Bladder stones, Urinary bladder calculi, Cystolithotomy, Prostate, Prostate protrusion
The incidence of bladder stones in Western countries is relatively low, most commonly found in developing countries due primarily to dietary factors. The most affected areas are the countries of the Middle East, North Africa and Thailand, Indonesia and Myanmar [1]. We report the case of a 73-years-old patient, followed For Low Urinary Tract Symptoms (LUTS) treated by alpha-blocker complicated by acute urinary retention and finally carrier of a vesical catheter. The ultrasound exploration showed a prostate enlargement which volume was estimate to 60g with intravesical prostate protrusion. In the bladder was the presence of multiple stones.
The Kidney, Ureter, and Bladder (KUB) X-ray revealed an intravesical necklace drawn by small stones (Figure 1). The rest of biologic assessment was normal. An open prostatectomy was indicated in front of this clinical picture. An enucleation of prostatic adenoma, and removal of the stones were performed.
Figure 1A shows the patient's KUB showing the arrangement of intravesical necklace calculi, Figure 1B shows the extraction of 17 stones forming the necklace, Figure 1C shows the whole piece of prostate adenoma and extracted calculi.
In general, men with Benin Prostate Hyperplasia (BPH) and bladder stones are more likely to have a history of kidney lithiasis, gout, lower urinary pH, lower urinary magnesium levels than men with BPH, but without bladder calculi. The presence of urinary tract infection and a prostatic median lobe (BPH) protrusion are the clinical signs most closely associated with the development of bladder calculi [2].
None declared.
Obtained.
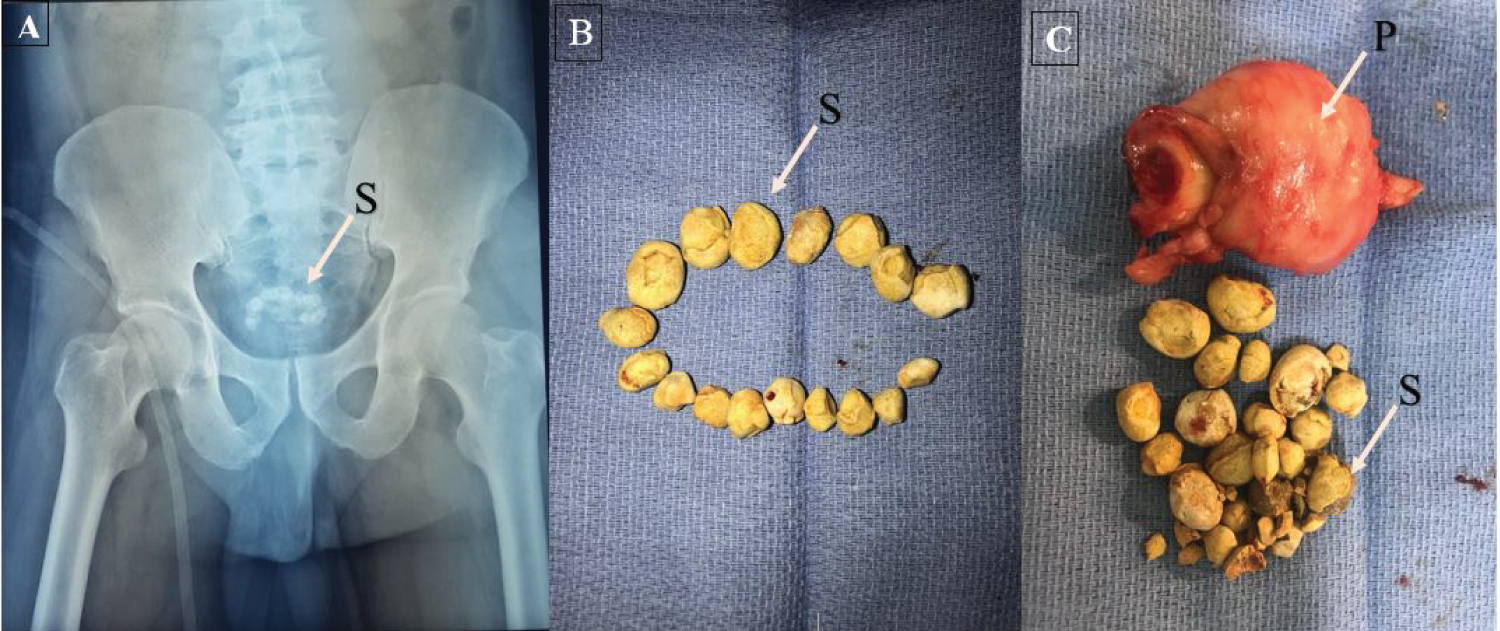
Figure 1: (A) KUB X-rays showing the intravesical calculi (S) arranged like necklace; (B) Total of the 17 stones (S) extracted; (C) Prostate adenoma (P) and extracted stones.