Osteoid osteoma of the foot can be difficult to diagnose, the clinical presentation may be mimicking other local pathologies leading to a considerable delay in diagnosis. We report an exceptional localization of osteoid osteoma in the second metatarsal in a 30-year-old patient, expressed for 3 years by metatarsalgia, with no clinical and radiological architecture defect of the foot. After discovering the nidus, the patient underwent surgical excision with an excellent outcome.
Osteoid osteoma, Forefoot, Metatarsalgia, Surgery
Osteoid osteoma is a relatively common benign bone tumor often discovered in the 2nd and 3rd decade [1]. It was described for the first time by Jaffe, et al. in 1935 [2]. In the foot, it frequently occurs in the talus, the metatarsal localization is uncommon, not exceeding 1.7% [3,4], only a few cases have been reported [5-8].
The diagnosis has been made easier with the availability of new imaging techniques such as computed tomography with 3 dimensional reconstruction and the use of magnetic resonance imaging (MRI) in medullary or abarticular localizations [9]. We report the case of a young male with an osteoid osteoma located at the base of the second metatarsal, a location not yet described in the literature to author's knowledge.
A 30-year-old patient consulted for metatarsalgia of the second ray of the left foot, evolving for several months, radiating towards the back of the foot. The clinical examination showed a square-shaped foot, without deformity of the 1st ray, nor claw toes, the pain was felt on palpation of the base of the 2nd metatarsal, the Muder's sign was negative, there were no retractions of the sural triceps, with the absence of any inflammatory or infectious signs.
X-rays of the forefoot were taken in the front and side views, and were initially considered normal (Figure 1). The patient was treated with nonsteroidal anti-inflammatory drugs (Diclofenac) with a rest period of two weeks. During this period, an improvement in the symptoms was noted, which rapidly deteriorated after the cessation of the medicine. A second radiological evaluation was performed after 3 months, using standard X-rays. This time, a lacunar image with a sclerotic border without any marked cortical thickening was observed, located at the metaphyso-diaphyseal junction of the 2nd metatarsal in the juxta-cortical aspect, which could be suggestive of a stress fracture or an osteoid osteoma (Figure 2). The CT scan showed a well-circumscribed lesion, round, 6 mm in diameter, and subperiosteal location, without cortical disruption (Figure 3). An MRI of the foot showed a nodular bone formation in T1 hyposignal, DPSF hypersignal, this abnormality of signal respects the continuity of the cortical bone, and there was no association with intramedullary or adjacent soft tissue edema (Figure 4).
 Figure 1: Anteroposterior and side X-rays of the left foot during the 1st consultation with no visible abnormalities.
View Figure 1
Figure 1: Anteroposterior and side X-rays of the left foot during the 1st consultation with no visible abnormalities.
View Figure 1
 Figure 2: Radiographs of the foot showing a round-shaped clarity next to the medial cortical bone of the 2nd metatarsal base.
View Figure 2
Figure 2: Radiographs of the foot showing a round-shaped clarity next to the medial cortical bone of the 2nd metatarsal base.
View Figure 2
 Figure 3: CT scan axial and sagittal views showing the intra-cortical nidus in the sub-periosteal location.
View Figure 3
Figure 3: CT scan axial and sagittal views showing the intra-cortical nidus in the sub-periosteal location.
View Figure 3
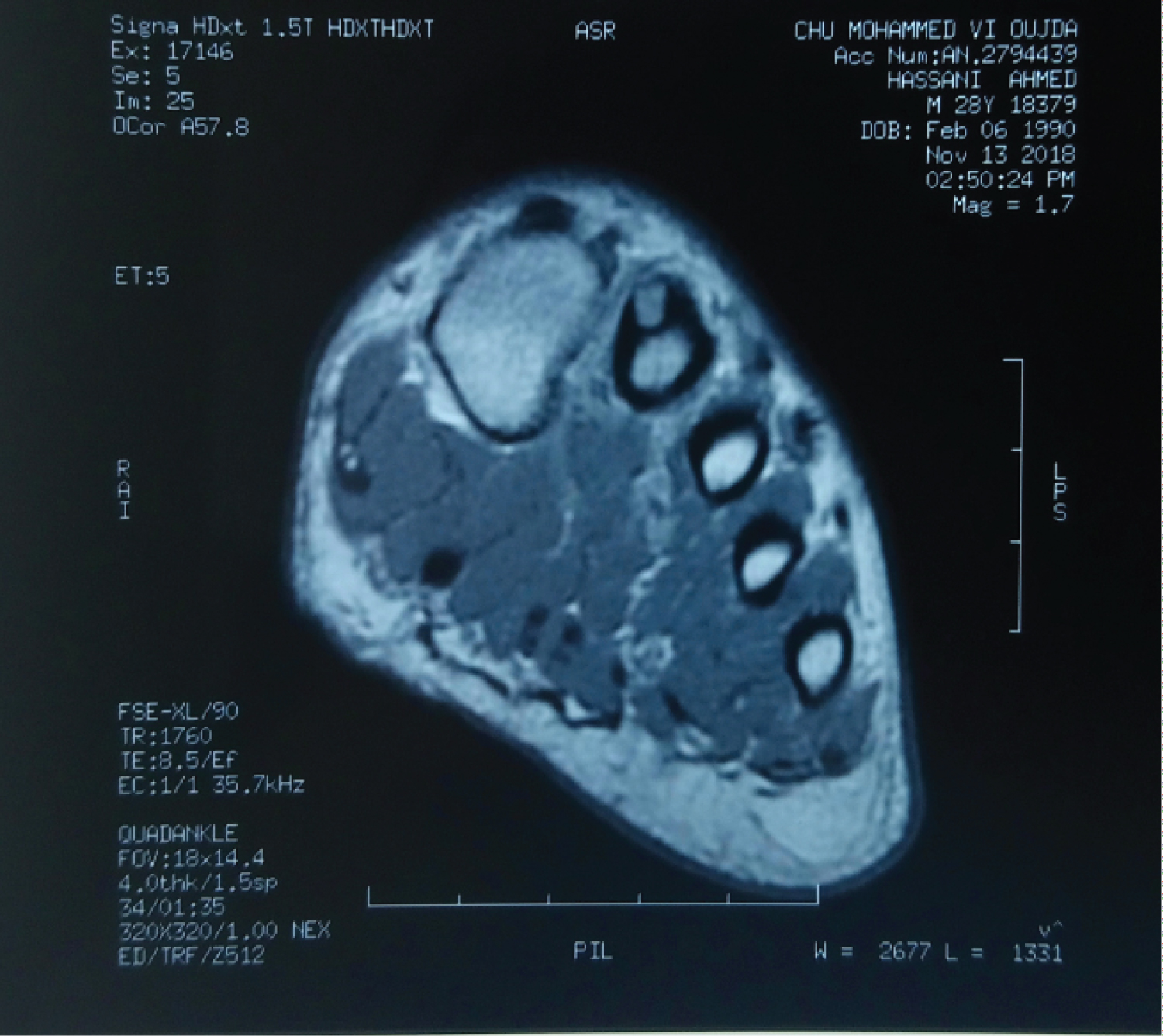 Figure 4: T1 MRI sequence in coronal view of the 2nd metatarsal showing the subperiosteal nidus, with no intramedullary cancellous bone or adjacent soft tissue changes.
View Figure 4
Figure 4: T1 MRI sequence in coronal view of the 2nd metatarsal showing the subperiosteal nidus, with no intramedullary cancellous bone or adjacent soft tissue changes.
View Figure 4
The patient underwent a block excision of the nidus with the help of fluoroscopy, and no bone grafting was required. Histological evidence confirmed the diagnosis of osteoid osteoma.
The postoperative course was very simple, the weight bearing was initially secured by Forearm crutches to provide comfort, and the patient was advised to self-rehabilitate. The patient was allowed to resume work after 3 weeks, and restart sports after 3 months. At the last follow-up, 12 months after the surgical excision, he had reached the previous state of physical activity, without any discomfort when putting on his shoes, nor any limitation, and with a complete absence of nocturnal pain. We also noted a complete disappearance of the nidus on the 12-month control radiograph (Figure 5).
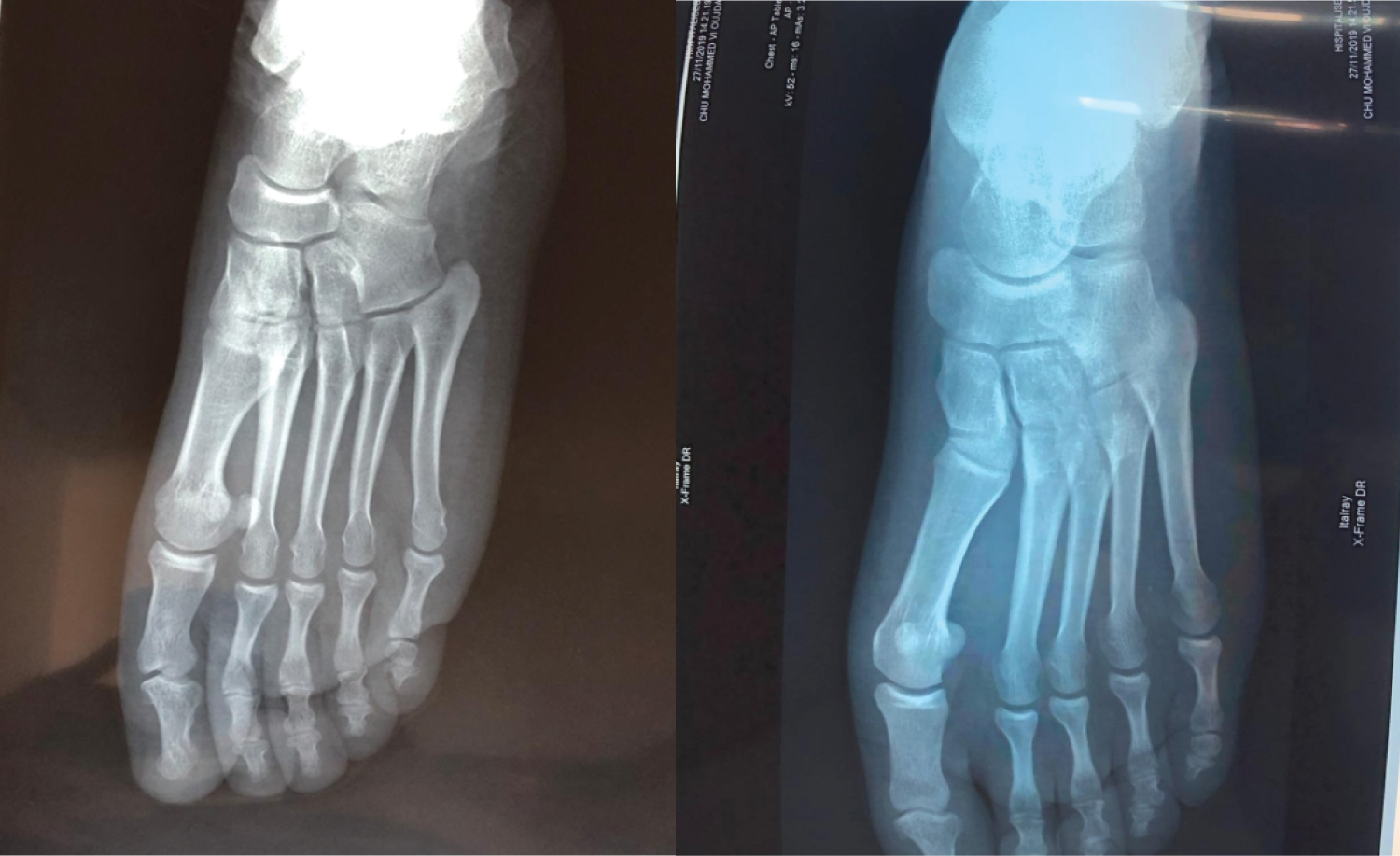 Figure 5: 12-month follow-up radiograph showing the complete disappearance of the nidus.
View Figure 5
Figure 5: 12-month follow-up radiograph showing the complete disappearance of the nidus.
View Figure 5
Shereff, et al. [10], by reviewing 10 cases of osteoid osteoma, noted that the duration of symptoms before a correct diagnosis was made ranged from 1 month to 4 years, and 80% of these patients had symptoms for over a year before diagnosis. Some other authors [11,12] have also reported delayed diagnosis for cervical (1 year) and lateral process talus (4 years) locations. In our case, it took 36 months to make the correct diagnosis.
According to Kenzora and Abrams [13], the reason for the delayed diagnosis is that there is little or no bone reaction on X-ray for some lesions, especially cancellous ones. Furthermore, from a pathological point of view, it seems that the nidus goes through a biological maturation process, starting with an initial stage where the nidus looks basically like healthy bone, to the stage where it is easily identifiable because of its hyperemic red appearance [13].
Standard foot radiographs may not provide enough accuracy to make the diagnosis, which seems to be happening in our case. We believe that this could be related to the unusual location of the lesion, or to the absence of the typical radiographic pattern, which is a round lucent spot containing a dense central nidus surrounded by sclerotic bone.
Computed tomography imaging is the most useful tool for a good analysis of the nidus, but MRI is much more sensitive for detecting cancellous localizations, as well as for searching for medullary edema or peripheral soft tissues [9,14]. For some authors [14], scintigraphy may be useful to eliminate a stress fracture.
Surgical removal of the nidus, either open or percutaneous with fluoroscopic guidance, are all approved treatments [3,7,9]. Arthroscopic resection is limited to the intra-articular form and shows good outcomes [11]. The trend is now towards radiofrequency thermo ablation, which is a valid indication for small lesions distant to the joints [8,15], but it remains an unavailable technique, especially in the least developed countries. In our case, we performed a complete surgical removal of the lesion, with no need for grafting as the lesion was limited in size. We achieved a complete and durable recovery with no recurrence at the last follow-up.
The metatarsal localization of an osteoid osteoma is one of the rarest, its diagnosis represents a true challenge, considering the amount of more common local pathologies. Based on our understanding of the literature, and the case we have presented, the diagnosis of osteoid osteoma should be considered when a combination of epidemiological and clinical arguments are present. A young male presenting with foot pain, mostly at night relieved when taking aspirin, should undergo a CT scan if standard radiographs are not helpful. The treatment is proposed according to the lesion's location and the facilities available to the surgeon.
The authors have declared no conflicts of interest. The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper. We the undersigned declare that this manuscript is original, has not been published before and is not currently being considered for publication elsewhere. We confirm that the manuscript has been read and approved by all named authors and that there are no other persons who satisfied the criteria for authorship but are not listed. We further confirm that the order of authors listed in the manuscript has been approved by all of us. We understand that the Corresponding Author is the sole contact for the Editorial process. He is responsible for communicating with the other authors about progress, submissions of revisions and final approval of proofs. Written informed consent was obtained from the patient to publish this report in accordance with the journal's patient consent policy on the title page of the manuscript.
We thank our colleagues who provided insight and expertise that greatly assisted the research, although they may not agree with all of the interpretations of this paper.
All authors contributed to the conduct of this research and read and approved the final version of the manuscript. Written informed consent was obtained from the patient to publish this report in accordance with the journal's patient consent policy on the title page of the manuscript.
No funding was disclosed by the author's.
We the undersigned declare that this manuscript is original, has not been published before and is not currently being considered for publication elsewhere.
We confirm that the manuscript has been read and approved by all named authors and that there are no other persons who satisfied the criteria for authorship but are not listed.
We further confirm that the order of authors listed in the manuscript has been approved by all of us.
We understand that the Corresponding Author is the sole contact for the Editorial process.
He is responsible for communicating with the other authors about progress, submissions of revisions and final approval of proofs.
Not applicable.
Consent was obtained from the patient for publication of this case report.