the humeral shaft). An incision is made dissecting subcutaneous cellular tissue, the deltopectoral groove is dissected, the cephalic vein is observed and protected laterally, the joint capsule is reached, which is incised, the tendons of the rotator cuff are referenced, which later are manipulated to achieve the reduction of the fracture. A fibula graft is placed intramedullary and the fracture is reduced and osteosynthesis material is placed (Figure 3 and Figure 4).
 Figure 3: Transsurgical images showing approximately 6cm of fibula graft.
View Figure 3
Figure 3: Transsurgical images showing approximately 6cm of fibula graft.
View Figure 3
 Figure 4: The medullary canal is exposed to place the allograft.
View Figure 4
Figure 4: The medullary canal is exposed to place the allograft.
View Figure 4
To retrieved the fibula graft, a lateral approach to the fibula is performed, approximately at the middle third level, 13 cm from the tibio-talar joint. Subcutaneous cellular tissue is dissected and the posterior region of the peroneal fascia is approached and bone tissue is reached. Then approximately 6 cm long of bone shaft is taken.
The osteosynthesis material used was a 4-hole proximal humeral internal locking system plate, locking screws and 1.6 mm Kirschner pins for temporary reduction (Figure 5 and Figure 6).
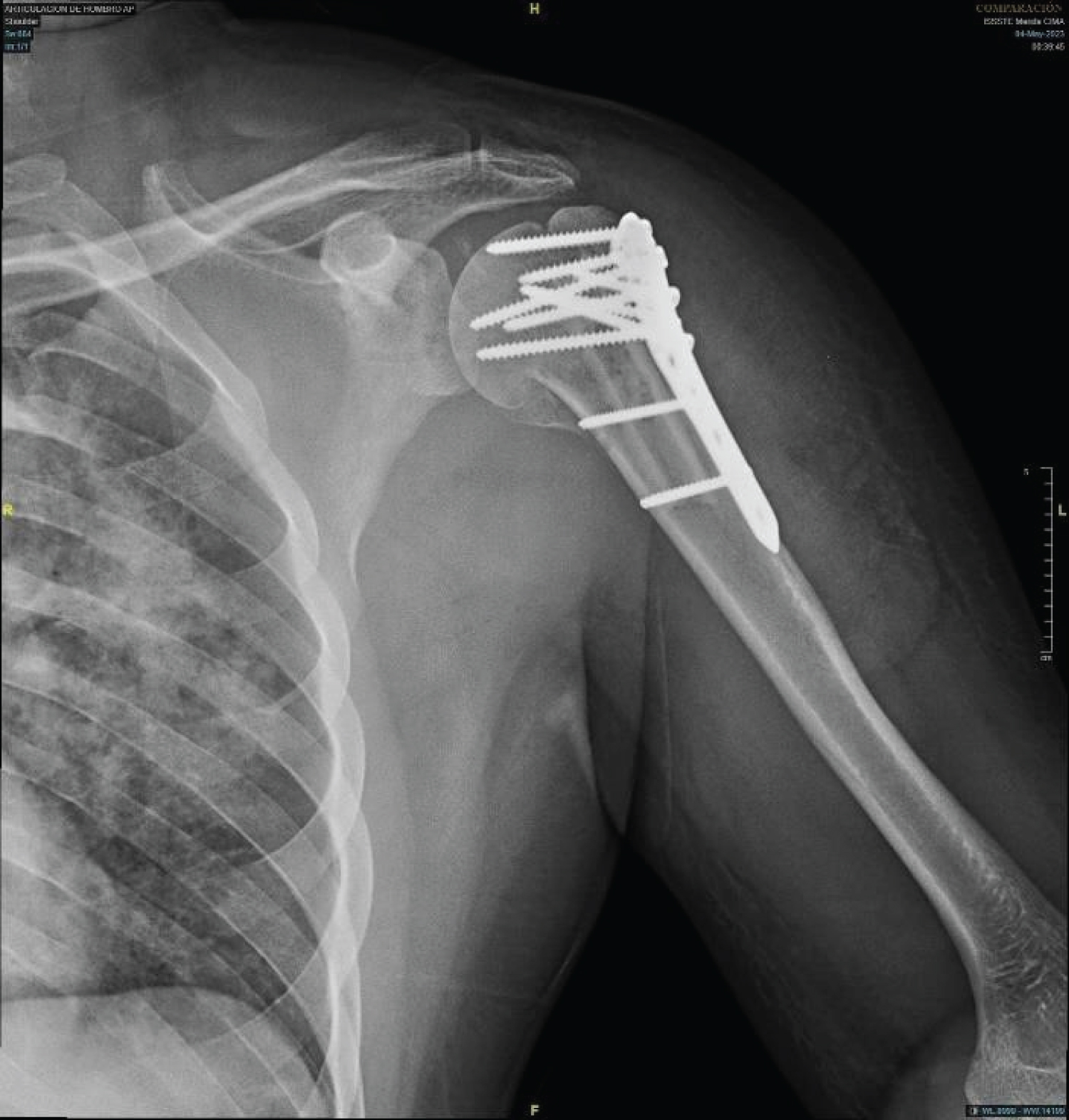 Figure 5: Immediate post-surgical radiographs showing reduction of the fracture and placement of osteosynthesis material and fibula autograft.
View Figure 5
Figure 5: Immediate post-surgical radiographs showing reduction of the fracture and placement of osteosynthesis material and fibula autograft.
View Figure 5
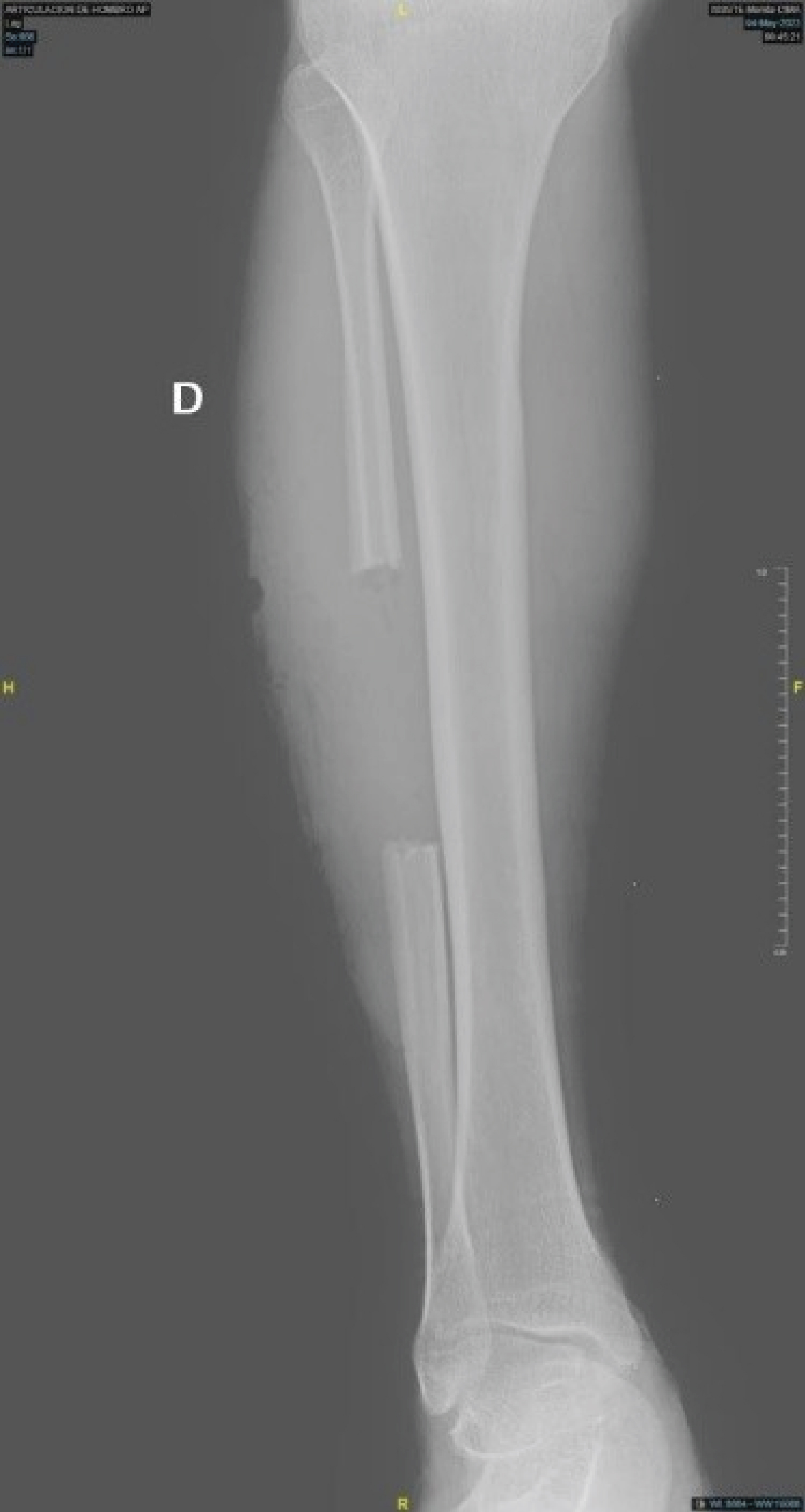 Figure 6: Anteroposterior radiograph of the right leg showing the area where the fibula graft was taken.
View Figure 6
Figure 6: Anteroposterior radiograph of the right leg showing the area where the fibula graft was taken.
View Figure 6
During his post-surgical follow-up at 3 months, he was observed to have adequate and functional ranges of motion, without limitations, without pain on mobility, adequate muscle strength with a Daniels scale of 5/5, and no distal neurovascular compromise. We evaluated the patient with the DASH (Disability of the arm, shoulder and hand) score, with a result of 3.3/100 which is related to excellent outcomes.
Proximal humeral fractures are likely to occur during high energy or low-energy trauma, such as falling from a standing height, among patients older than 50 years of age. Good reduction and stable fixation are difficult to achieve with severe proximal humeral comminuted fractures, and this difficulty results in negative effects on the normal rehabilitation of patients and leads to the loss of shoulder function.
In 1970, Neer proposed a four-part classification for proximal humeral fractures that is the most commonly used tool for classifying proximal humeral fractures in clinical settings. Most physicians prefer open reduction and internal fixation for Neer type III and type IV fractures with severe comminution. Most internal fixation materials are proximal humeral locking plates or proximal humeral intramedullary nails. According to recent studies, locking plates are widely used and recommended for the treatment of limb fractures. Furthermore, locking plate fixation is the most widely used technique for the treatment of proximal humeral fractures. However, 30% of reoperations are attributable to fixation failure, a vascular necrosis of the humeral head, and postoperative infections. These complications are caused by the lack of appropriate medial column structural support. Medial calcar comminuted fractures are often accompanied by the loss of medial support, which is an important factor that leads to internal fixation failure.
However, appropriate treatment for comminuted fractures has not been identified.
The autogenous fibula is a source of bone grafts for the treatment of boned effects. Its advantages include easy access, absence of immune rejection, and considerable strength. However, its disadvantages include the requirement of an additional surgical incision, postoperative pain in the harvested bone area, and the risks of bleeding, infection, and nerve injury. Using structural bone grafts comprising autogenous fibula for the treatment of severe proximal humeral comminuted fractures can re-establish medial support of the proximal humerus and increase fixation strength. Fibular allograft and artificial shoulder joint replacement are also effective treatments for proximal humerus comminuted fractures among elderly individuals. However, these procedures cannot be performed in all regions. Compared to the aforementioned treatments, the use of the autologous fibular segment is more convenient and less expensive [4-6].
Humeral shaft nonunion occurs in 3% of all surgically treated fractures. Fixation with unstable construct can lead to macro-motion at the fracture site leading to nonunion. It presents pain and difficulty in the involved upper extremity while performing day-to-day activities. Instability in fracture fixation can also lead to macro-motion at bone-implant interface. Intramedullary (IM) interlock nailing is widely used for the primary fixation of diaphyseal fracture of long bones with good result. A large series of cases has been published in which screw-locking mistakes such as nail and screw failure, loosening of screws, delayed or non-unions were the most common reported complications. Various treatments modalities such as fixation by IM nailing, plating, augmentation plating after nailing, and external fixation. Long-standing humeral shaft nonunion treatment is more challenging as compared to recently diagnosed nonunion as it can present with larger bone defect and implant breakage. Two studies reported a case of humerus shaft nonunion operated with 2 nd generation IM interlock nailing with unstable construct complicated with peri-implant benign diaphyseal expansive lesion managed with implant removal curettage of lesion and stabilized with extraarticular distal humerus locking plate after strut fibular autobone grafting. The result was evaluated based on disability [7,8].
Proximal humerus fractures (PHFs) are with second most frequent incidence related to upper extremity, following distal forearm fractures. They represent approximately 5% of all fractures, display constantly increasing incidence [9], occur mostly in the population of over 65 years of age as a result of falls, and have a higher prevalence in females versus males. Epidemiologic changes with increasing severity of osteoporosis result in more common displaced PHFs. Approximately 20% of all PHFs are unstable and displaced, benefiting from the advantages of operative treatment. Special attention is required by three- and four-part fractures according to the Neer Classification. Different methods for open reduction and internal fixation (ORIF) exist, with locked plating being the standard treatment of choice for osteoporotic and/or comminuted PHFs due to the angular stable construct without plate-to-bone compression, enhancing vascularization and periosteal blood supply. However, despite the biomechanical advantages, the postoperative complication rate is still high. Among others, the most common complications are represented by varus collapse, screw cut-through and screw penetration, frequently indicated in cases with medial comminution or in elderly patients with poor bone stock.
A prerequisite for such complications is the reduced mechanical support due to fracture morphology [10]. On the other hand, the high rigidity of the locking plates could be another reason for cutting of the screws through the osteoporotic bone and subsidence of the humerus head fragment while the screws remain locked in position. Both screw cut-through and perforation risk implant penetration into the joint cavity, resulting in damage to the articular strictures, impaired joint function, and persistent pain. The penetration of the screws into the articulating joint of the humerus head carries the risk of glenoid wear and erosion. Studies have demonstrated a direct relationship of the medial calcar communication and local vascularization with the development of subsequent a vascular necrosis (AVN). According to a series of clinical and biomechanical reports, in case of poor bone quality, the challenging stable fixation can be considerably enhanced via placement of an allograft or an autograft [11].
Proximal humeral fracture is a common clinical fracture, which accounts for 5-6% of all fractures, and is the third most common fracture in the elderly. About 20% of proximal humeral fractures require surgical treatment [12]. Currently, the surgical treatment for proximal humeral fractures mainly involves open reduction and internal fixation and shoulder replacement. Shoulder replacement should be considered when the comminuted fracture is difficult to reduce, the rotator cuff cannot be repaired, or the blood supply to the humeral head is found to be severely compromised during preoperative assessment [13]. In the vast majority of the remaining cases, locking plates are widely used and have become the gold standard due to their anatomical shape, low profile, suture holes, and angular stabilization [14]. However, despite these advantages, the locking plate technique has been reported to have a high complication rate (10-35%) in the surgical management of proximal humeral fractures. The lack of anatomical reduction and support of the medial calcar has been considered to be the main cause of increased failure rate and nonunion [15].
Proximal humerus fractures, particularly anatomical neck fractures in older adults, are prone to failure of internal fixation, commonly resulting in poor prognosis and shoulder function. Patient factors, such as reduced local bone density, incomplete medial calcar support, and humeral head ischemia, may all precipitate these failures, in addition to surgeon-related factors, including inadequate fracture reduction and postoperative displacement [16]. OTA/AO type C proximal humerus fractures remain particularly challenging to treat due to these above-mentioned factors, in addition to difficulties in managing bone voids that remain after fracture reduction. Locking plate fixation remains the gold standard for the treatment of proximal humerus fractures. However, the use of locking plates in the treatment of proximal humerus fractures carries a high risk of complications, such as humeral head varus, screw penetrations, and internal fixation loosening. On the contrary, proximal humerus locking intramedullary nails have become increasingly popular with orthopedic physicians because of their minimally invasive insertion and good stability. Currently, there are no studies comparing the efficacy and safety of locking plates and intramedullary nail fixations in the treatment of OTA/AO type 11C1.1 and 11C3.1 proximal humerus fractures [2,17-19].
None.
None.