Umbilicus, Seborrheic keratosis, Dermoscopy, Dermatopathology
Seborrheic keratosis is one of the most common skin tumors. It most often presents as a light brown to brown nodule with a papillomatous or squamous surface. However, it may vary in color and shape and can thus resemble the pattern of other skin tumors. We report the case of an atypical seborrheic keratosis located at the umbilicus with misleading dermoscopy.
We report the case of a 34-year-old female patient with a medical history of schizophrenia on antipsychotic medication. She presented to our department with an asymptomatic growing lesion of the umbilicus of two years duration. The examination revealed a keratosicoval nodule measuring 15 × 16 mm, of heterogeneous color (Figure 1). Subsequent dermoscopy revealed exophytic keratotic projection pattern with dotted vessels, brown and yellowish structure less areas and aggregated blue-gray globular-like structures (Figure 2).
Complete excision was performed. Anatomopathological examination objected well-limited exophytic lesion made of an epidermal proliferation with a hyperplastic epidermis surmounted by a layer of orthokeratotic and papillomatous keratin with a proliferation made mainly of epidermal basal cells (Figure 3). Numerous horny inclusion cysts were associated. The diagnosis of seborrheic keratosis was retained.
Seborrheic keratosis is one of the most common skin tumors [1]. The etiology is still unclear but advanced age and exposure to radiation may be contributing factors [2]. It most often presents as a light brown to brown nodule with a papillomatous or squamous surface [1]. However, it may vary in color and shape and can thus resemble the pattern of other skin tumors. On our case, the dermoscopy was misleading as we didn't note the presence of milia-like cysts or comedo-like opening that are characteristic of seborrheic keratosis. The main differential diagnoses were squamous cell carcinoma, skin metastasis and omphalolith. It is the anatomopathological examination that allowed to re-establish the diagnosis. Histology remains the gold standard.
None disclosed.

Figure 1: Keratosic oval nodule measuring 15 × 16 mm of heterogeneous color located on the umbilicus.
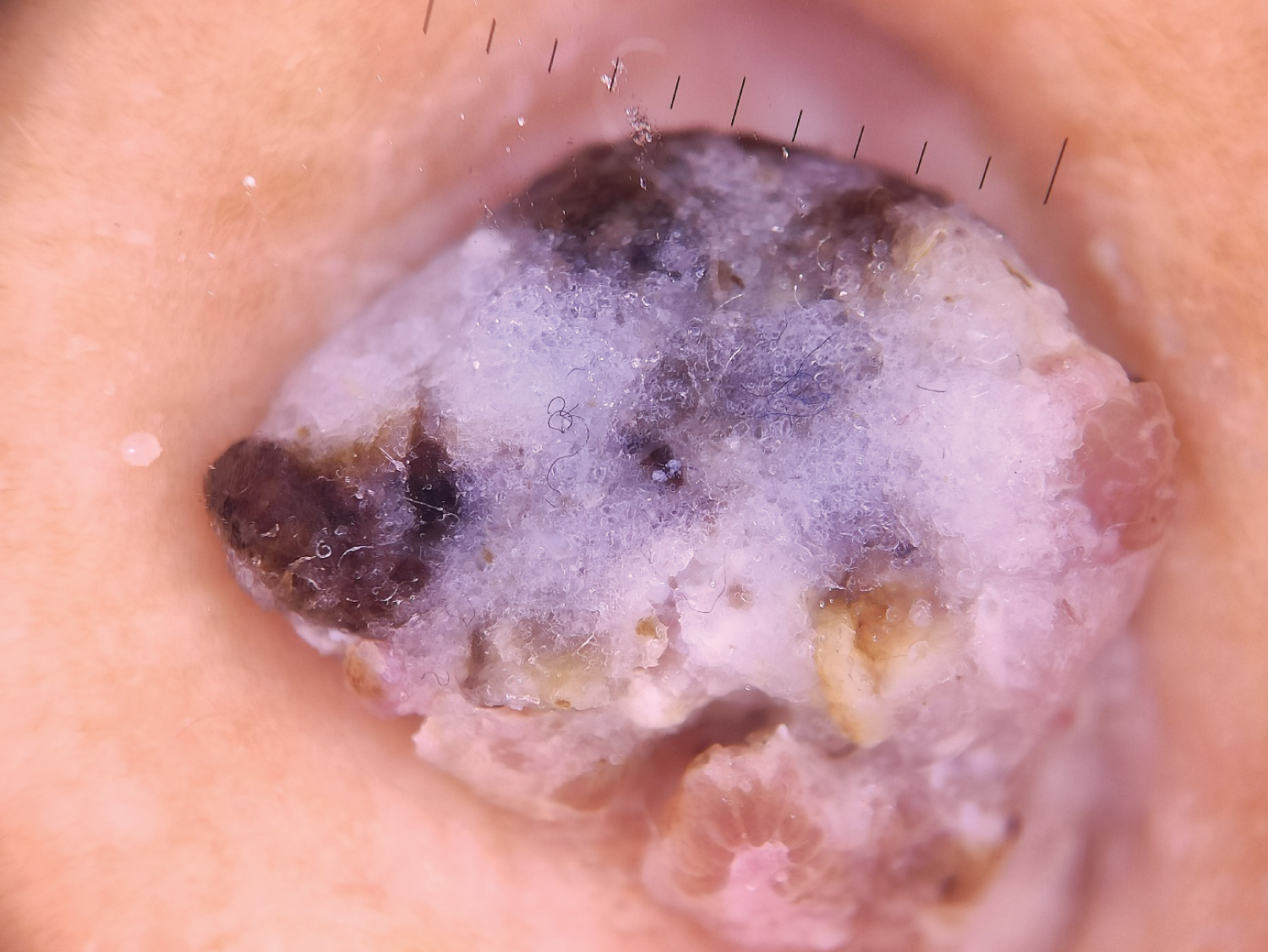
Figure 2: Dermoscopy of the nodule showing exophytic keratotic projection pattern with dotted vessels, brown and yellowish structureless areas and aggregated blue-gray globular-like structures.
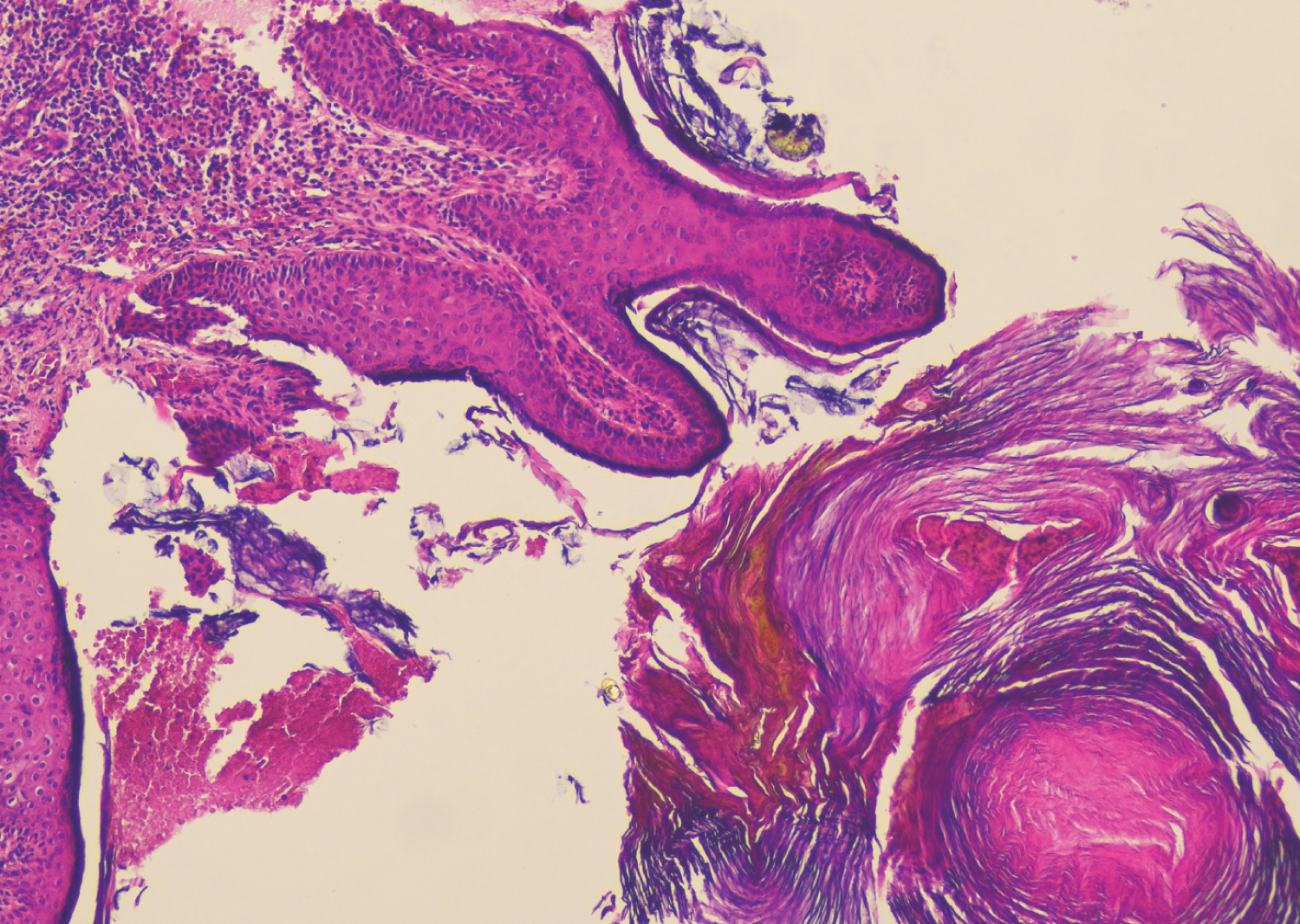
Figure 3: Histology showing an epidermal proliferation with a hyperplastic epidermis surmounted by a layer of orthokeratotic and papillomatous keratin with a proliferation made mainly of epidermal basal cells.