Spontaneous dissection of the coronary artery (SCAD) is an uncommon cause of acute coronary syndrome (ACS) and is defined as a dissection of the coronary artery not associated with an atherosclerotic process, plaque rupture and/or thrombus formation and, by definition, not iatrogenic. The resulting myocardial damage is determined not by the rupture of a plaque indeed, but by the formation of an intramural hematoma (IMH) or intimal/medial disruption that determines the dissection of the arterial wall with the formation of a false lumen that obstructs the blood flow through the true lumen. SCAD can represent up to 4% of the total ACS according several casuistry [1].
The population most affected by the SCAD is the female one, representing, in fact, up to 35% of all myocardial infarction (MI) in women aged ≤ 50 years and also is the main cause of MI associated with the pregnancy [2]. SCAD is a condition often underdiagnosed for several reasons, such as the young age of the patients on average, the low presence of classic cardiovascular risk factors, the poor level of knowledge of this entity by physicians and the limitations of classical hallmarks for coronary artery dissection during angiography [1] causing flow deficits in the coronary arteries and therefore MI [3].
Two main theories of how a spontaneous dissection develops have been described, the first one suggests that primum movens is the formation of an interruption in the arterial wall (intimal tear), which causes blood to come out of the true lumen to create a false lumen. The second theory predicts that primum movens is a spontaneous hemorrhage from the vasa vasorum that starts the dissection process [4,5]. The presence of an inflammatory cellular infiltrate was also noted around the spontaneous dissection that could be useful in the post-mortem diagnosis to distinguish between spontaneous and iatrogenic dissections [3].
SCAD is a multifactorial disease, with a poor predominance of traditional risk factors. Predisposing factors are female gender, pregnancy, age < 50 years, female sex hormones, other arteriopathies, such as fibromuscular dysplasia (FMD) that represents the most commonly extracoronary arterial disease associated. FMD is a non-atherosclerotic and non-inflammatory vascular disease that can affect any part of the arterial bed and has a very varied manifestation (arterial stenosis, aneurysm, tortuosity, or dissection) [6].
Probable triggers of SCAD, in a predisposing patient, are emotional/physical stress, intense isometric exercise, and weightlifting [7].
Clinical manifestations of SCAD include ACS (26% to 87% of patients with SCAD presents an ST-segment elevation MI), ventricular arrhythmias or sudden cardiac death [8,9].
Regarding the management of SCAD, despite the substantial difference between ACS caused by SCAD compared to those based on atherosclerosis in the field of pathogenesis, response to the medical therapy and revascularization, no randomized studies or comparisons have been performed between these strategies in ACS caused by SCAD [1].
From the point of view of the angiographic manifestation, several contemporary coronary angiography series show that the classical pathognomonic characteristics of artery dissection (presence of multiple radiolucent lumens and contrast extra luminal staining) are present only in a reduced percentage of SCADs. Therefore, for greater clarity, we report a recent proposal for angiographic classification of SCAD (Figure 1) [10]. With these premises, as an angiography supplement, intravascular imaging is a very useful means of diagnosing SCAD. In our experience, we prefer to use OCT more than IVUS. In fact, OCT improves the possibility of making a diagnosis and, in our opinion, is the intravascular imaging of the first choice in doubtful cases [11]. OCT has a spatial resolution ranging from 10 to 20 μm and is therefore superior to IVUS in delimiting the lumen-intimal interface and discriminating true lumen, false lumen, intimal tear, and intraluminal thrombi.
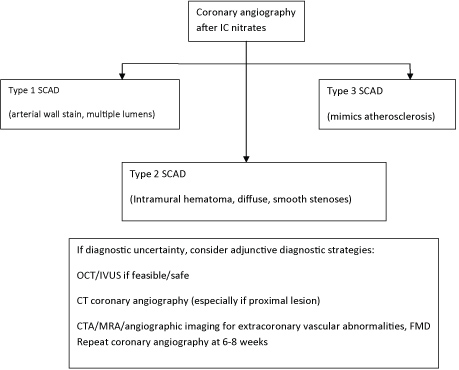 Figure 1: Algorithm for diagnosis of spontaneous coronary artery dissection (SCAD) in the setting of acute coronary syndrome [1].
View Figure 1
Figure 1: Algorithm for diagnosis of spontaneous coronary artery dissection (SCAD) in the setting of acute coronary syndrome [1].
View Figure 1
According to the difficulty of angiographic SCAD diagnosis, we proposed a clinical-angiographic score system, previously worked out by our group (Figure 2). In presence of a patient with chest pain, ECG/Echo-abnormalities or a rise/fall in troponin, if at least three points are gained it's advisable to perform an intracoronary imaging (OCT as the first choice or, if unavailable, IVUS) to detect a suspected SCAD [12-15].
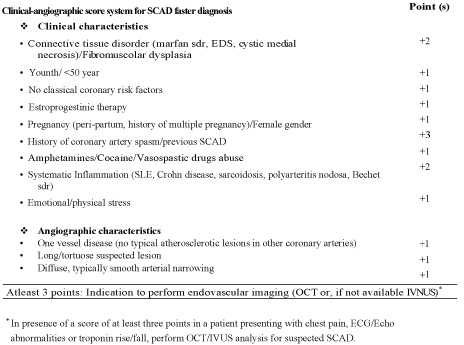 Figure 2: Clinical-angiographic score system for SCAD faster diagnosis [12].
View Figure 2
Figure 2: Clinical-angiographic score system for SCAD faster diagnosis [12].
View Figure 2
If a SCAD diagnosis is confirmed, recent American heart association (AHA) guidelines suggest an algorithm for management of this condition, based at first on clinically stability/instability of patient and also according on the coronary arteries anatomy (Figure 3). Thus, in a patient with a diagnosis of SCAD, clinically stable with no high-risk anatomy, a conservative therapy is reasonable, monitoring as an inpatient for 3-5 days [1]. In fact, the majority of cases of SCAD goes to spontaneous healing generally within a months, moreover, percutaneous coronary intervention (PCI) in these cases has a lower yield than ACS on atherosclerotic basis, due to a greater technical difficulty due to the fragility of the arteries and to the possible interaction between the metal stents and IMH after the natural reabsorption of the latter [16]. Conservative management consists of medical therapy, based on ACE-I, B-blockers, statins, an antianginal drugs if necessary, dual antiplatelet therapy (DAPT) [17], also if there is little evidence regarding the duration of DAPT in patients with SCAD that don't undergo percutaneous revascularization.
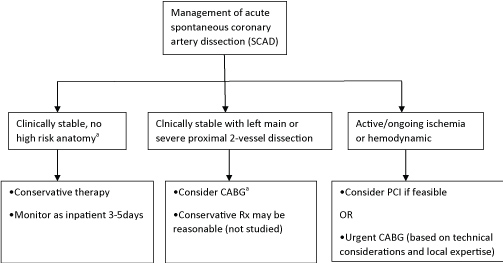 Figure 3: Algorithm for management of acute spontaneous coronary artery dissection [1].
View Figure 3
Figure 3: Algorithm for management of acute spontaneous coronary artery dissection [1].
View Figure 3
If there is a high risk-anatomy, like the left main coronary artery (LMCA) involvement or several proximal two-vessel dissections, and the patient is clinically stable, the proposed strategy is to perform a CABG, according to also with the new guidelines for myocardial revascularization [18].
Finally, if a patient is unstable and there is ongoing ischemia, PCI should be considered, based on the case and coronary anatomy [1].
In cases where PCI is needed, our approach is to prefer the use of a bioresorbable scaffold (BRS), which have proven effective and safe in our experience [19] and in a cohort analysis of 18 patients [20]. Although despite these intriguing findings, larger studies will be needed in the future.
Patients with SCAD require after hospitalization a clinical follow-up at 1, 3, 6 and 12 months. In cases where symptoms should reoccur, it is advisable to repeat an invasive re-evaluation [12]. In fact, in a series of the year 2012, the risk of relapse, with a median of 2.8 years in the second episode, was 17%, with an estimated 10-year rate of MACEs (death, heart failure, myocardial infarction, and SCAD recurrence) of 47% [16].
It is increasingly clear that the SCAD is a clinical entity, albeit uncommon, to be kept in close consideration especially in the youth and female who present with ACS without the traditional risk factors. The effort of the scientific community, as evidenced by the review published by the AHA in 2018, is aimed at reducing more and more the lack of diagnosis and providing guidance in the management of this condition which still today has shady areas.