Infection, Renal cyst
Renal cysts are relatively common, increasing in prevalence with age [1-3]. They are usually benign and asymptomatic, with their diagnosis being incidental on imaging exams. In some cases, however, they can reach large dimensions, leading to symptoms and/or complications [3,4].
An 80-year-old woman with a history of metabolic syndrome, ischemic heart and cerebrovascular disease was admitted at the emergency department with asthenia and left abdominal and flank pain. She was on day 5th of empiric cefuroxime for urinary tract infection. On physical examination, the patient was febrile, but hemodynamically stable; an abdominal mass in the left flank was evident and painful on deep palpation; ipsilateral Murphy's sign was present. Laboratory studies showed a marked elevation of C-reactive protein (329.9 mg/L), normal renal function, and mild isolated leukocyturia (70/µL) on urinalysis. A contrast-enhanced abdominal-pelvic computed tomography scan revealed an enlarged left kidney conditioned by a multiloculated cystic lesion (14 × 11 mm in the axial plane; 21 mm in the longitudinal plane), with homogeneous content and regular parietal thickening, associated to heterogeneous densification of the left perirenal fat, without hydronephrosis (Figure 1). In the absence of unequivocal findings of complicated cyst, the diagnosis of acute pyelonephritis with failure to cephalosporin therapy (no prior urine culture) was assumed, and piperacillin/tazobactam was started. However, since the patient maintained persistent fever and elevated inflammatory markers, the possibility of occult cyst infection was considered. Thus, a percutaneous approach was performed with immediate drainage of 1500 mL of purulent content. Multisensitive K. pneumoniae and E. coli were isolated in the cystic fluid, and the antibiotic spectrum was narrowed to cefuroxime, according to the antibiogram, and drainage of the cyst was maintained through a pigtail drain (Figure 2). She evolved favorably, having completed 1 month of antibiotic and subsequently referred to Urology consultation for a potential nephrectomy.
Renal cyst infection is a rare complication, accounting for only 2.5% of all events [5]. The clinical presentation and imaging findings are nonspecific, making diagnosis challenging. Antibiotic therapy is the first-line treatment; however, radiologic or surgical intervention may be necessary.
The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
None declared.
CPF was involved in drafting the article. AMT and SF were involved in revising the article critically for important intellectual content. All authors read and approved the final manuscript.
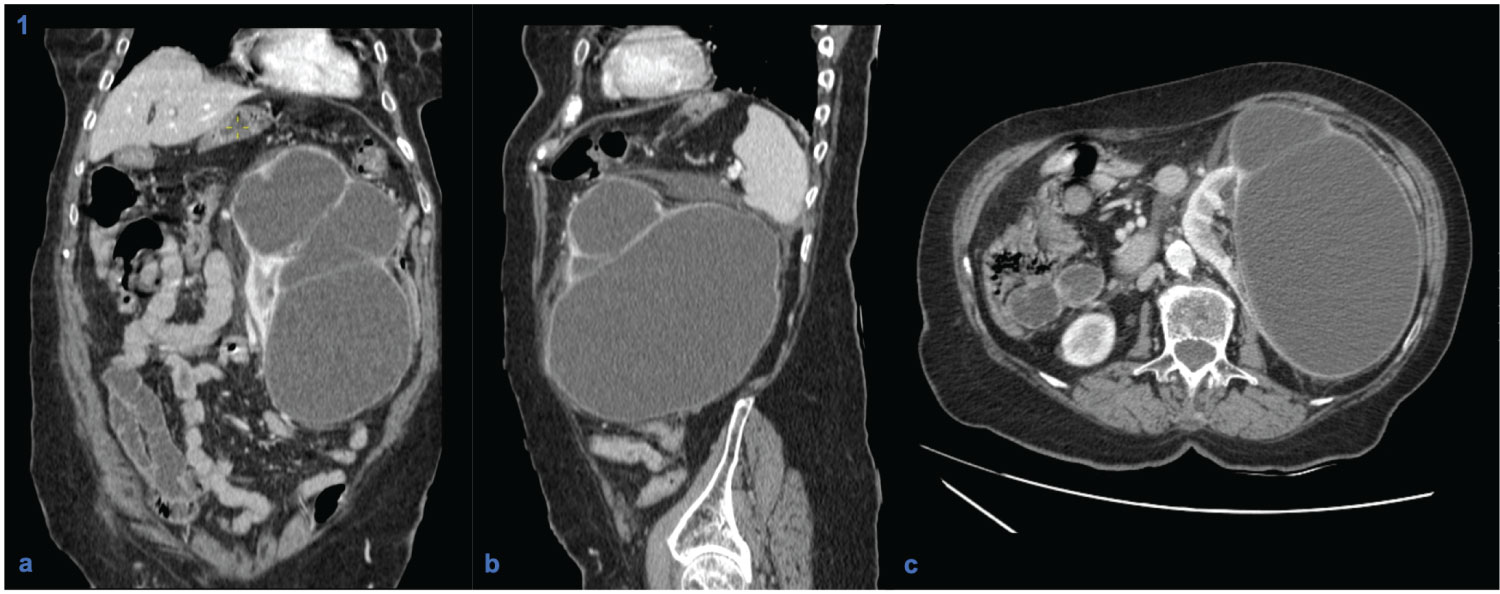
Figure 1: Contrast-enhanced computed tomography scans (coronal (a), sagittal (b) and axial (c) planes), showing a multi-septated cystic lesion in the left kidney with wall enhancement and water-like density content, without contact with the excretory system.
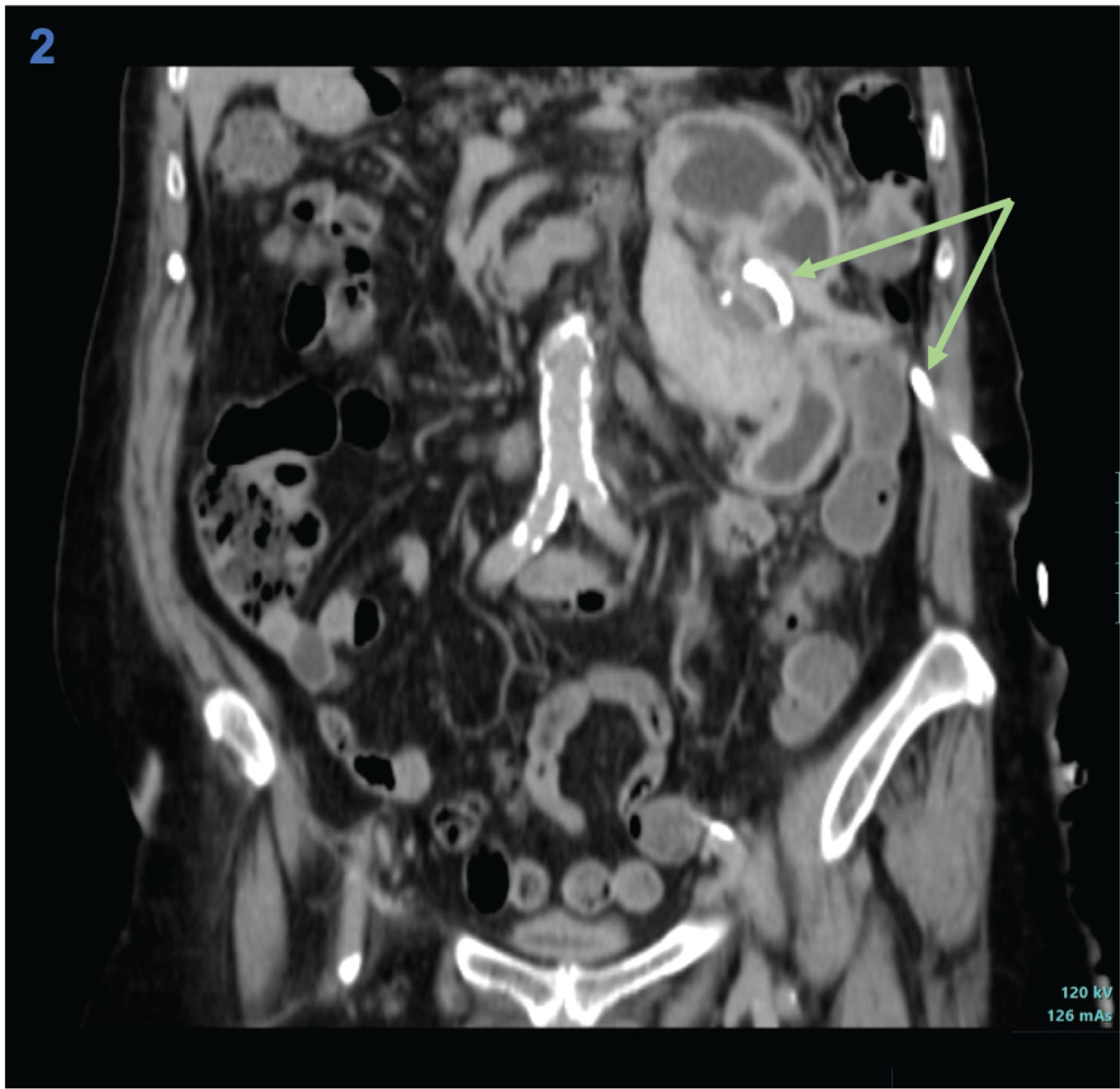
Figure 2: Coronal section of contrast-enhanced computed tomography scan after percutaneous drainage of the left renal cyst, revealing collapse of the cystic structure and drain inside (arrows).