A 29-year-old man with a history of bulbar ulcer treated 2 years previously and chronic smoking at 13 packs/year was hospitalized for respiratory symptoms made up of right basithoracic pain with cough and clear sputum without fever or progressive night sweats for six months in a context of deterioration in general condition. The clinical examination was unremarkable. On the biological assessment, there was a slight inflammatory syndrome with sedimentation rate at 29 mm in the first hour and CRP at 9.8 mg/l, the blood count was normal, as were the liver and kidney assessments and the viral serologies (HBV, HCV and HIV) were negative. The search for mycobacterium tuberculosis in sputum and by gastric tube was negative on three occasions and the Quantiferon was at 2.70 IU/ml (2xN). The chest X-ray showed opacity in the apical segment of the right upper lobe. Complementary CT scan revealed significant right apical mass with alveolar condensation, pleural connections and adjacent micronodules strongly suspecting a tumor or infectious localization (Figure 1 and Figure 2). A transparietal biopsy was then performed.
Diagnosis of Caseo-follicular pulmonary tuberculosis was made and Antibacillary treatment was introduced with good clinical and radiological evolution.
Despite the positivity of the quantiferon, the atypical clinical and radiological presentation did not allow the diagnosis of pulmonary tuberculosis to be retained. The use of CT-guided biopsy was then necessary and revealed a granulomatous and follicular inflammatory process with caseous necrosis, without lesion suspicious of malignancy.
Pseudotumoral pulmonary tuberculosis is a rare form of tuberculosis in the immunocompetent [1,2]. Its frequency would be 3 to 5% according to most series [1,3]. This presentation can simulate bronchopulmonary cancer, especially when bacilloscopy is negative. It thus poses diagnostic difficulties since in the majority of the cases described, the clinical symptoms are non-specific [3], the most often negative bacteriological samples related to the solid and poorly oxygenated character of the pseudotumoral tuberculosis lesions [3], the CT appearance rather suggestive of a tumor lesion (convex edges, spiculated limits, pleural attachments) [3] and the biopsy samples that are often difficult to perform in forms without endobronchial lesion. These difficulties are at the origin of a delay in diagnosis which would be 30 to 70 days depending on the series [1,3]. The treatment remains classic and is based on antibacillary drugs at the usual dosages and durations [4]. The evolution is favorable in the majority of cases and few complications are reported [3,4].
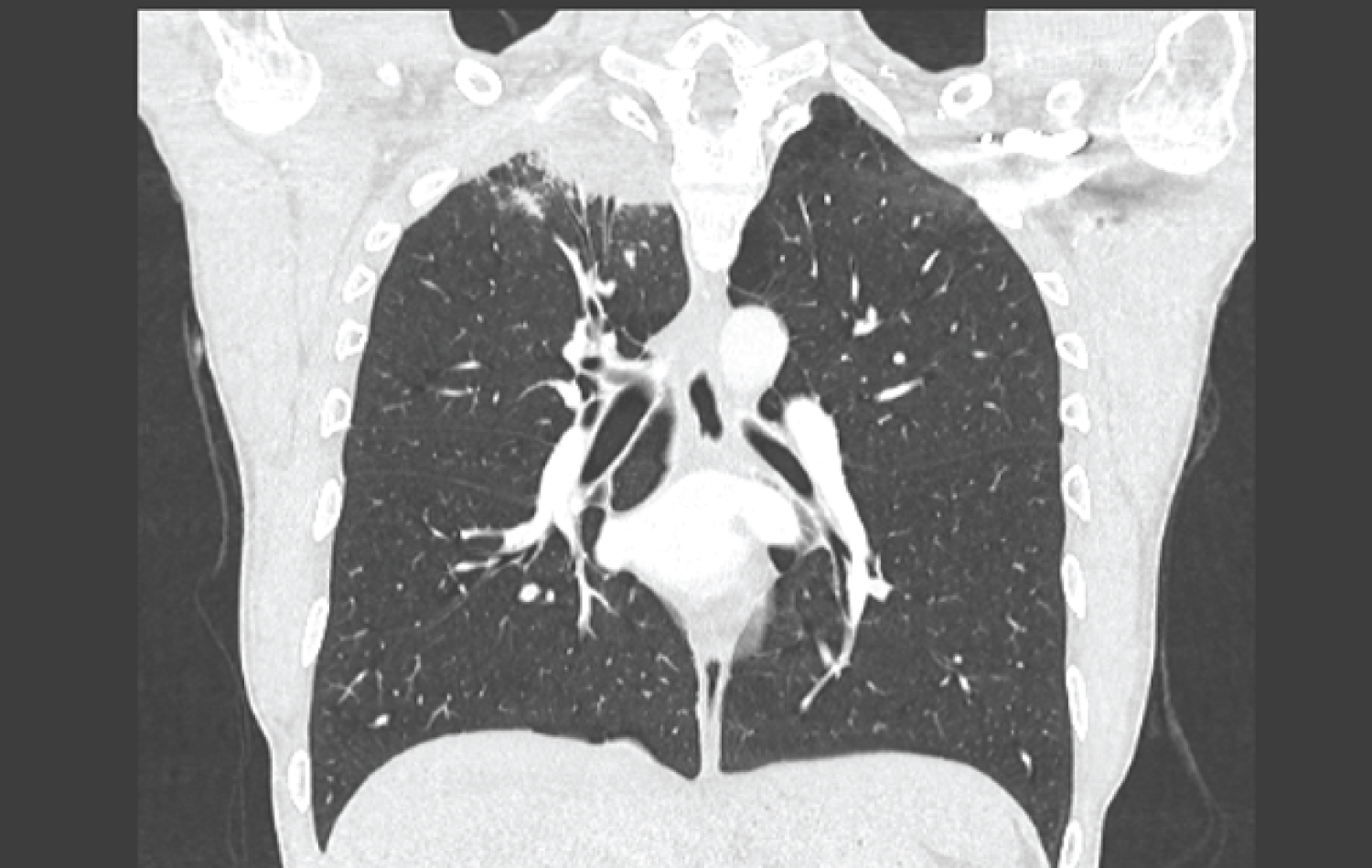
Figure 1: Coronal thoracic CT section showing right apical lung mass.

Figure 2: Thoracic sagittal CT section showing the apical lung mass.
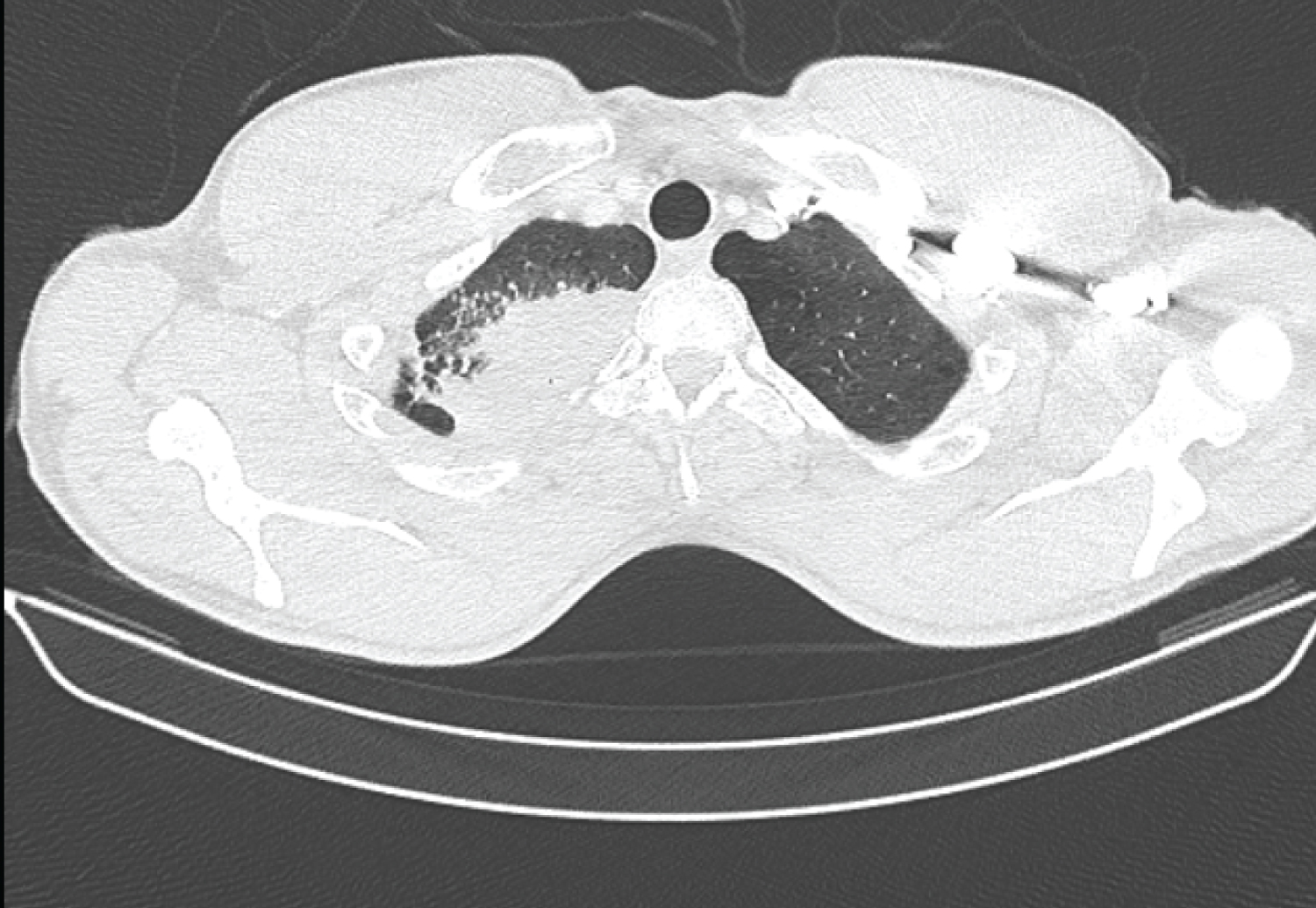
Figure 3: Thoracic cross-sectional CT scan showing the right apical lung mass with alveolar condensation, pleural connections and adjacent micronodules.