Diabetes bullosis is a chronic manifestation, a specific cutaneous marker, of diabetes mellitus essentially insulin-dependent. It is very rare. Its etiology is still unknown. It is seen more frequently in long-standing diabetic patients commonly with peripheral neuropathy, retinopathy, or nephropathy. The lesions are usually asymptomatic. There are no specific tests for DB. The diagnosis is based on characteristic findings, clinical course, and the exclusion of other bullous disorders. Its evolution is benign; the treatment is not specified. Its management remains essentially preventive.
Diabetes mellitus, Bullous eruption, Fusidic acid
DB: Bullosis Diabeticorum
Diabetes mellitus affects an estimated 26 million people in the United States; the epidemic is growing and has been projected to double by 2050 [1].
Diabetes bullous is a chronic manifestation, a specific cutaneous marker, of diabetes mellitus essentially insulin-dependent. It is a rare bullous dermatosis. In the literature, about 100 cases are described [2].
It is a spontaneous, non-inflammatory, blistering condition of unknown etiology [3].
It was first described by Kramer in 1930.In 1967, Cantwell & Martz1 introduced the term ‘bullosis diabeticorum’ [4].
We present a case of bullosis diabeticorum on the trunk of a female patient.
A 70-years-old woman with a medical history of uncontrolled diabetes mellitus was admitted to neurological service for suspicion of neurosyphilis.
On physical examination, she had ablister, non-tender, tense, large, measuring 4 × 3 cm, filled with clear sterile serous fluid, based on the trunk, developed spontaneously overnight without any preceding trauma or friction to the area (Figure 1 and Figure 2).
 Figure 1: Post-bullous erosion located on the left flank.
View Figure 1
Figure 1: Post-bullous erosion located on the left flank.
View Figure 1
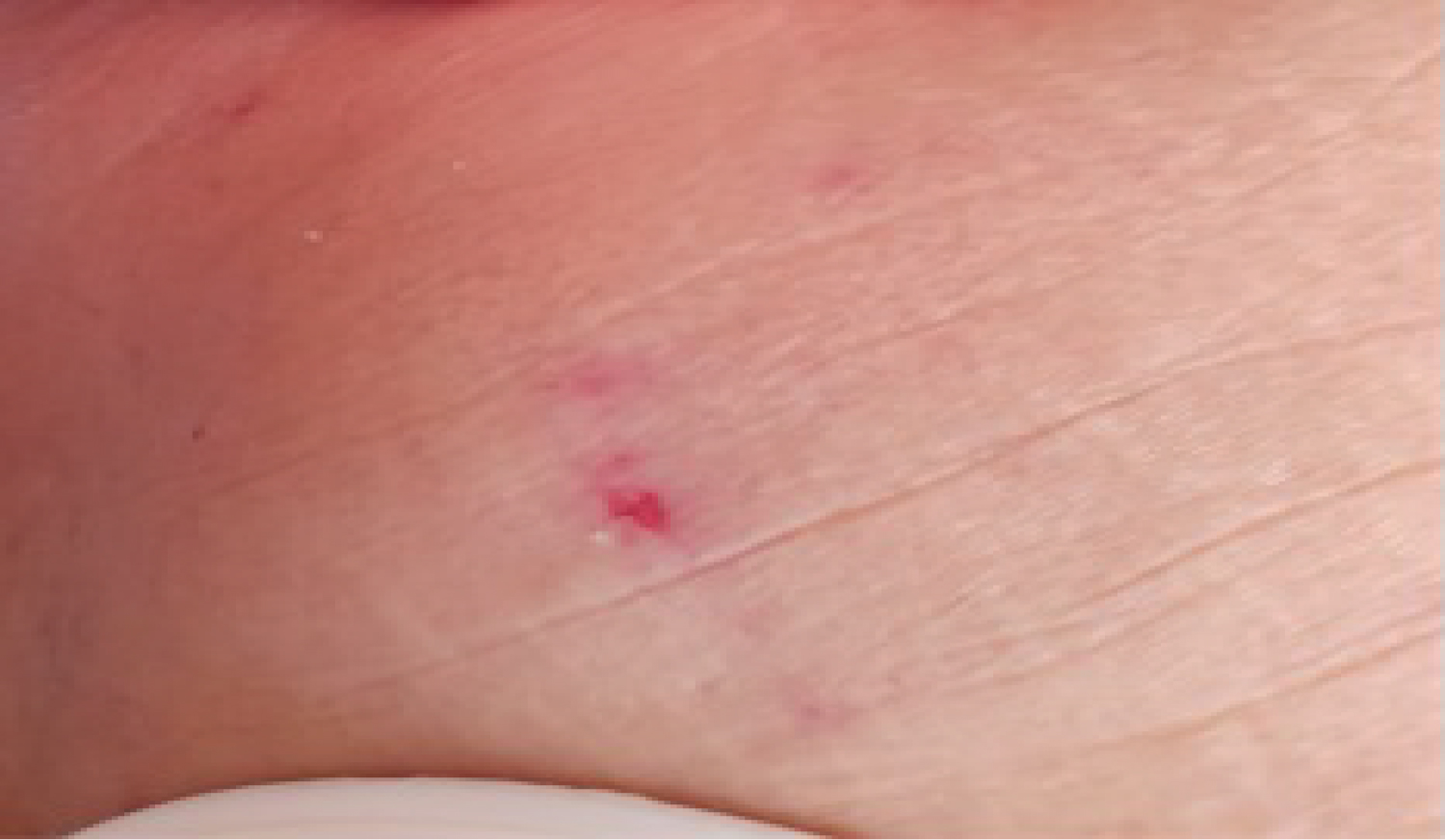 Figure 2: Post-bullous erosion located on the left flank.
View Figure 2
Figure 2: Post-bullous erosion located on the left flank.
View Figure 2
The bullae arise from a non-inflamed base, without erythema or edema perilesional. There was just a little pain. Aspiration was not attempted to avoid secondary infection.
2 days later, they rupture leaving a superficial painless ulcer.
Biopsy shows a subepidermal bulla. The epidermis of normal height with a skin covering lined with a thickened orthokeratotic stratum corneum centered by an excoriation made up of a fibrinoid leukocyte block made up of some apoptotic cells; the underlying dermis is oedematous congestive shelters a minimal inflammatory infiltrate made up of scattered mature lymphocytes and some neutrophils.
Direct immune fluorescence was negative.
The ulcers were compressed 2 times a day with a fusidic acid topical cream 2 weeks after presentation, the patient reported that the lesions were healing on therapy.
On the follow-up visits, it was recurrence of multiple bullae located on the lower back and right buttock; having benefited from the same treatment (Figure 3 and Figure 4).
 Figure 3: Multiple Bullae located at the level of the right buttock.
View Figure 3
Figure 3: Multiple Bullae located at the level of the right buttock.
View Figure 3
 Figure 4: Multiple Bullae located at the back.
View Figure 4
Figure 4: Multiple Bullae located at the back.
View Figure 4
According to various studies, 30% to 90% of diabetic patients experience at least 1 dermatologic complication [1].
The exact prevalence of bullosis diabeticorum is still unknown, it involves approximately 0.2% to 0.5% of patients [5].
The male to female q ratio is 2:1 and the age of onset ranges from 17 to 84 years with a mean age of 55 years. [4].
Despite the poorly understood cause of DB, numerous mechanisms have been proposed, including minor trauma-induced blister formation, hypoglycemia or highly fluctuating blood glucose levels, microangiopathy, neuropathy, alterations in calcium or magnesium metabolism, UV exposure, an autoimmune phenomenon, and vascular insufficiency [1].
It is seen more frequently in long-standing diabetic patients commonly with peripheral neuropathy, retinopathy, or nephropathy [4].
The most common location in the decreasing order, are the feet, distal legs, hands, and forearms, but nonacral sites may also be involved like the trunk [4,6].
The lesions are usually asymptomatic, they often overnight they are tense and vary in diameter from 0.5 to several Centimeters [4].
There are no specific tests for DB [1].
The diagnosis is based on characteristic findings, clinical course, and the exclusion of other bullous disorders, such as bullous fixed drug reaction, immunobullous disease like bullous pemphigoid, friction blisters; epidermolysis bullosa acquisita and porphyria cutanea tarda, and pseudoporphyria associated with dialysis and medications [3,5].
The histological finding is heterogeneous [3]. The microscopic findings reveal 2 major groups with different levels of cleavage, suggesting different stages of development or even separate pathogenetic mechanisms: The first and most common group shows intraepidermal or subepidermal cleavage at the level of the lamina Lucida, without acantholysis. These lesions usually resolve spontaneously without scarring and are epithelialized early. By contrast, in the second type, cleavage is below the dermo-epidermal junction with the destruction of anchoring fibrils. This type heals with scarring and atrophy [1].
Direct immunofluorescence is usually negative although one report described an IgM and C3 deposits within dermal blood vessel Wald [4].
Although most DB heals in 2 to 6 weeks without treatment, the course is not always smooth. Secondary infection or ulceration, particularly associated with blisters on the foot, may lead to osteomyelitis, large areas of necrosis and scarring, as well as toe amputation. Healing may be as long as 2 years [1].
The prognosis is normally good [5].
The treatment is not specified focused on skin protection and preventing secondary infection. Immediate regulation of the blood glucose level has been recommended as a result of the finding that hypoglycemic episodes often precede eruptions regular wound cares with antibiotics helped in some cases [1,4].
Uncomplicated blisters should be left intact, but the sterile aspiration of fluid may prevent rupture in some cases. For Ulcerated blisters, she should be treated with aggressive wound management [1].
The bullosis diabeticorum is a specific skin complication of diabetes. Its pathophysiology not fully understood. Its evolution is normally benign, and its therapeutic management remains essentially local [7].
It is still a rare yet well-documented condition [6]. This infrequency with witch is, it encountered, makes it a diagnostic challenge for dermatologists [3].