Cystic lesions of the minor salivary glands are very common. These lesions are referred to clinically and collectively as mucoceles and can be of either the extravasation or the retention type. Intraoral retention phenomenon is quite common but the presence of retention cyst extraorally mimicking as midcheek mass is rare. These lesions often arise from the salivary glands, but can also originate from the muscles, buccal fat pad, or other structures. We report a case of 40-year-old female presented to our department with lateral facial swelling which was diagnosed as mucous retention cyst on cytology and confirmed on histopathology after excision of the cyst via intraoral approach.
Mucocele, Mucous retention cyst, Extravasation cyst
Mucous retention cysts (extravasation type, mucoceles) are oral lesions most commonly diagnosed during routine surgical pathology service for dental practice. Extravasation mucous cyst results from a broken salivary gland duct and consequent spillage into the soft tissue thereby forming a mucous pool surrounded by granulation tissue with no epithelial lining. Mucous retention cyst appears due to decreased glandular secretion resulting from dilatation of duct [1,2]. The only histological difference between the retention cyst from extravasation type is the presence of epithelial lining. Thereby we report a case of retention cyst with a predominant lateral facial swelling.
A 40-year-old female reported to our department with a complaint of an asymptomatic swelling on the right side of the face. Patient gave history of similar swelling, much smaller in size 1 month back that regress on aspiration and relapsed in 2-3 days on its own. Patient had experience this twice in past 1 month. Medical history of the patient did not reveal any significant finding. Patient could not relate the occurrence of swelling to any event namely trauma, meals, dental pain, fever, etc. Incidentally, patient experienced increase in swelling while having his meals during this period. On examination, a diffuse swelling of about 6 × 4 cm extended from zygomatic arch to right lower border of mandible (supero-inferiorly) and from right oral commissure to the anterior border of masseter (anteroposteriorly) (Figure 1).
 Figure 1: Pre-operative profile.
View Figure 1
Figure 1: Pre-operative profile.
View Figure 1
The swelling was moderately firm, non-tender, fairly mobile and not fixed to the skin or underlying tissues. The color, texture and temperature of the overlying skin were normal (Figure 2). Cervical nodes were not palpable bilaterally. There was no eversion of ipsilateral ear lobe, and masseter was normal in palpation. Neck movements were normal and cranial nerve functions intact. Mouth opening was adequate, and there were no signs of any intraoral pathology or tooth decay. Patient experienced decreased salivation since few days. The differential diagnosis based on clinical findings included buccal space infection, dermoid or epidermoid cyst, branchial cleft cyst, lipoma, vascular malformation, recurrent lymphadenitis, recurrent sialadenitis, cyst/pseudocyst or tumor of salivary origin. Absence of inflammatory signs and normal intraoral findings excluded chances of infection.
 Figure 2: Swelling present in right cheek region.
View Figure 2
Figure 2: Swelling present in right cheek region.
View Figure 2
Ultrasonography revealed echogenic fluid collection with margins appearing irregular and with no evidence of calcifications. Aspiration of the lesion resulted in dirty brown fluid of a mucoid consistency that was sent for microscopic and biochemical examination. The clinical picture of aspirate reduced the probability of vascular anomaly, dermoid or epidermoid cyst to a great extent and was suggestive of mucous retention cyst. Serum amylase enzyme concentrations were found to be increased considerably. Other investigations such as MRI, CT Parotid Sialography were done for the patient. MRI gave impression of a well defined hyperintense peripherally enhancing thick walled cystic lesion of approx. 3.5 × 3.2 × 3.4 cm in subcutaneous region on right side of face. The lesion was seen to be anteriorly extending upto subcutaneous tissue and posteriorly closely abutting and displacing the masseter muscle (Figure 3).
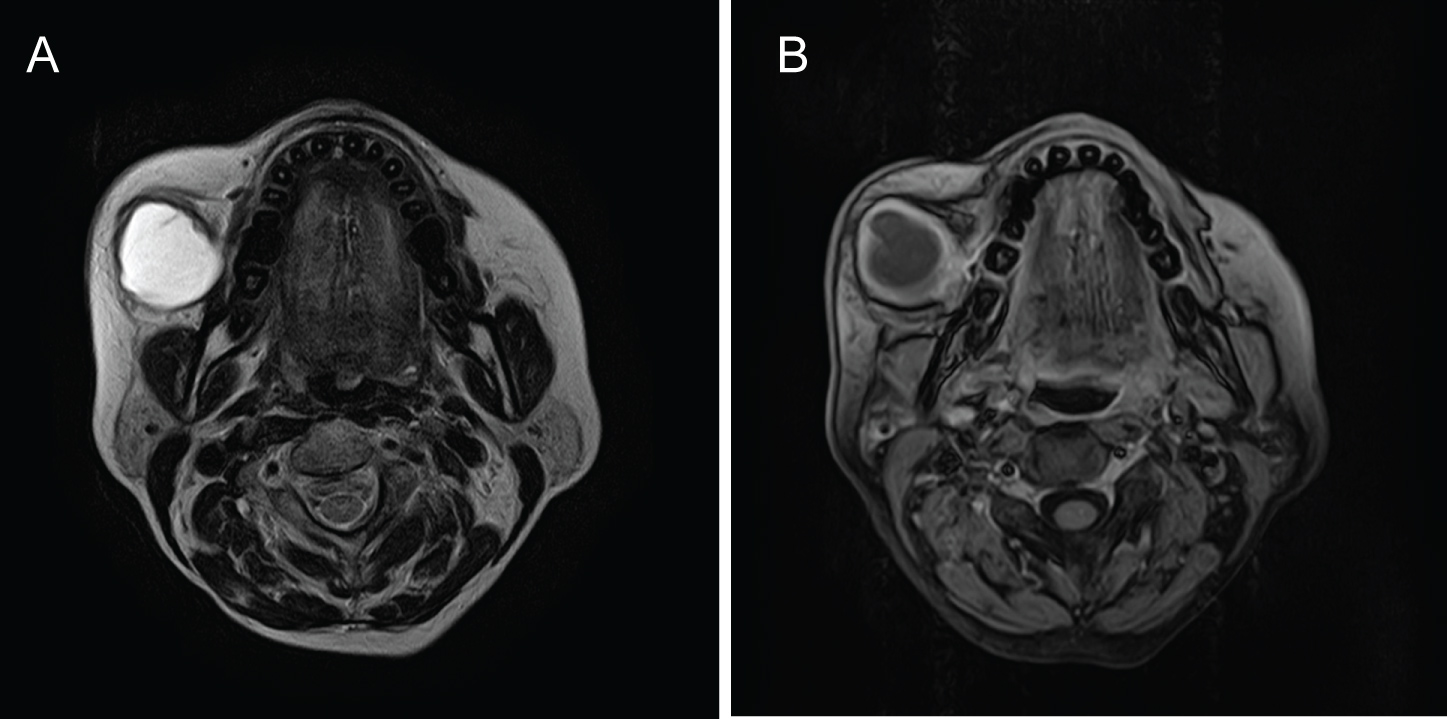 Figure 3: MRI revealing well defined hyperintense peripherally enhancing thick walled cystic lesion in subcutaneous tissue abutting and displacing masseter muscle.
View Figure 3
Figure 3: MRI revealing well defined hyperintense peripherally enhancing thick walled cystic lesion in subcutaneous tissue abutting and displacing masseter muscle.
View Figure 3
The lesion was approached intraorally via horizontal incision over right buccal mucosa 2 cm below the opening of stenson’s duct (Figure 4). A layered dissection was done and the cystic mass was exposed. After dissecting, the fluid was aspirated from the cystic lesion and the cystic cavity was removed in toto along with its entire epithelial lining. Adjacent vital structures were preserved, and respective duct ligated. Haemostasis was achieved and wound closure was done using 3-0 round body vicryl (Figure 5).
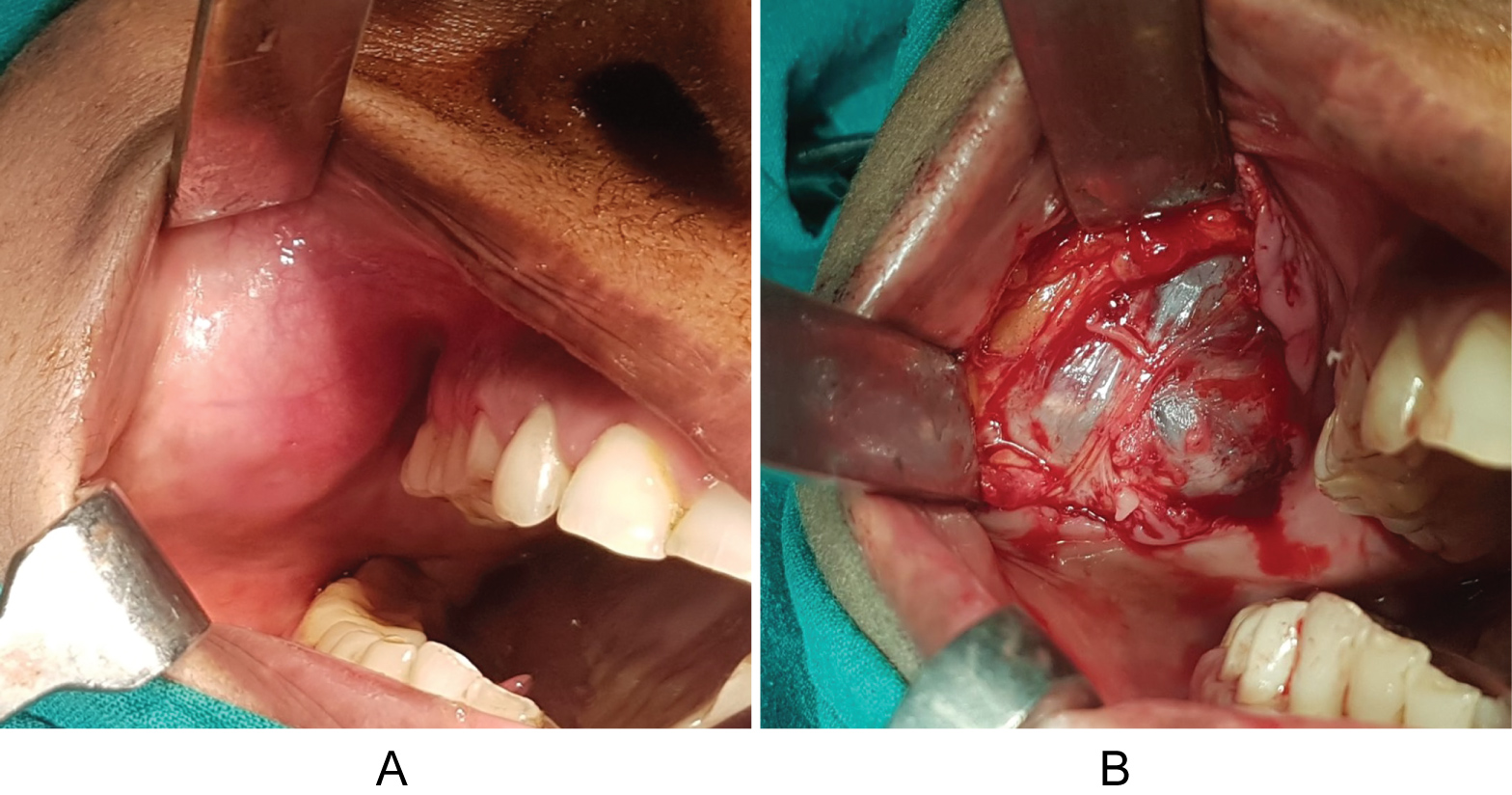 Figure 4: Lesion approached intraorally and excised in toto.
View Figure 4
Figure 4: Lesion approached intraorally and excised in toto.
View Figure 4
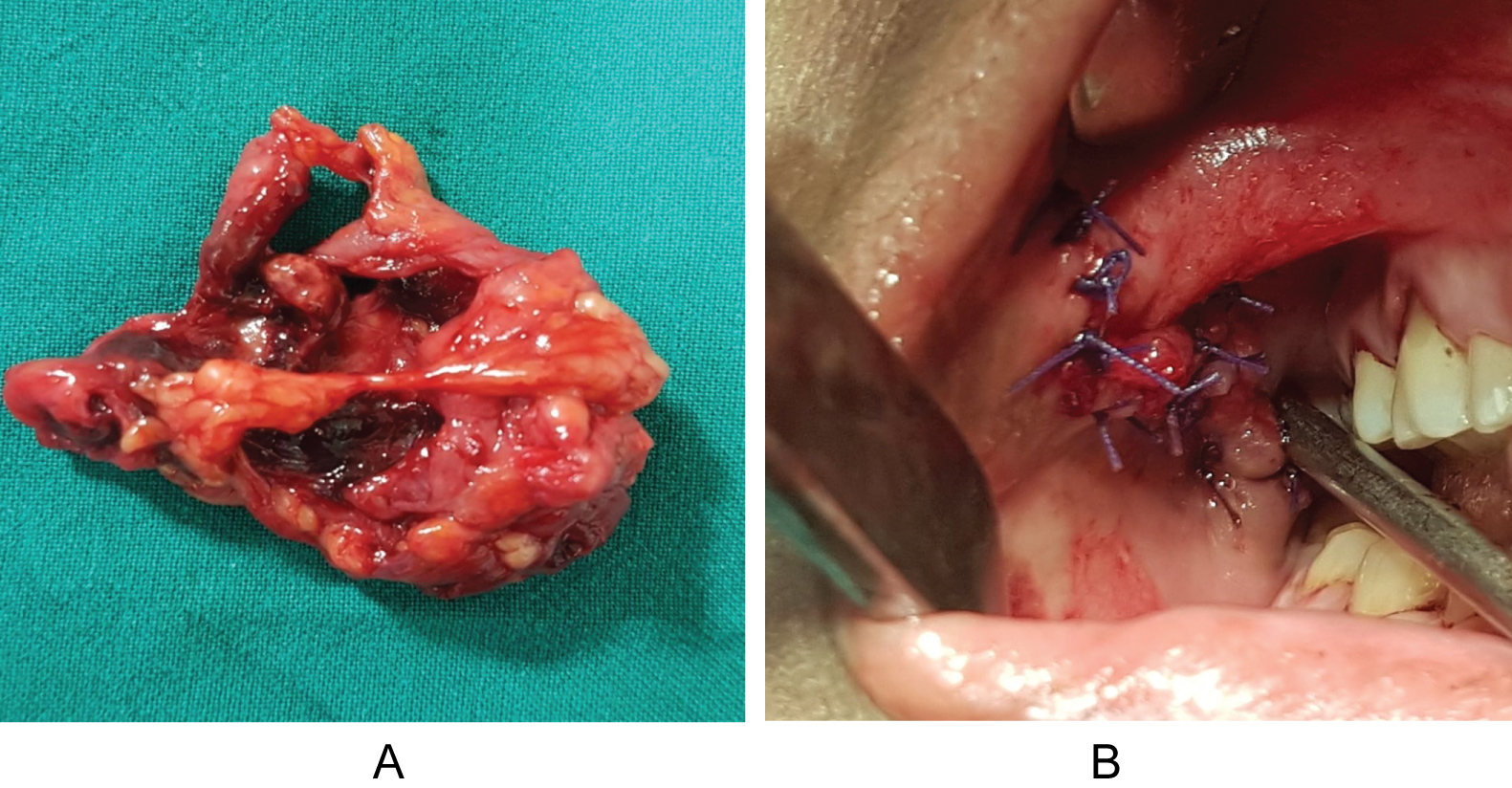 Figure 5: Excised cystic mass in-toto along with its entire epithelial lining and closure of defect using 4-0 absorbable suture.
View Figure 5
Figure 5: Excised cystic mass in-toto along with its entire epithelial lining and closure of defect using 4-0 absorbable suture.
View Figure 5
Histopathological analysis revealed fibrocollagenous tissue lined by stratified squamous epithelium. Rest showed ulceration and granulation tissue. Underlying muscle noted. The fibrocollagenous wall showed mixed inflammatory infiltrate comprising of neutrophils, lymphocytes and occasional plasma cells with haemorrhage (Figure 6). Thus a final diagnosis of mucous retention cyst was established as lymphoid tissue were not present in the histopathological specimen neither any dysplastic changes ruling out the possibilities of branchial cleft cyst and cystic squamous cell carcinoma respectively. Fine needle aspiration cytology which in correlation with clinical findings was suggestive of mucous retention cyst. Patient followed up for a period of 6 months with no evident complications and with satisfactory clinical outcomes (Figure 7).
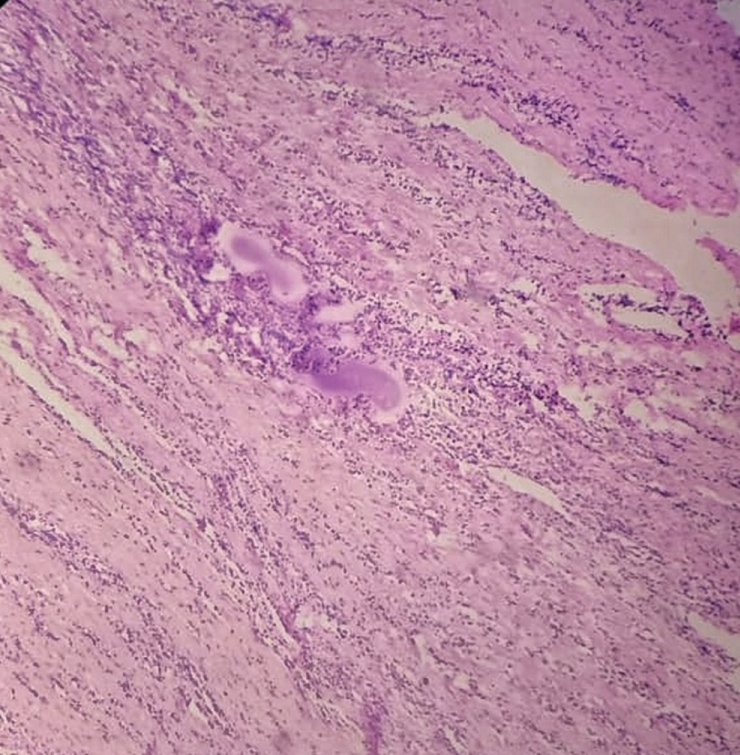 Figure 6: Histopathological specimen revealing fibrocollagenous tissue lined by stratified squamous epithelium with admixed inflammatory infiltrate s/o mucous retention cyst.
View Figure 6
Figure 6: Histopathological specimen revealing fibrocollagenous tissue lined by stratified squamous epithelium with admixed inflammatory infiltrate s/o mucous retention cyst.
View Figure 6
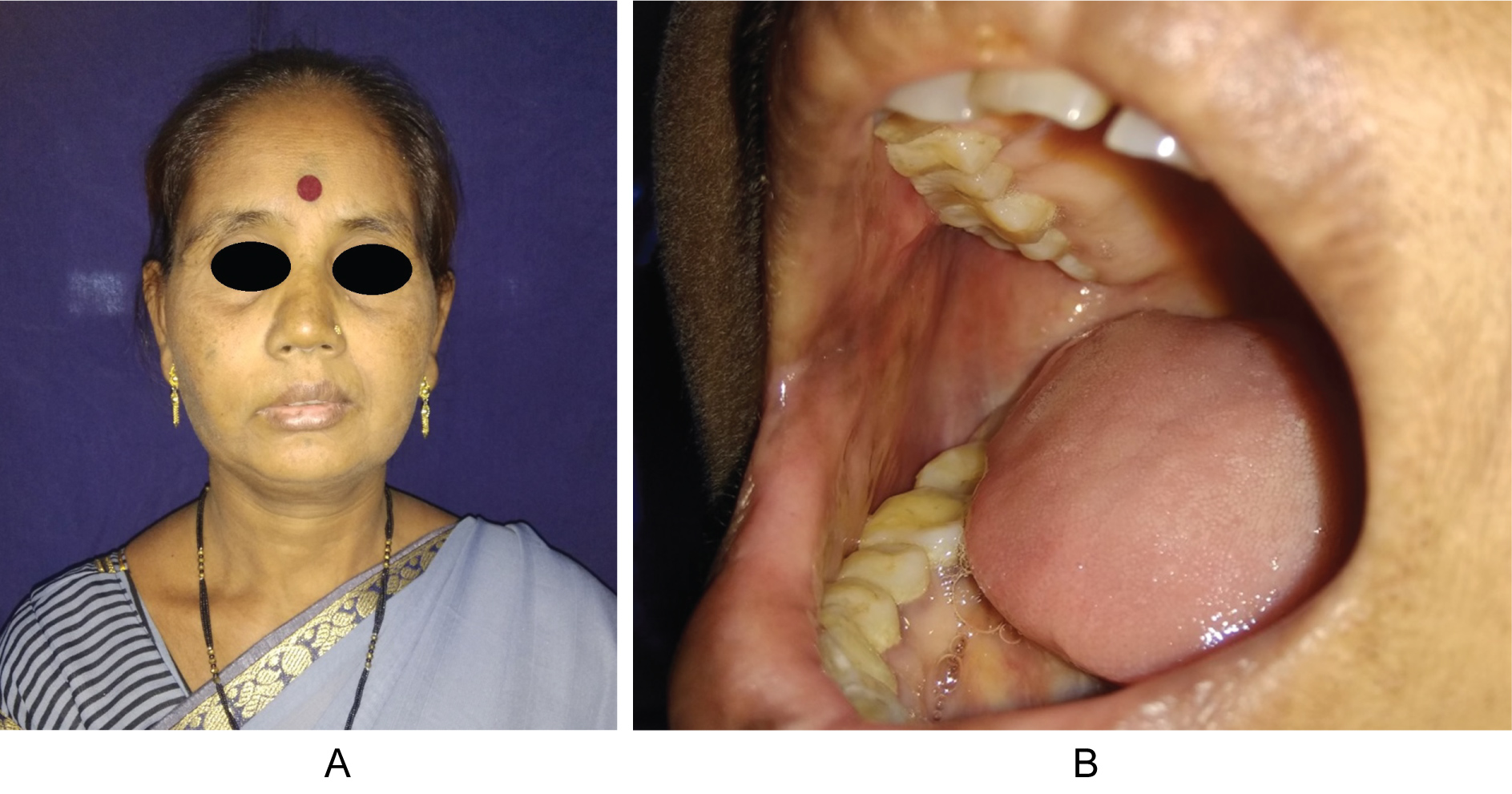 Figure 7: Follow up with no recurrence.
View Figure 7
Figure 7: Follow up with no recurrence.
View Figure 7
Mucoceles are mucus containing cystic lesions of the minor salivary glands with a prevalence of 2.4 cases per 1000 people and are 15th most common oral mucosal lesion. Mucoceles occurs in young individuals, with 70% of them being younger than 20 years. Superficial mucoceles tend to occur in individuals older than 30 years and ranulas in children and young adults, with a peak frequency in the second decade. Mucus retention cysts occur in older individuals; the peak prevalence occurs in persons aged 50 - 60 years. The most common site of occurrence is the lower lip followed by tongue, floor of mouth (ranula), and the buccal mucosa.
Mucous extravasation results from rupture of minor or major salivary duct due to trauma. Irrespective of the cause, extravasation leads to mucin pool in tissue spaces and elicits inflammatory response. Granulation tissue forms around the mucin and encapsulation occurs to form a pseudocyst. When this extravasation occurs in superficial tissue planes, it clinically presents as a fluctuant, painless and bluish swelling in the region of lower lip, floor of the mouth, ventral tongue or buccal mucosa. Other regions such as the palate, retromolar region and submandibular gland are rare sites for extravasation probably due to low susceptibility to trauma [3].
The mucous retention phenomenon occurs as a result of obstruction of the duct by a sialolith or a stricture. The hindrance in the flow of saliva from gland to the oral cavity leads to its accumulation in duct and back pressure. The flow from gland continues, and this causes gradual inflation of ductal diameter to accommodate the salivary volume. The pooled saliva is walled by inflated duct making the picture resemble a cystic pathology. It is more of a true cyst, as there is the presence of an epithelium lining. Back pressure may inflame the gland and cause acute/chronic recurrent sialadenitis. The signs and symptoms and management vary with the type of gland involved and the anatomical position of obstruction.
The clinical appearance of a mucus cyst is a distinct, fluctuant, painless swelling of the mucosa. About 75% of the lesions are smaller than 1 cm in diameter; however, rarely, the size can vary from few millimeters to several centimeters. Superficial lesions take on a bluish to translucent hue, whereas deep lesions have normal mucosal coloration and bleeding into the swelling may impart a bright red and vascular appearance. The patient may relate a history of recent or past trauma to the mouth or face or the patient may have a habit of biting the lip. The various differential diagnoses are Blandin and Nuhn mucocele, oral hemangioma, oral lymphangioma, lipoma, and soft tissue abscess [4].
Fine-needle aspiration cytology (FNAC) and MRI are more useful for the diagnosis. FNAC invariably gives high amylase content, and microscopic examination would present as inflammatory cells in mucoid background. MRI serves two purposes. First, it narrows down the differential diagnosis and second, it helps to localize the gland involved with exact dimensions and planes of the lesion.
Mucous retention cyst are a common phenomenon, however their occurrence as midcheek mass is not quite common. These lesions often arise from the salivary glands, but can also originate from the muscles, buccal fat pad, or other structures. Surgical excision of the entire cystic mass has been suggested as the comprehensive line of management. The excised tissue should be submitted to the pathological investigations to confirm the diagnosis. Laser ablation, cryosurgery, and electrocautery are approaches that have also been used for treatment of the conventional mucoceles, with variable success [5,6].