Urinary tract infections frequently affect pregnant mothers. This problem causes significant morbidity and healthcare expenditure. Three common clinical manifestations of UTIs in pregnancy are: Asymptomatic bacteriuria, acute cystitis and acute pyelonephritis. Escherichia coli remains the most frequent organism isolated in UTIs. Urine culture and sensitivity is the gold standard in diagnosing UTIs.
Objective: A purposive study aims to determine the prevalence of urinary tract infection (UTI) among pregnant women in Tripoli city and determine the sensitivity of isolated organisms to various antibiotics was also examined.
Method: The research sample was taken from laboratory records in private hospitals at Tripoli. Sample of 91 pregnant women at Tripoli city from September -December 2021 was taken (45 for urine routine analysis + 46 for culture and sensitivity test). Information on age, were collected for each woman. Clean midstream urine samples were examined for UTI microscopically and culture, and sensitivity tests were done for the organisms isolated using a range of antibiotics.
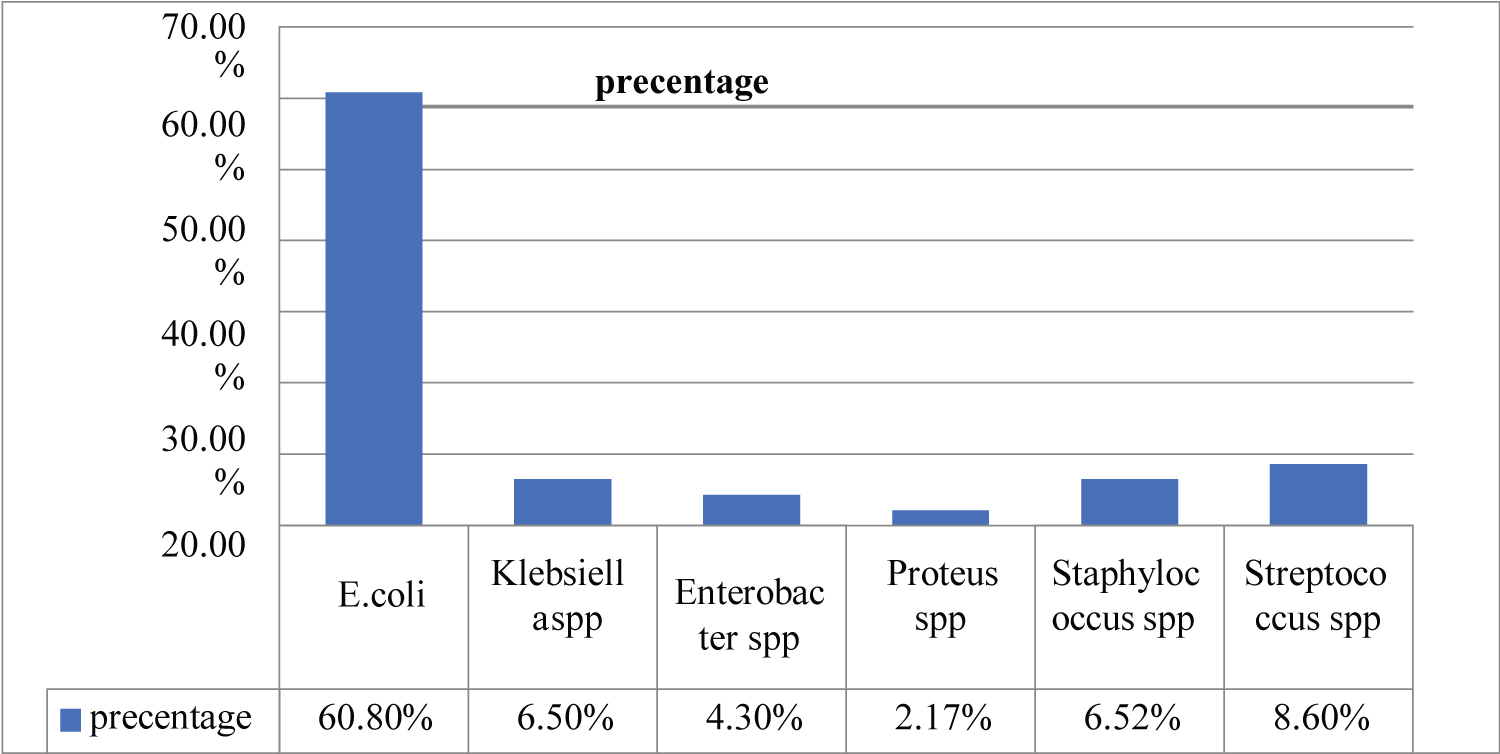
Results: Prevalence rate of UTI among the studied subjects was 37.3%. Escherichia coli was the most frequently isolated organism (60.8%) which was highly resistant to antibiotic.39.13% isolated organism (Staphylococcus spp, Streptococcus spp, Enterobacter spp, Klebsiella spp, Proteus spp).
Conclusion: UTI is still a major health problem among pregnant women. Escherichia coli is the predominant pathogen causing UTI. Urinalyses with culture and sensitivity tests are mandatory for all pregnant women during the different trimesters. Health education with regular antenatal care share greatly in reducing the incidence of this infection. All pregnant mothers should be screened for UTIs in pregnancy and antibiotics should be commenced without delay.
Pregnant, Urinary, Antibiotic, Isolated, Infections
Urinary tract infections (UTIs) are one of the most frequent complications during pregnancy [1]. Traditionally UTI is classified as either involving the lower urinary tract (acute cystitis) or the upper urinary tract (acute pyelonephritis). A predisposing factor or precursor to UTI is bacteriuria.
Asymptomatic bacteriuria is defined as the presence of a positive urine culture in an asymptomatic person and occurs in 2 to 7 percent of all pregnancies [2]. Asymptomatic bacteriuria rates in the pregnant and non-pregnant population are similar, however bacteriuria during pregnancy has a greater tendency to progress to ascending infection than in the nonpregnant woman [3,4]. This is because pregnancy is associated with a rapid increase in progesterone levels which leads to ureteric dilatation and urinary stasis which increases the risk of bacteriuria. Mechanical pressure from the gravid uterus and the physiological changes that occur in pregnancy further increase the risk of asymptomatic bacteriuria and in turn ascending infection [5].
Asymptomatic bacteriuria is associated with an increased risk of adverse fetal outcomes. In particular, an increased risk of preterm birth and an increased risk of delivering a low birth weight infant [6]. Furthermore, studies have also shown that treatment of asymptomatic bacteriuria during pregnancy reduces the incidence of these complications [7]. The prompt recognition and treatment of bacteriuria therefore should limit the risk of progression to ascending infection and the risk of these adverse maternal and fetal outcomes [4].
Asymptomatic bacteriuria is symptomless. Ascending infection may present in pregnancy with lower abdominal pain, frequency, dysuria, haematuria, vomiting or pyrexia and in cases where Pyelonephritis has occurred signs of systemic infection may be present in addition to flank pain (Table 1).
Table 1: Clinical signs and symptoms of urinary tract infections. View Table 1
In severe pyelonephritis there is a significant risk of progression to systemic sepsis and in some cases acute respiratory distress. Untreated pyelonephritis may lead to abscess formation and suppuration (i.e. discharging pus) [8].
In pregnancy urinary frequency is common as the bladder and gravid uterus compete for space in the pelvis. Unfortunately, UTI symptomatology changes in pregnancy and dysuria may not be present. In some cases vomiting may recur or increase in frequency and may be the only indication that infection is present.
Current clinical diagnostic algorithms for the detection of UTI when applied to the pregnant woman have disappointing have low specificity and positive predictive values [9].
UTIs are characterized by the presence of infectious agents in the genito-urinary tract that cannot be explained by contamination. These agents have the potential to invade the tissues of the urinary tract and adjacent structures. The microbiological profile is well known and pathogens such as Escherichia coli have been present in the vast majority of cases [10]. The infection may be limited to the growth of bacteria in the urine (which frequently don’t produce symptoms) or it can result in several syndromes cszv associated with an inflammatory response to the bacterial invasion. Actually, the term UTI represent a wide variety of conditions, including asymptomatic forms of UTIs, urethritis, cystitis, acute pyelonephritis and pyelonephritis with bacteremia or sepsis [11].
There are several classification methods for these infections. In this chapter, we will refer to UTIs as follows:
Asymptomatic bacteriuria is defined as the presence of more than 108 colonies/L of urine, without the symptoms of an acute UTI [12].
Lower tract infection and upper tract infections, according to the anatomical site of contamination [11].
Lower UTIs: The anatomical site of the infection can be the bladder (cystitis) and/or the urethra (urethritis) [11].
Upper UTIs: The kidneys are the anatomical site of the infection (pyelonephritis associated with inflammation of the renal parenchyma, calices and pelvis) [13].
Uncomplicated UTIs: Infections occurring in individuals who lack structural or functional abnormalities of the urinary tract that interfere with the normal flow of urine or voiding mechanism [11].
Complicated urinary tract infections: Infections occurring in individuals with predisposing lesions of the urinary tract that interferes with the normal flow of urine and urinary tract Common causes of predisposing lesions are birth defects, kidney stones, catheters, or obstruction [14]. An UTI during pregnancy is considered complicated. During gestation, untreated UTIs can lead to several pregnancy complications, such as low birth weight infants, premature delivery, and occasionally, stillbirth. Prompt and efficacious treatment of symptomatic UTIs is warranted in pregnant women.
Nevertheless, there is still some controversy regarding the screening and treatment of asymptomatic forms during gestation [15,16].
Given the prevalence and the potential impacts of UTIs on the health of the mother and her child, the objective of this chapter is to cover the most important clinical aspects of the epidemiology, etiology, physiopathology, pregnancy outcomes, and the treatment risks and benefits associated with UTIs during pregnancy.
It is estimated that 2 to 10% of pregnant woman suffer from any form of UTIs (Lee et al., 2008). These infections complicate up to 20% of pregnancies and are responsible for the majority of antepartum admissions to the maternal-fetal medicine units [10].
The prevalence of asymptomatic forms of UTIs has remained constant across countries, and most of the recent observational studies report similar rates, ranging from 2 to 10% - similar to that of nonpregnant women [17]. Acute cystitis is prevalent in 1 to 4% of pregnant women [13].
Despite the relatively low prevalence of pyelonephritis during pregnancy (0.5 to 2%), it is estimated that 20% to 40% of pregnant women with asymptomatic bacteriuria will develop this condition later in gestation [18]. A study showed that if UTI is left untreated, 30% of mothers will develop acute pyelonephritis compared with 1.8% of nonbacteriuric controls. Many studies have reported that pyelonephritis is more common during the second half of pregnancy, with an incidence peak during the last two trimesters of pregnancy. Acute pyelonephritis may lead to adverse outcomes for the baby and the mother, such as premature delivery, low birth weight infants, preeclampsia, hypertension, renal failure and fetal death [19].
The prevalence of UTI in pregnancy is closely related to socioeconomic factors [20]. Predictors of UTIs’ asymptomatic forms include: welfare status, increasing maternal age, multiparity, risky sexual behavior, history of childhood UTIs and history of recurrent UTIs. It has been reported that indigent women have a five-fold greater incidence of bacteriuria than non-indigent populations [20,21]. The prevalence is also markedly increased if women present certain pre-existing medical conditions, such as diabetes mellitus, sickle cell disease, immuno-deficiency states, urinary tract anatomic anomalies, spinal cord injuries and psychiatric illnesses [1].
During Pregnancy it was suggested that UTIs screening and testing algorithms should be designed, incorporating identified risk factors in order to lower overall costs and to improve maternal and infant outcomes [22]. To date, no such algorithm has been prospectively evaluated [12].
In normal physiological circumstances, the genito-urinary tract is sterile. The microorganisms causing UTIs usually originate from the gastro-intestinal flora of the host.
For example, during pregnancy bacteriuria can occur when bacteria from a fecal source gains access to the bladder by ascending the relatively short female urethra [2]. Pathogens causing bacteriuria are similar in both pregnant and non pregnant women [12]. Although virtually every organism can be associated with UTIs, certain organisms predominate as a result of specific virulence and host susceptibility factors [11].
The most common agent implicated in uncomplicated UTIs is Escherichia coli, which accounts for 85% of non-hospital setting infections [6]. Other microorganisms such as Staphylococcus saprophyticus (5% to 15% of cases) [23], Gardnerella vaginalis , Chlamydia trachomatis , Klebsiella pneumoniae , Proteus spp., Pseudomonas aeruginosa, Enterococcus spp . (5% to 10%), Ureaplasma urealyticum and lactobacilli have also been associated with UTIs. Although the clinical significance of these organisms on UTIs during pregnancy was not yet appreciated, a few small studies have reported improved outcomes following therapy against these agents. The consensus is that during gestation, most UTIs are caused by a single organism.
Nevertheless, organisms isolated from pregnant women with complicated UTIs are more varied and generally are more resistant to treatment than those found in uncomplicated infections. Anaerobic and other fastidious microorganisms have been identified in the urine of a large percentage of pregnant women, but the role played by these organisms on adverse perinatal outcomes is unknown.
There is evidence that some bacterial strains can replicate inside the cells, explaining the difficulties in treating some cases, given that these strains are protected from the action of anti-infective drugs. At present, there is no evidence showing advantages in routinely examining the urine for these uncommon organisms.
For many years, pregnancy was seen as a period that naturally predisposes to all forms of UTIs. This was explained by the fact that genito-urinary anatomical and physiological changes induced by gestation predispose women with asymptomatic bacteriuria to develop symptomatic UTIs, leading to the impression that the number of UTIs was higher during this period of life. Nowadays, it is known that gestation itself is not the only responsible for the increased risk of UTIs. Throughout pregnancy, UTIs often persist, owing to re-infection [24].
During gestation the urethra is colonized by bacteria originated from the gastro-intestinal and perineal flora. Other factors that can predispose urethral colonization include the use of some methods of contraception before pregnancy, such as spermicides and diaphragms [24]. Although there is evidence that bladder infections follow colonization of the urethra, the mode of ascent of the microorganisms is not completely elucidated. After reaching the bladder, the organisms quickly multiply and can ascend the ureters to the kidneys. This sequence of events is more likely to occur if reflux of urine into the ureters and kidneys is present.
Bacterial colonization is facilitated as early as the renal pelvis and ureters begin to dilate (eighth week of gestation), and the bladder is displaced superiorly and anteriorly inside the intra-abdominal cavity. Mechanical compression caused by the enlarging uterus is the principle cause of this dilatation, but smooth muscle relaxation induced by progesterone may also play a role. The main consequences of these changes are the decrease in peristalsis of the ureters, followed by an increase in bladder capacity and urinary stasis. It is known that the decreased renal capacity to concentrate urine during pregnancy reduces the antibacterial activity of this fluid, leading it to excrete smaller amounts of potassium and higher amounts of glucose, amino acids and hormone degradation products. These biochemical alterations turn the urine into an alkaline solution, thus providing a suitable environment for bacterial growth [25].
Additionally, the increase in the estrogen induced by gestation, contribute to the adhesion of certain E. coli strains to the type 1 uroepithelial cells [26].
Host protective factors such as the low glucose concentration of the urine, stability of the vaginal lactobacilli population, the influence of estrogens, the activity of Tamm-Horsfall protein, the presence of urinary mucus or slime (called glycosaminoglycan) and the immunologic defense mechanisms, makes the normal urinary tract generally resistant to invasion and efficient in rapidly eliminating microorganisms that reach the bladder [11].
Specific subsets of E. coli clones identified with O, K and H antigens were shown to have increased propensity to cause UTIs. An important virulence factor of bacteria is their ability to adhere to urinary epithelial cells, resulting in colonization of the urinary tract, bladder infections, and pyelonephritis. Uropathogenic E. coli have such virulence factors, known as fimbrias or pilli. These are adherence proteins (adhesins) expressed on the bacterial wall surface that promote binding to the epithelium of the vagina and urethra, thus increasing E. coli ability to cause UTIs [27].
Haemolysin provides E. coli a possible selective advantage by releasing iron from lysed erythrocytes and thus, enhancing pathogenicity by destroying phagocytic and epithelial cells [28].
Current laboratory tests for the diagnosis of UTI are based on the color changes of chemical reactants according to urine composition (dipstick analysis). Two of these are important for their rapidity and low costs: the test of nitrite and the test of leukocyte esterasis. The nitrite test is based on the ability of certain bacteria to reduce the urinary nitrate to nitrite. This test has 50% sensitivity and specificity of 97%, and can result in false positives when used on urine contaminated by normal vaginal bacteria or highly concentrated urine, given that the test follows colorimetric principles. The leukocyte esterase test has low sensitivity and specificity (25%) and can also result in false positives. Both tests have low sensitivity and therefore not suitable as screening tests for diagnosis, unless they are used in combination with other tests [29].
Microscopic urinalysis is the examination of one drop of centrifuged and uncoloured fresh urine, with dry objective (400 times magnification). The observation of any bacteria per field correlates with a urine culture of at least 108 colonies/L of urine. Despite being a low cost test, its low sensitivity limits it to be indicated in the screening of asymptomatic bacteriuria [29]. Current evidence seems to indicate that the microscopic analysis of a Gram-colored urine sample is a more suitable and rapid test for UTI screening. It consists in the microscopic observation of the urine bacteria Gram stain, improving the accuracy of microscopic urinalysis [17].
Several alternative laboratory methods can be used for the diagnosis of UTIs with varying sensitivities and specificities. Therefore, the association of these tests can be necessary to confirm the positive results of a urinalysis. Moreover, for their meaningfull interpretation, it become imperative to use correct techniques for collecting the urine sample (aseptic perineal urine midstream, immediate transportation and refrigeration at 4 °C for, no later than 24 hours) [30].
Among the abnormalities likely to be detected in a urinalysis, we can find pyuria, hematuria, proteinuria and cylinders in the urinary sediment. These findings can indicate UTI, but actually they are just signs of inflammation and may also be present in other conditions. It should be remembered that a normal urinalysis result does not exclude the diagnosis of UTI, hence, not being ideal for screening of asymptomatic bacteriuria during pregnancy. However, in symptomatic patients, the result of this test is accepted for the initiation of therapy until the results of urine microbiologic culture are known [17,30].
The urine microbiologic culture is considered the gold standard for laboratory diagnosis of UTI. It is the most accurate method to identify and quantify bacteria in the urine with high sensibility. Its drawbacks are the relatively higher costs, the long time needed to achieve the number of bacterial colonies necessary for a sensitive result and the need for professionals and laboratories qualified for its elaboration. The correct interpretation of a urine culture is crucial for therapeutic success. In asymptomatic cases, the finding of more than 108 colonies/L of urine suggests infection.
Values between 107 and 108 correspond to infection in 50% of cases. If the urine is collected by bladder catheterization, the finding of values above 106 indicates infection; if the urine is issued by suprapubic aspiration, infection is diagnosed with any number of bacteria. In symptomatic cases, urine cultures are considered positive with up to 105 bacteria/mL of urine [30].
A purposive study aims to determine the prevalence of urinary tract infection (UTI) among pregnant women at Tripoli city and determine the sensitivity of isolated organisms to various antibiotics was also examined.
The research procedure included the following:
Research sample: The research sample was taken from laboratory records in private hospitals at Sample of 91 pregnant women in Tripoli city from September-December 2021 was taken (45 for urine routine analysis + 46 for culture and sensitivity test). Information on age, were collected for each woman. Clean midstream urine samples were examined for UTI microscopically and culture, and sensitivity tests were done for the organisms isolated using a range of antibiotics.
Research method: Clean catch midstream urine was collected from the studied sample in sterile bottles. General urine examination was carried out for each woman. Accordingly, for the infected women, urine culture and sensitivity test was Plates of blood agar and Macconcky medium were aseptically inoculated with 2-3 drops of the urine precipitate and then incubated for 24-48 hours and sensitivity tests were done for the organisms isolated using a range of antibiotics.
Prevalence rate of UTI among the studied subjects was 37.3%. Eschirishia coli was the most frequently isolated organism (60.8%). 39.13% isolated organism ( Staphylococcus spp , Streptococcus spp , Enterobacter spp , Klebsiella spp, Proteus spp ). Most of the isolates were resistant to at least five antibiotics, and multiple drug resistance was observed in E. coli isolates. A high degree of resistance was seen against ciprofloxacin, amoxicillin and cefuroxime (Table 2).
Table 2: Culture and sensitivity cases. View Table 2
By Jennifer Le University of California, San Diego December 2004, UTIs are the most common bacterial infections during pregnancy. They are characterized by the presence of significant bacteria anywhere along the urinary tract. Enterobacteriaceae account for 90% of UTIs. The common antibiotics used are nitrofurantoin, cefazolin, cephalexin, ceftriaxone, and gentamicin. Sivalingam Nalliah International Medical University (IMU) August 2007, Urinary tract infections frequently affect pregnant mothers. This problem causes significant morbidity and healthcare expenditure. Three common clinical manifestations of UTIs in pregnancy are: asymptomatic bacteriuria, acute cystitis and acute pyelonephritis. Escherichia coli remains the most frequent organism isolated in UTIs.
Urinary tract infections (UTIs) are one of the most common medical complications of [23]. It is estimated that one in three women of childbearing age will have a UTI [17]. Because of the normal physiologic changes induced by gestation, pregnant women are especially susceptible to these infections.
By Jennifer Le University of California, San Diego December 2004, UTIs are the most common bacterial infections during pregnancy. They are characterized by the presence of significant bacteria anywhere along the urinary tract. Enterobacteriaceae account for 90% of UTIs. The common antibiotics used are nitrofurantoin, cefazolin, cephalexin, ceftriaxone, and gentamicin. Sivalingam Nalliah International Medical University (IMU) August 2007, Urinary tract infections frequently affect pregnant mothers. This problem causes significant morbidity and healthcare expenditure. Three common clinical manifestations of UTIs in pregnancy are: Asymptomatic bacteriuria, acute cystitis and acute pyelonephritis. Escherichia coli remains the most frequent organism isolated in UTIs.
UTIs are the widely spread infections seen in hospital settings, and the second commonest infections seen in the general population.
It is concluded that UTI is still a major health problem among pregnant women. Escherichia coli is the predominant pathogen causing UTI. Urinalyses with culture and sensitivity tests are mandatory for all pregnant women during the different trimesters. Health education with regular antenatal care share greatly in reducing the incidence of this infection.