Popliteal Pterygium Syndrome (PPS) is autosomal dominant syndrome with incomplete penetrance and variable expressivity. We report a case of 18-year-old female, who had repair of cleft of lip and palate in childhood, and now presented with paramedian bilateral lower lip pits. Examination revealed her to be a case of sporadic PPS. A comprehensive plan of management was formed, but the patient was lost to follow-up. We report the case for the purpose of educating the clinicians of this rare syndrome and highlighting the importance of proper counselling at index presentation.
Popliteal pterygium syndrome, Cleft lip, Cleft palate, Pterygium, Equinus
Popliteal Pterygium Syndrome (PPS) is autosomal dominant syndrome with incomplete penetrance and variable expressivity [1]. Most cases are sporadic [2]. Its incidence is approximately 1 in 300000 live births. It was first described by Trelat in 1869, named after its most characteristic feature, a web of skin between thigh and leg, present in 96% cases [2].
The spectrum of PPS includes orofacial, musculoskeletal and genitourinary anomalies. The diagnostic criteria for PPS are any three of the following, namely, cleft lip/palate, popliteal pterygium, paramedian lower lip sinuses, genital and toe nail anomalies [3]. There is no growth disturbance and intelligence is usually normal [3]. Rarity of presentation prompted us to report it.
An 18-year-old female, from tribal background, presented with two lower lip pits and a limping gait (Figure 1). She was born out of a non-consanguineous marriage, at full term, without any complications and was youngest of five siblings, the rest of whom were apparently normal. There was no similar affliction in any family member. She had been operated in a surgical camp in childhood for cleft lip and palate, of which no documents were available.
Examination of face revealed maxillary retrusion, scar on left upper lip indicating repaired cleft lip, broad philtrum, bilateral paramedian pits on lower lip vermillion, equidistant (5 mm) from midline, with serous fluid oozing from the pits, obtuse left alar-facial groove, asymmetrical nose with broad tip, left ala more posteriorly and laterally positioned, left nostril wider than right, obtuse angle between medial and lateral crus of left alar cartilage and caudal end of columella deviated to the right (Figure 1, Figure 2 and Figure 3). Intraoral examination revealed scar of repaired cleft palate, high arched palate, cleft of left alveolus and medial collapse of both dental arches. Left upper medial and lateral incisors were absent and left upper canine had erupted into the cleft (Figure 4). She had class III malocclusion and crossbite. Her voice had hypernasality and nasal resonance. She had mild conductive deafness on both sides.
On further examination, she had a pterygium in right lower limb, spanning from ischial tuberosity to heel of foot, causing flexion deformity of right knee and equinus deformity of foot and distortion of arches of foot (Figure 5 and Figure 6). There was heaping of skin on right hallux eponychium (Figure 7). Echocardiography revealed no cardiac anomalies.
Patient's consent for photography and publication of photographs was taken. Under local anaesthesia, correction of upper lip scar and lower lip pits was done. The patient's family did not want correction of the rest of anomalies and the patient was lost to follow-up.
The aim of treatment is to allow the PPS child to run, hear and speak without complications, and to look as normal as possible by age of 4 years [2]. Release of ankyloblepharon, symblepharon, syngnathia and oral synechiae must be done soon after birth [2]. Repair of cleft of lip and palate must be done within first year of life. Early release of popliteal webs is important to allow growth of the limb [2]. Adhesion of popliteal artery and peroneal nerve within the popliteal pterygium may necessitate soft tissue lengthening with Ilizarovdevice, before excision of the pterygium is performed [4].
No funding or support received by any of the authors.
No conflict of interest declared of any author.
The manuscript has been read and approved by all the authors, that the requirements for authorship have been met, and that each author believes that the manuscript represents honest work.

Figure 1: Frontal view of face.

Figure 2: Right lateral view of face.

Figure 3: Worm's eye view of face.
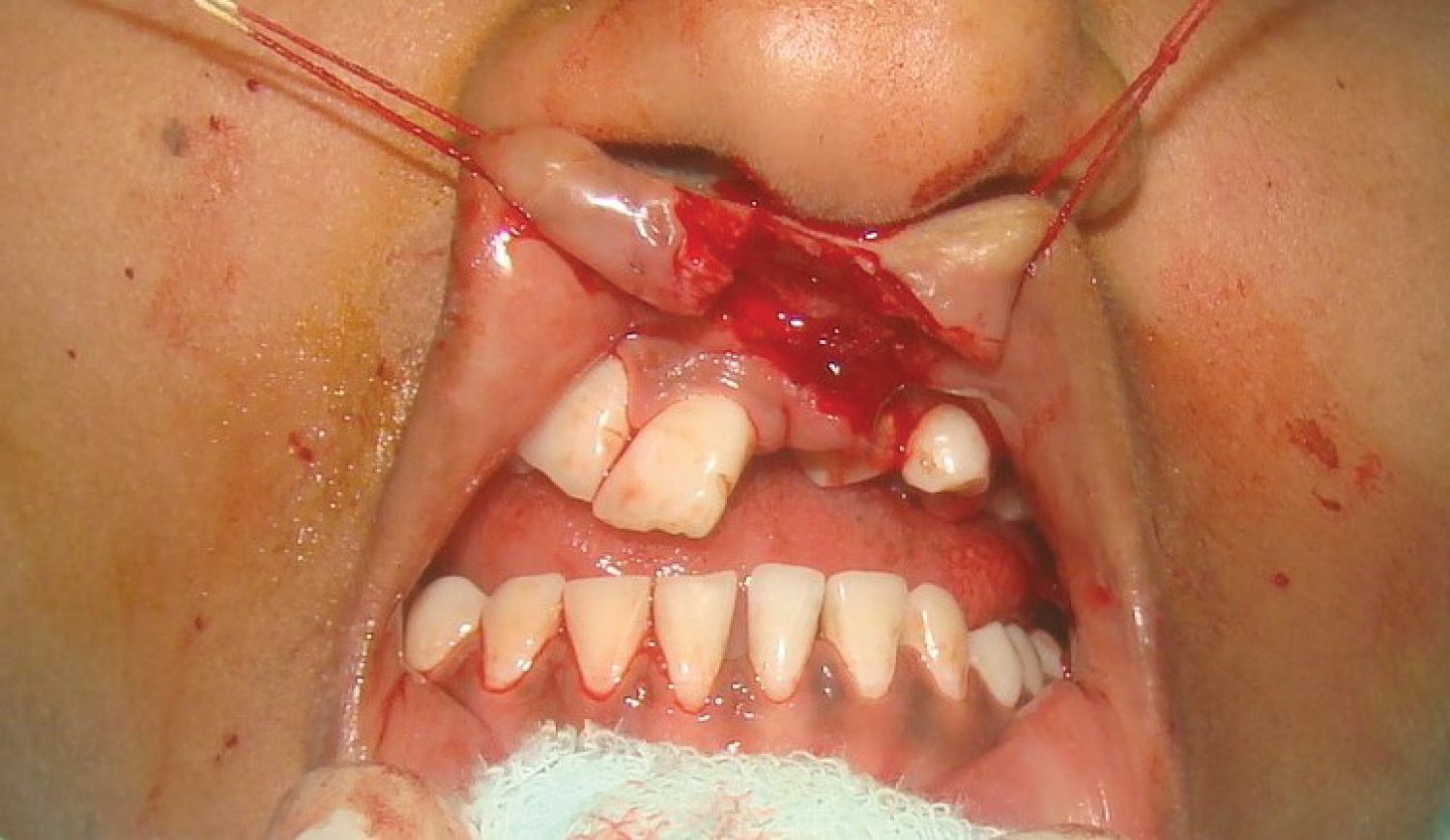
Figure 4: View of anterior dentition.

Figure 5: Medial view of right lower limb.

Figure 6: Posterior oblique view of both lower limbs.

Figure 7: View of dorsum of right foot.