Depressive, anxiety and somatic disorders are three major diagnostic groups of common mental health disorders that can affect health related quality of life negatively. Poor quality of life (QoL) in people with common mental disorders may increase the susceptibility to medical problems such as chronic heart disease, diabetes mellitus and hypertension. Quality of life is also the most sensitive indicator of the effects of psychiatric treatment. However, studies that assess the QoL of people with common mental health disorders (CMD) are limited and their method of data analysis does not consider the complex relationship of factors that affect it. This study was done to fill the information and methodological gap.
An institution based cross-sectional study was conducted from March 31 to May 29, 2021 in St. Amanuel Mental Specialized Hospital in Ethiopia. Data related to socio-demographics, and clinical factors and HRQoL was collected from 679 patients with common mental disorders through face to face interviews. Online based data collection was employed with kbotoolbox online data collection server. Data was exported to STATA 14 for further analysis. Structural Equation Modeling was employed to verify relationships and association among exogenous, mediating and endogenous variables.
The final analyses included 679 patients. The mean score for HRQoL was 40.8. The environmental health domain was the most affected domain of HRQoL with mean score of 35.4. Being not physically active had both direct and indirect negative effect on overall HRQoL. Rural residence, unemployment and longer duration of follow up had a negative indirect effect in overall HRQoL. Older age had a direct positive effect on social related domain. Absence of disease relapse had a direct positive effect on psychological health domain.
Patients with CMD had poor quality of life in all domains WHOQOL-BREF and overall health-related quality of life. Socio-demographic factors (Age, educational status, residency, payment method for health service and occupational status), clinical factor (comorbid condition and duration of follow up) and physical activity were factors associated with HRQoL among adults with CMD. Thus we suggest that improvement in quality of life should be a central goal of mental health policy and better to develop physical exercise, educational and occupational status to improve the health-related quality of life of patients with common mental disorders.
Common mental disorders, Health related quality of life, Associated factors, Structural equation modeling
AMSH: Amanuel Mental Specialized Hospital; CFA: Confirmatory Factor Analysis; CFI: Comparative Fit Index; CMD: Common Mental Disorders; DAGs: Directed Acyclic Graphs; ETB: Ethiopian Birr; HRQoL: Health-Related Quality of Life; MARS: Medication Adherence Rating Scale; OSSS: Oslo Social Support Scale; QOL: Quality of Life; RMSEA: Root Mean Square Error of Approximation; SD: Standard Deviation; SEM: Structural Equation Modeling; SPSS: Statistical Package for Social Sciences; STATA: Data Analysis and Statistical Software; St.: Saint; TLI: Tucker-Lewis Index; UoGCSH: University of Gondar Comprehensive Specialized Hospital; WHO: World Health Organization
Health is a state of complete physical, mental and social well-being and not merely the absence of disease or infirmity [1]. In turn, this definition has given rise to theoretical and philosophical ideas of what constitutes mental wellbeing and arguments for assessing both positive and negative outcome [2].
Life has two dimensions, according to Patrick and Erickson: quantity and quality [3]. In terms of "hard" biomedical data, such as death rates or life expectancy, the quantity of life is expressed. Quality of life refers to intricate aspects of life that cannot be expressed by the use of quantifiable metrics alone; it represents an overall subjective assessment of life. However, it comprehends not only the subjective sense of well-being, but also objective indicators such as health status and external life circumstances [4].
WHO defines Quality of Life as an "individual's perception of their position in life in the context of the culture and value systems in which they live and in relation to their goals, expectations, standards and concerns. It is a broad ranging concept affected in a complex way by the person's physical health, psychological state, level of independence, social relationships, personal beliefs and their relationship to salient features of their environment" [5]. Quality of life has recently been recognized as a significant component and prognostic predictor of mental illness and is recommended for use in the clinical evaluation and interventions of people with serious mental illness [6,7].
Common mental disorder (CMD) is a term used to describe a group of mental disorders that frequently occur they include depression, anxiety and somatisation (medically unexplained somatic symptoms such as headaches and backache) [8,9].
Depression disorder presents with depressed mood, loss of interest or pleasure, decreased energy, feelings of guilt or low self-worth, disturbed sleep or appetite, poor concentration, problem of thinking and making decisions, and, in severe stages, recurring thoughts of death or suicide [10].
The American Psychiatric Association, on the definition of anxiety, describes anxiety as the anticipation of a future concern and is more associated with muscle tension and avoidance behavior. It can cause people to try to avoid situations that trigger or worsen their symptoms. Job performance, school work and personal relationships can be affected [11].
Somatic symptom disorder is characterized by one or more somatic symptoms associated with significant distress and plus abnormal thoughts, feelings, and behaviors in response to these symptoms rather than the absence of a medical explanation for somatic symptoms [12].
Although interest in the impact of common mental disorders on health related quality of life is growing, many questions remained unanswered and there are limited studies in our country. Also undetermined are the roles of physical activity and comorbid conditions in relation to quality of life impairment in the common mental disorders. In addition, most of previous studies done on HRQoL among common mental disorder patients consider HRQoL as observed variable but in fact it is a multidimensional concept that is best measured by a number of latent constructs. Therefore, more research is needed to elucidate these issues and to fill the methodological gap. And addressing health related quality of life regarding to mental health mainly in common mental disorders during and after the global health crisis COVID 19 should be placed into the international and national public health agenda to improve citizens' wellbeing.
An institution based cross-sectional study design was conducted at St. Amanuel mental specialized hospital, Ethiopia from March 31 to May 29, 2021. Ethiopia is the second most populous nation in Africa with the population in 2021 is 117,876,227 [13]. Currently, St. AMSH is the only biggest and specialized psychiatric hospital in the country serving for people from the nine regions and two city administrations of the country (Figure 1).
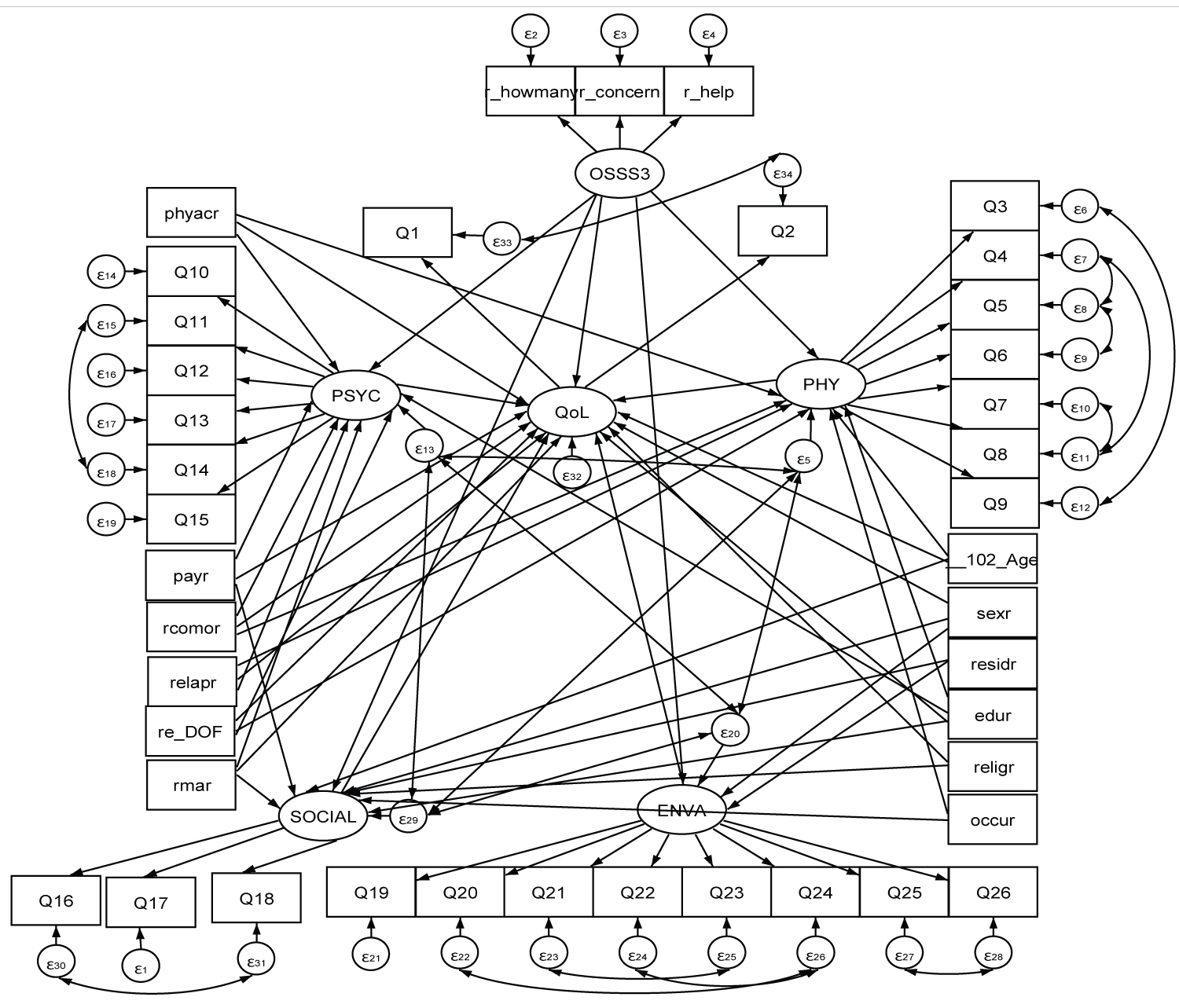 Figure 1: Conceptual frame work for causal factors of health related quality of life among patients with common mental disorders attending an outpatient clinic at Saint Amanuel Mental Specialized Hospital, Ethiopia, 2021.
View Figure 1
Figure 1: Conceptual frame work for causal factors of health related quality of life among patients with common mental disorders attending an outpatient clinic at Saint Amanuel Mental Specialized Hospital, Ethiopia, 2021.
View Figure 1
Saint Amanuel Mental Specialized Hospital serves at inpatient and outpatient bases of people with mental illness and other medical illness. The Hospital has 259 beds including 11 private wing beds and 23 emergency beds and also it has 13 outpatient departments (OPDs). An average of 10,320 patients get service per month and most patients attend the Hospital with family members. The hospital is also playing its pivotal role as a training institute for psychiatric professionals of different levels; so as to expand the service throughout the country by introducing psychiatry service to the primary health care system.
The study was conducted at Saint Amanuel Mental Specialized Hospital which is situated in the capital city of Ethiopia, Addis Ababa.
The source population was all clients diagnosed with common mental disorders with age above or equal to 18 years, having follow-up visit for at least 6 months in St. Amanuel mental specialized hospital. Whereas clients diagnosed with common mental disorders with age above or equal to 18 years, having follow-up visit for at least 6 months in St. Amanuel mental specialized hospital and present during the data collection period was the study population. Clients diagnosed with common mental disorders with age above or equal to 18 years, having follow-up visit for at least 6 months in St. Amanuel mental specialized hospital and present during the data collection period were included in the study. Those Patients who had chronic severe psychiatric condition (e.g., psychosis) were excluded.
Sample size is determined based on the number of free parameters in the hypothetical model; a 1:5 ratio of respondents to free parameters to be estimated has been recommended [14]. Number of distinct parameters to be estimated (excluding those nine values fixed with 1) = 118.
29 variances of independent variables, 5 variance of latent variables, 24 coefficients of latent factors with indicators and 4 regression coefficient and 12 covariances of disturbances, 6 covariance between domains and 38 regression coefficient between indicators and latent Accordingly, considering the 118 parameters to be estimated based on the hypothesized model, taking participants to free parameters ratio of 5, the minimum sample required is 590.
The sample size calculated adjusted to account for non-response rate 15% and therefore considered it to demonstrate the final sample size. Then the final sample size becomes 679.
Based on the estimation we got from the preceding months, on average 1000 patients with CMD visited per month, according to this we used Systematic random sampling technique with "k" interval of 3 was employed to withdraw samples from study population.
Data was collected with face to face interview using semi-structured questionnaires. The questionnaire had different domains, including socio-demographic profile, clinical related questions and world health organization quality of life brief (WHOQOL-BRFE). Data related to socio demographic and clinical characteristics of CMD, variables like age, sex, marital status, residence, educational status, occupational status, duration of follow up, comorbidity and disease relapse was obtained by reviewing the chart and interview. And lastly all 26 item variables were obtained by interviewer administered face to face interview. Smart phone and tablet based online data collection was employed with kbotoolbox online data collection server.
The outcome variable Health related quality of life measurement domain questionnaire was adopted from WHOQOL which is also validated in Ethiopia and countries in the world It has 4 domains that denote an individual's perception of quality of life in each particular domain. The WHOQOL-BREF is a 26-item instrument consisting of four domains: physical health domain (7 items), psychological health domain (6 items), social relationships domain (3 items), and environmental health domain (8 items) and it also contains the overall perception of QOL and general health (2 items) [15]. And also we were made pilot study and validated for our specific study population with Cronbach's alpha of 0.94 and the Bartlett's Test of Sphercity had a degree of freedom = 300 and it was significant.
Overall HRQoL: Defined as the average of the four domain scores. HRQoL profile categorized as low, moderate and high when the mean score was less than or equal to 45, 45-65 and greater than 65 respectively, for all domains and overall HRQoL [5].
The Oslo Social Support Scale (OSSS-3) sum score ranges from 3 to 14 and can be operationalized into three broad categories of social support. 3-8 poor social support 9-11 moderate social support 12-14 strong social support [16].
Physical activity is any bodily movement produced by skeletal muscles that requires energy expenditure include walking, cycling, wheeling, sports, active recreation and play, and can be done at any level of skill and for enjoyment by everybody. For Adults aged 18-64 years regular exercise, they should do at least 150-300 minutes of -moderate-intensity aerobic physical activity; or at least 75-150 minutes of vigorous-intensity aerobic physical activity; or an equivalent combination of moderate- and vigorous-intensity activity throughout the week [17].
The returned data was exported to STATA version 14 for further analysis. Descriptive and summary statistics was done using figures, tables and texts.
Reliability was also assessed for each domain of WHO-QoL -Bref using the Cronbach's α coefficient and value of 0.7 and higher was considered satisfactory. The raw score of each domain of WHO-QOL -Brief was obtained by multiplying the mean of their corresponding items by four for each participant. Then two linear transformation was performed, in the first transformation method the scores converted to range between 4-20 by multiplying the mean of items in each domain by 4, then the second transformation method converts domain cores to scores 0-100-scale using a formula = .
The Structural Equation Modeling (SEM) was employed to examine the relationship between various exogenous, endogenous and mediating variables after the assumptions are fulfilled, and modifications was performed iteratively by adding path links or including mediator variables, if theoretically supported, and comparing the Root Mean Square Error of Approximation (RMSEA), Comparative Fit Index (CFI) and Tucker-Lewis index (TLI) of each model fitted after the assumptions normality and adequate sample size are fulfilled. Hence, distributions of the items are nonnormal, and the results produced by the normal theory maximum likelihood (ML) approach may be misleading. The basic idea of the multivariate probit model approach or the expectation-maximization (EM) algorithm approach is relating the ordinal categorical item to an underlying continuous normal distribution through a threshold specification. Estimates of the unknown parameters are obtained on the basis of the ordinal categorical data that are correctly treated by an underlying multivariate normal distribution with a threshold specification. Finally, an over identified model with value RMSEA = 0.05, CFI = 0.87 and TLI = 0.85 was retained. Diagrammatically, the effect of each exogenous or mediating variable on the respective dependent variable was indicated by the path coefficient along with single headed arrow, and the correlation among disturbances (residual errors that reflect the unexplained variances in the latent endogenous variables due to all unmeasured causes) was indicated by double arrows. Statistically significant effects were assumed for P 0.05 at Confidence interval of 95%.
If mediation of effects present, the direct, indirect, and total effects was determined using the Expectation-maximization maximum likelihood estimator technique.
The goodness of fit was assessed by comparative fit index (CFI), Root mean squared error of approximation (RMSEA) and Tucker-Lewis index (TLI).
Ethical approval to conduct the study was obtained from university of Gondar, college of medicine and health science, institute of public health institutional review board, the study will announce to university of Gondar before proceeding any further. An ethical clearance and a permission letter were obtained from EkaKotebe General Hospital and St. Amanuel Mental Specialized Hospital. The purpose of the study, potential risk, benefits and rights of participants was explained. Verbal consent was obtained from the participants and assured about the confidentiality of the information given by them during all phases of research activities. Personal identifiers, such as name, address and any other private information was collected for the sake of privacy. And throughout the data collection period, preventive measures for the global pandemic COVID19 was strictly enforced, including the use of face masks, hand washing, keeping physical distance, well ventilated place, and sanitizer use, as well as environmental disinfection.
A total 679 participants were included in the study of them 363 (53.5%) were men, 312 (46%) were single, 216 (31.8%) educated up to secondary education and 153 (22.5%) were unemployed. The median age of participants was 34 (IQR = 17) years (Table 1).
Table 1: Show socio-demographical, behavioral and clinical characteristics of adults with CMD attending an outpatient clinic in St. AMESH. View Table 1
For the OSSS-3, the internal consistency was satisfactory with chronbach's alpha of 0.82. considering the sample as a whole, the mean score of social support was 8.75 (SD = 2.64).
More than one quarter (43.9%) of the patients had poor social support level (Figure 2).
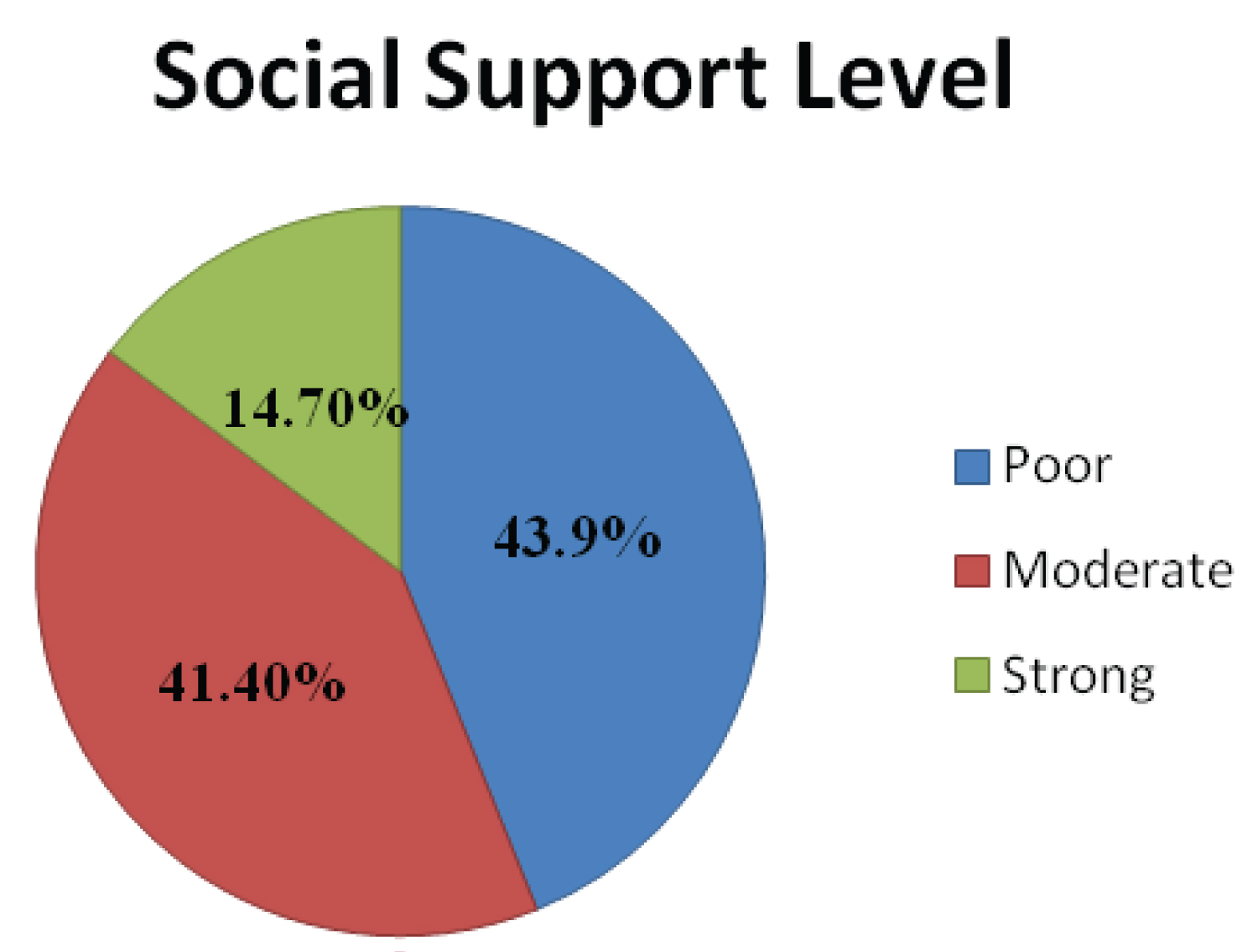 Figure 2: Social support level of common mental disorder patients attending an outpatient clinic at St. Amanuel Mental Specialized Hospital, 2021.
View Figure 2
Figure 2: Social support level of common mental disorder patients attending an outpatient clinic at St. Amanuel Mental Specialized Hospital, 2021.
View Figure 2
The mean score of the overall QoL was 40.79 (with SD = 15.49). The minimum and maximum mean scores of the study participants in overall QoL were 2.72 and 91.18, respectively (Table 2).
Table 2: HRQoL of patients with CMD in St. AMESH, 2021. View Table 2
Study participants were asked to give their perception on their quality of life and health satisfaction. Based on their response; about one third 237 (34.9%) of the study participants reported that their quality of life was neither poor nor good, while 186 (27.4%) of them had poor quality of life (Figure 3).
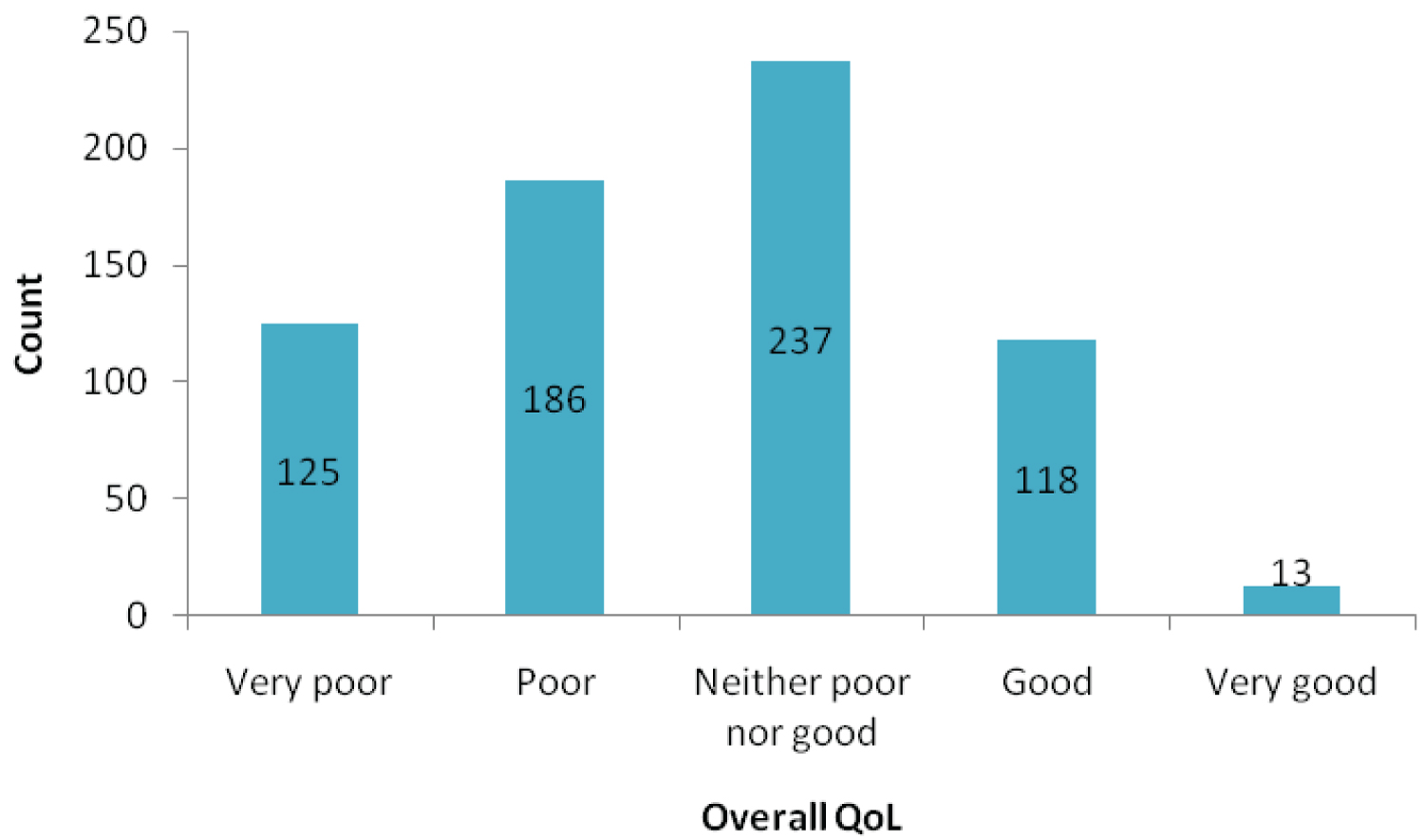 Figure 3: Perceived self-rated QoL of common mental disorder patients attending an outpatient clinic at St. Amanuel Hospital, 2021.
View Figure 3
Figure 3: Perceived self-rated QoL of common mental disorder patients attending an outpatient clinic at St. Amanuel Hospital, 2021.
View Figure 3
Regarding to the health satisfaction, 225 (33.1%) of them were neither satisfied nor dissatisfied with their health and 205 (30.2%) of them were dissatisfied with their health (Figure 4 and Table 3).
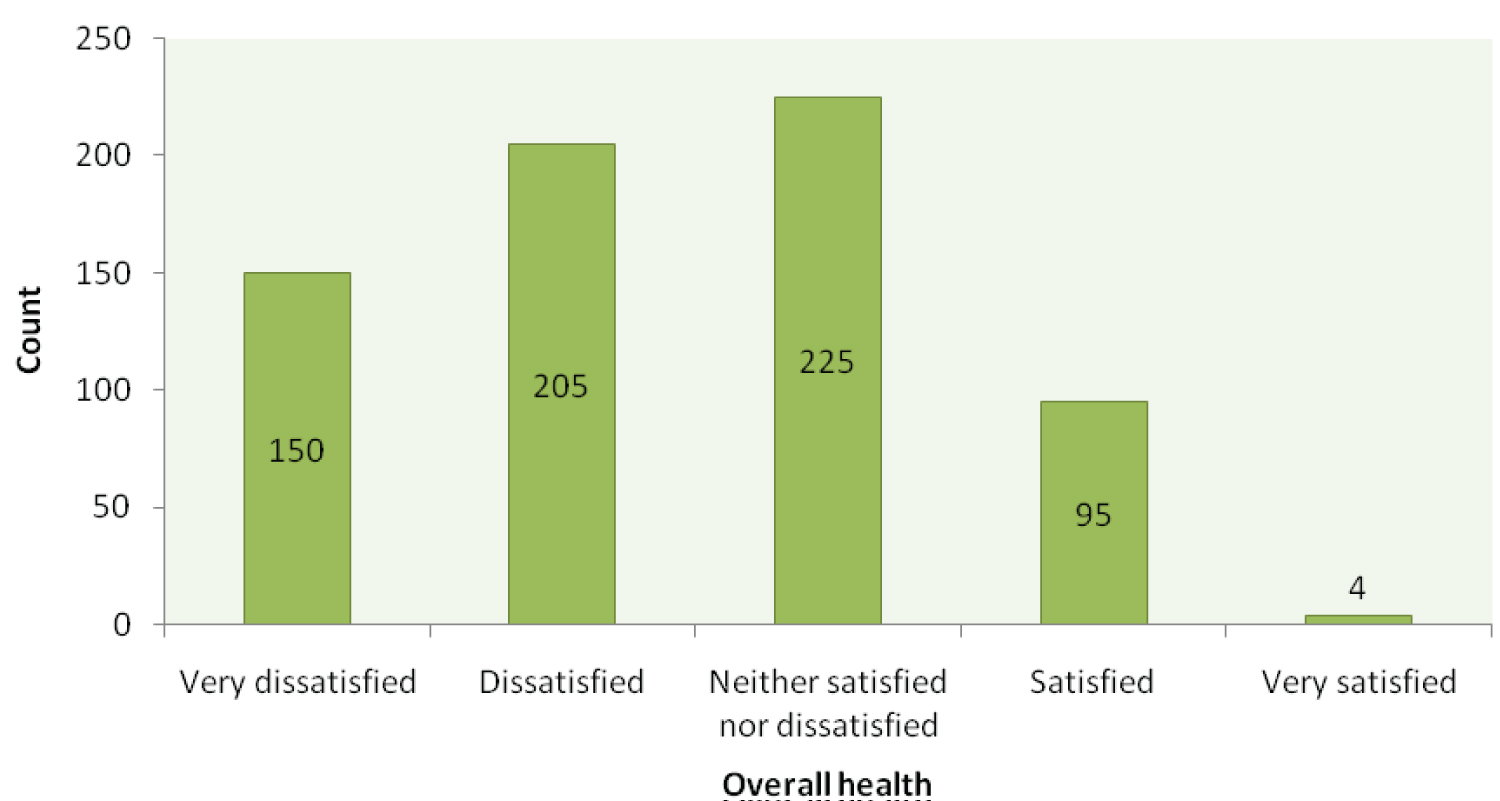 Figure 4: Perceived self-rated health satisfaction of common mental disorder patients attending an outpatient clinic at St. Amanuel Hospital, 2021.
View Figure 4
Figure 4: Perceived self-rated health satisfaction of common mental disorder patients attending an outpatient clinic at St. Amanuel Hospital, 2021.
View Figure 4
Table 3: Internal consistency and correlations between the domains of WHOQoL-Brief. View Table 3
The final model containing both the structural part (relationships among latent or observed variables) and the measurement part (relationship between a latent variable and its indicator or items) is shown in Figure 5 and Table 4. The fitted model was relatively parsimonious and good fitted with REMSA = 0.05.
 Figure 5: SEM for factors associated with HRQoL among adults with CMD attending an outpatient clinic in St. AMESH, 2021.
View Figure 5
Figure 5: SEM for factors associated with HRQoL among adults with CMD attending an outpatient clinic in St. AMESH, 2021.
View Figure 5
Table 4: The direct, indirect and total effect of socio-demographical, clinical and behavioral factors on HRQoL domains among adults with CMD attending an outpatient clinic in St. AMESH, 2021 (Derived from SEM). View Table 4
The eleven exogenous variables were both directly and indirectly related with HRQoL via the mediator variables.
This estimated structural equation model indicates that environment health factor had the most substantial causal effect on HRQOL, which was larger than the causal effects of psychological QOL, physical health and social relationship factors. Physical health was statistically significant associated with occupational status (p = 0.014), comorbid condition (p = 0.00002) and duration of follow up (p = 0.02) and regarding to environmental health domain, it was associated with residency (p < 0.00006) and payment method for health service (p = 0.0002) (Figure 5).
Having comorbid condition had a direct positive effect on physical health (β = 0.19, 95% CI 0.10 to 0.28), psychological health (β = 0.20, 95% CI 0.12 to 0.28) and both positive direct (β = 0.23, 95% CI 0.11 to 0.35) and indirect effect (β = 0.10, 95% CI 0.04 to 0.15), consistently a total positive effect (β = 0.33, 95% CI 0.20 to 0.45) on HRQoL.
Being rural residency had a direct negative effect on environmental health (β = -0.14, 95% CI -0.2 to -0.07) and a negative indirect effect on HRQoL (β = -10.51, 95% CI -15.80 to -5.22) and Environment Health (β = -0.6, 95% CI -0.10 to -0.001). Older age had a direct positive effect (β = 0.010, 95% CI 0.005 to 0.14) on social relation domain.
Longer duration of follow up had a negative direct effect on physical health (β = -0.012, 95% CI -0.022 to -0.002) and both negative direct (β = 0.22, 95% CI -0.33 to -0.11) and indirect effect (β = -0.015, 95% CI 0.024 to -0.006), accordingly a total negative effect (β = -0.24, 95% -0.34 to -0.13).
In this study, we aimed to construct a hypothetical model and verify the significance of the direct/indirect paths and the goodness of fit of the model under the theoretical assumption that demographic factors, disease-related factors, and physical activity to determine the QoL of patients with CMD directly and indirectly and to estimate the magnitude of HRQoL of CMD patients.
While measures of functioning focus on objective, quantifiable impairments that exist, measures of quality of life assess enjoyment and life satisfaction associated with various activities [18]. The invisible suffering on the account of impact of the anxiety and depression on every aspect of life compromises the QOL of patients not only during the active symptomatic state but often beyond symptomatic recovery [19]. Our findings are discussed below in the light of the literature referenced.
According to our study, Adults with CMD were found to have significant lower quality of life in all domains of the WHOQOL-BREF and in overall quality life. Direct comparisons with the findings of other studies are difficult because there are no other comprehensive QOL studies of patients with CMD from Ethiopia or other countries. However, although the patient group was different, this finding is congruent with previous studies on QoL that targeted patients with depression [20,21]. This finding also congruent with previous studies done on QoL of anxiety patients [22,23]. This consistence may be due to the emotional component of subjective well-being consists of high levels of positive affect (experiencing pleasant emotions and moods), and lack of low levels of negative affect (experiencing few unpleasant emotions and moods) [24]. This suggested the symptoms of mental illness such as the experience of depressed mood; problems with energy and motivation and fear and anxiety, is an important aspect of quality of life [25].
According to this structural model, we found that environmental health factors like leisure activities, financial resources and health care facility had the most substantial causal effect on QoL of patients with CMD with path coefficient 0.51 (95%, 0.3, 0.7) , which was larger than the causal effects psychological health, physical health and social relation domain. In Environmental health factor home environment (with loading of 1.3), leisure activities and financial resource (with loading of 1.2) are highly influential items n HRQoL as compared with physical environment and transportation (with loading of 0.9 and 0.93 respectively). This might be due to CMD has great impact on the patients' perceptions and thought that affect them to becomes carless for everything due to they are affected mentally. The other possible reason might be due to the effect of less competitive to do their day to day activity on decision making than other healthy people. This also could be by the effect of workless, due to financial problem and their home and home environments are not comfortable for mentally ill person.
Our finding demonstrated that, among domains of HRQoL, the social relation domain was most affected domain for HRQoL next to environmental health domain.
Similarly, psychological health and social relation was the least affected domain among the CMD patients.
Our results revealed that older age had significant positive association with the social relation domain only among the four domains of HRQoL. This finding is in line with other studies [26-30]. The probable reason may be older ages complained less about their limitations, took solace in religious faith and kept good social relationships [31].
A study done in Germany shown that female gender was related to higher QOL among patients with anxiety and depression [22,28]. However, our investigation showed that gender had no effect on any of the domains of HRQoL. Residence had a negative indirect effect on HRQoL and a negative direct effect on environmental health domain. Common mental disorder patients who live in rural showed lower environmental health, which, in turn, results lower level of HRQoL. Rural areas are characterized by higher unemployment and more severe poverty, as well as lower levels of education, and more difficult access to health and social services [32]. Limitations in resources other than health care in rural settings, such as personal finances, may further restrict access to health care and influence the quality of life of patients [33].
Education status had a direct effect on HRQoL and psychological domain. A higher education level increases psychological health domain, which also contributed to higher HRQoL. This finding is in line with previous studies [22,28,34,35]. This agreement might be due to the fact that higher levels of educational attainment are generally linked to better occupational prospects and higher income, hence having a positive effect on a person's quality of life [36]. On top of this higher levels of education had a positive relationship with higher profits, a healthy nutrition, and general physical and mental care [37].
Furthermore occupational status had a direct effect on both physical health and social relation domain and indirect effect on HRQoL. Other studies reported that Unemployment were found to be significantly associated with low QoL [22,34] this is in line with the finding of the current study. The reason may be because work not only provides people with an adequate amount of money to make ends meet, it also provides individuals with a clear time structure, a sense of identity, social status and integration, and opportunities for personal development [38].
The analysis of our structural model showed that patients with no physical activity had a direct negative effect on psychological health domain and HRQoL. Not doing physical activity worsens HRQoL among CMD patients. This finding is supported by other study [28]. This consistence might be because physical activity contributes to quality of life through the influence of exercise on the onset and progression of disease. Habitual exercisers are less likely than sedentary individuals to develop heart disease, hypertension, diabetes, and some forms of cancer [39] and have a higher QoL as reflected by high levels of vigor, low levels of fatigue, and freedom from health-related restrictions on their daily lives [40,41]. Physical exercise had chronic or long-lasting benefits influence QOL by increasing life-satisfaction and feelings of energy and by decreasing fatigue particularly in people who are clinically anxious or depressed [42].
The finding of the present study also showed that longer duration of follow up (suffering from CMD) for the disease had a negative direct effect and indirect effect on physical health and HRQoL respectively. This finding agreed with previous studies done [29,43]. The agreement may be due to the fact that longer follow up duration are more likely to have an unfavorable prognosis, higher rates of relapse, chronicity of the illness which increases the likelihood of dissatisfaction with their health related QOL [28].
The finding of the present study showed that comorbid condition had a direct effect on physical health domain and both direct and indirect positive effect on HRQoL. Patients with no comorbidities had higher QoL. This was consistent with other studies [34,44-46]. This might be due to the following reasons. One, due to synergistic effects of different chronic conditions on HRQoL [47]. Multimorbidity is associated with increased likelihood of referrals [48], increase costs of care and hospitalization [49]. Second People with comorbid conditions were at greater risk of health problems in mobility, self-care, usual activities, pain/discomfort [50] all these can reduce HRQoL.
In this study, we analyzed the factors that affect the HRQoL of patients with CMD and we constructed a model to identify direct and indirect paths. The Goodness of Fit indices satisfied the recommended levels.
According to this structural model, adults with CMD had poor quality of life in all domains WHOQOL-BREF and overall health-related quality of life. Socio-demographic factors (Age, gender, educational status, residency, payment method for health service and occupation status), clinical factor (comorbid condition and duration of follow up) and physical activity were factors associated with HRQoL among adults with CMD.
AG and AW developed the research protocol and tool, supervised the data collection, managed and analyzed the data, interpreted the findings, and wrote the manuscript.
RE has been involved in research protocol and tool development, trained the data collector, supervised the data collection, managed and analyzed the data, interpreted the findings, and wrote the manuscript.
The authors would like to express special and sincere thanks of gratitude to University of Gondar for the technical support and funding. We are grateful to Saint Amanuel mental specialized hospital for facilitation and support during the study. We also thank all the patients and their attendants who participated in the study.