Infective endocarditis, Septic pulmonary emboli, Cavitary lung disease
A 29-year-old female with an extensive history of polysubstance abuse presented to an outside hospital for symptoms of myalgias, malaise, and a dry cough for one week in duration. Additional imaging was obtained, most notable for multiple cavitary lung lesions, a possible bronchopleural fistula, and tricuspid valve vegetation. The patient was transferred to our institution for consideration for cardiothoracic surgical intervention. Upon arrival, the patient was found to be hypoxic with an oxygen saturation of 79% on room air, tachypneic, and tachycardic to 130 beats per minute. She presented with altered mentation and was subsequently intubated for worsening respiratory distress. A left lower sternal border diastolic heart murmur and coarse breath sounds on posterior chest auscultation were appreciated. Blood cultures obtained at the previous hospital were positive for methicillin resistant Staphylococcus aureus and reconfirmed on three subsequent sets of repeat blood cultures. CT scan findings were significant for numerous lung cavitating lesions with thickened walls bilaterally (Figures 1, Figure 2, Figure 3, Figure 4 and Figure 5), as well as bilateral renal and splenic hypodensities concerning for infarctions. Echocardiogram revealed tricuspid valve regurgitation and multiple vegetations (Figure 6). Admission complete blood count was significant for leukocytosis with a white blood cell count of 24.2k /uL, thrombocytopenia with a platelet count of 24 k/uL. All of the above findings in conjunction with history were suggestive of cavitary septic emboli from infective endocarditis. The patient developed septic shock due to endocarditis and a right pneumothorax likely secondary to a ruptured cavity (Figure 4). Cardiothoracic surgery evaluated the patient for consideration for tricuspid valve repair and deemed her to not be a surgical candidate given her pulmonary status. After a discussion with the patient's family, the patient was palliatively extubated and the patient unfortunately expired [1,2].
Special thank you to the medical ICU staff at Abington-Jefferson Health for the care of this patient. The authors declare no conflicts of interest.
None.
Nathaniel Rosal: Conceptualization, Original draft preparation, Investigation. Shafaq Tariq: Original draft preparation, Investigation, Editing. John C Madara: Supervision.
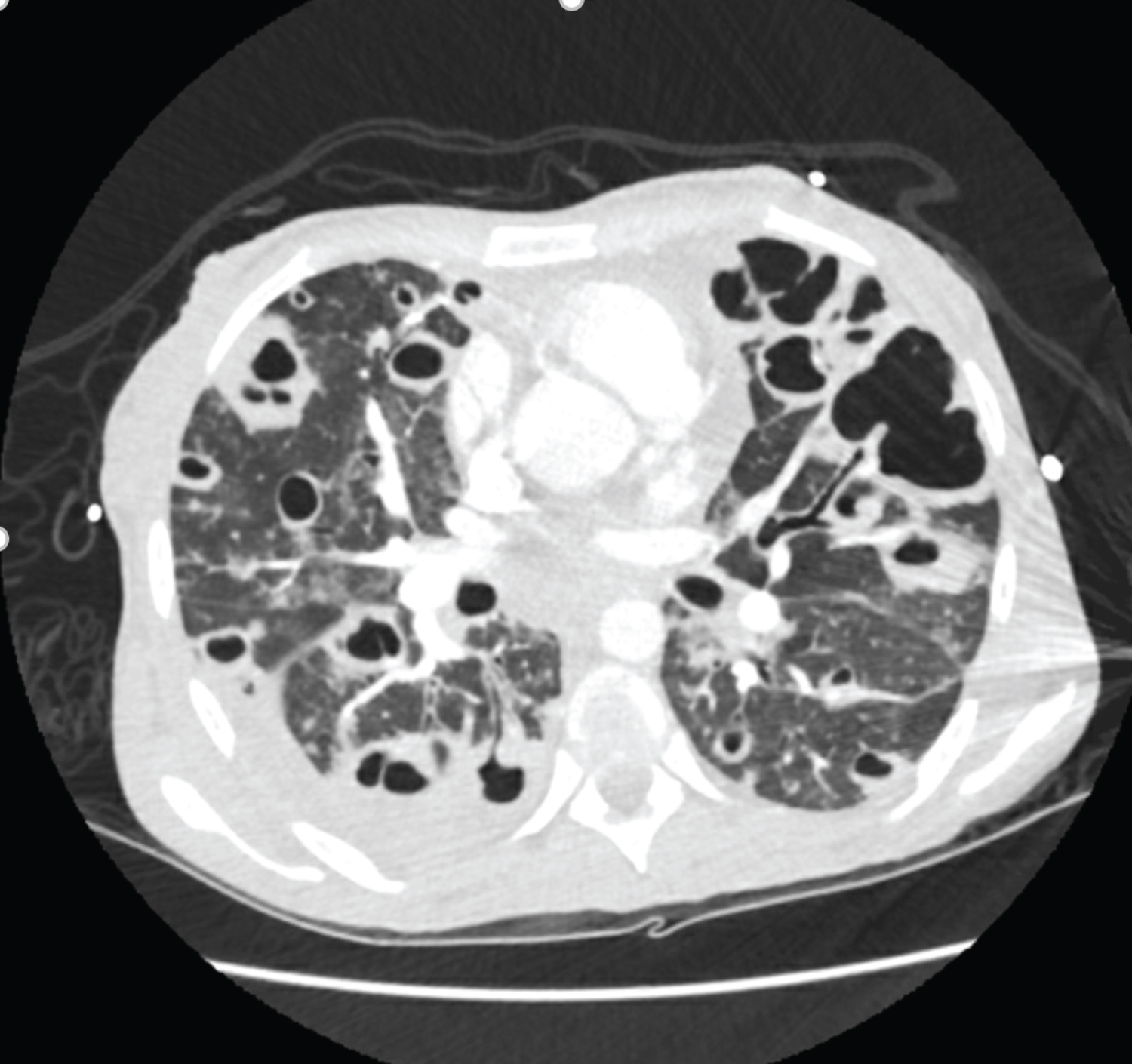
Figure 1: CT scan of the chest at the level of the upper lung lobes.
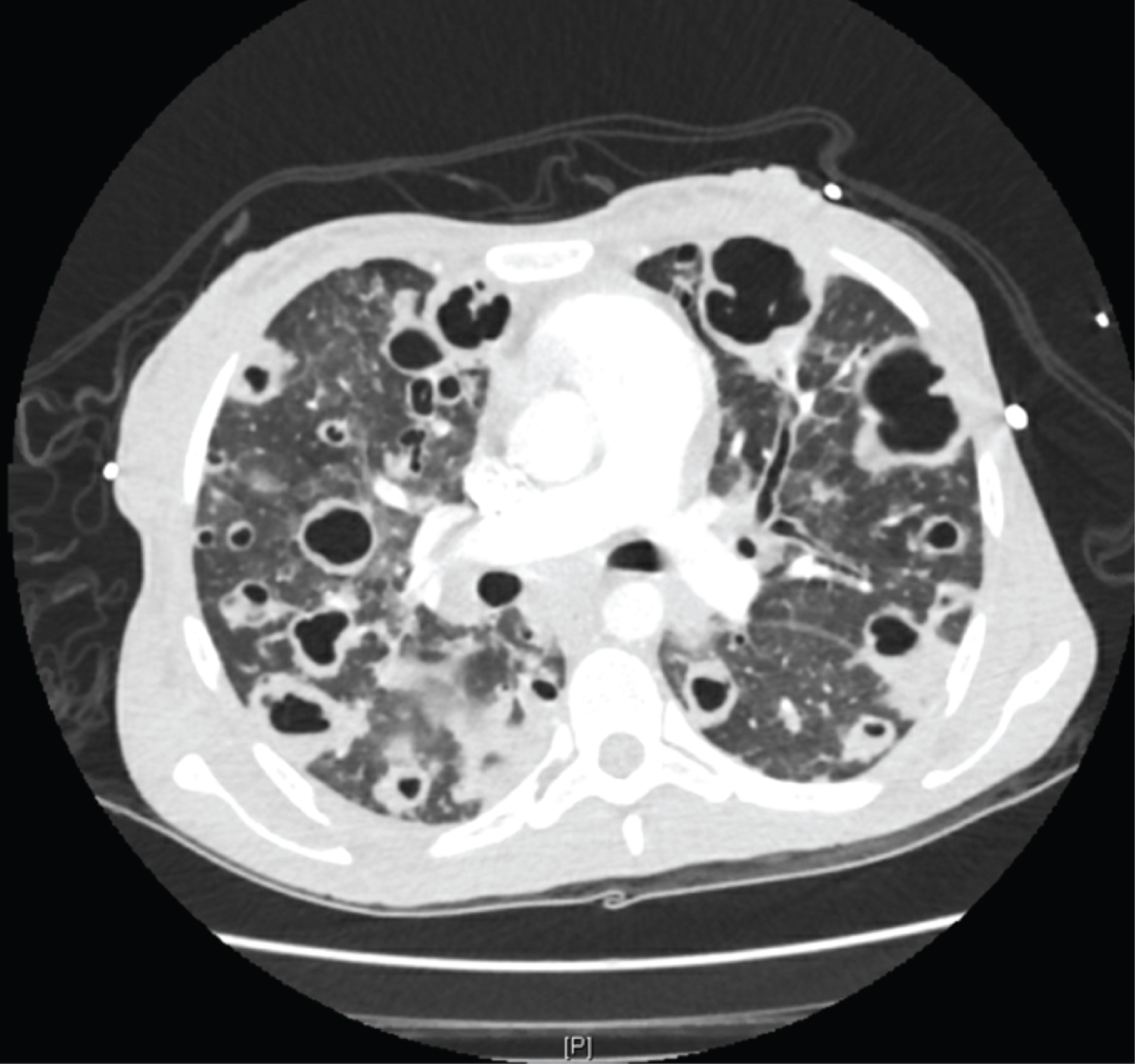
Figure 2: CT scan of the chest at level of pulmonary arteries.
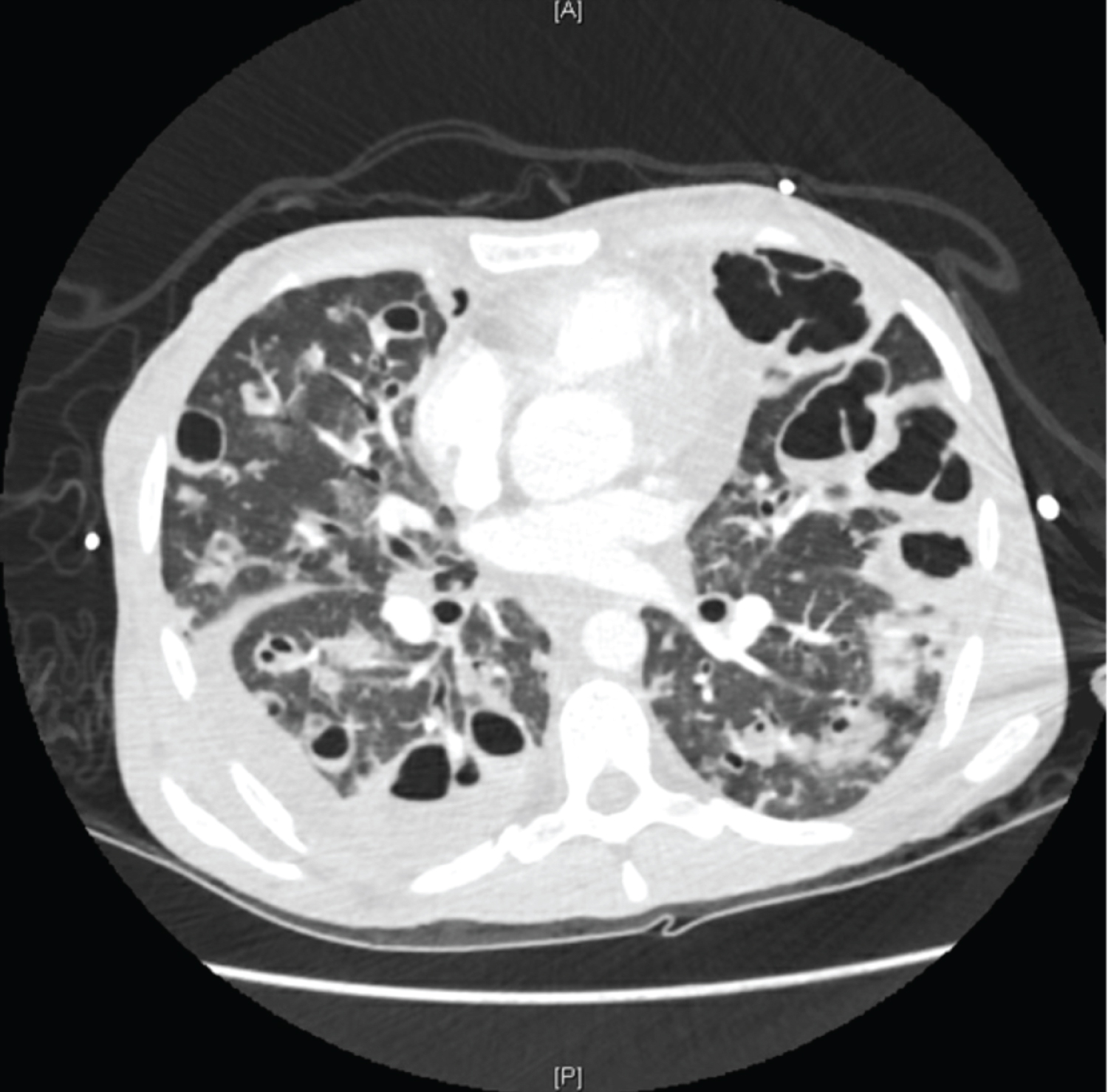
Figure 3: CT scan of the chest inferior to the level of the pulmonary arteries with evidence of right sided pleural effusion.
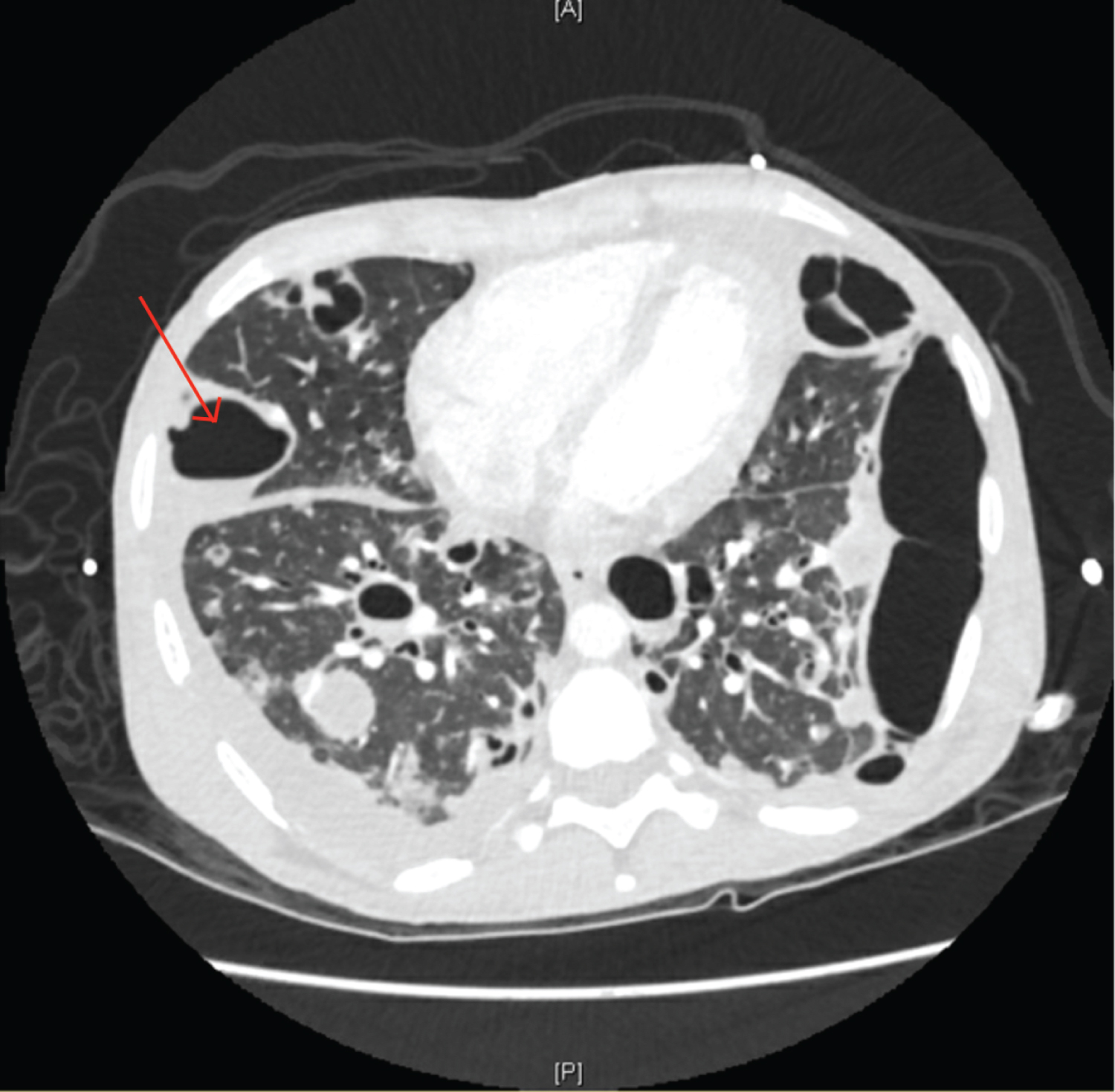
Figure 4: CT scan of the chest with arrow pointing to the cavity that later ruptured. Left sided cavity spanning entire left lung border.
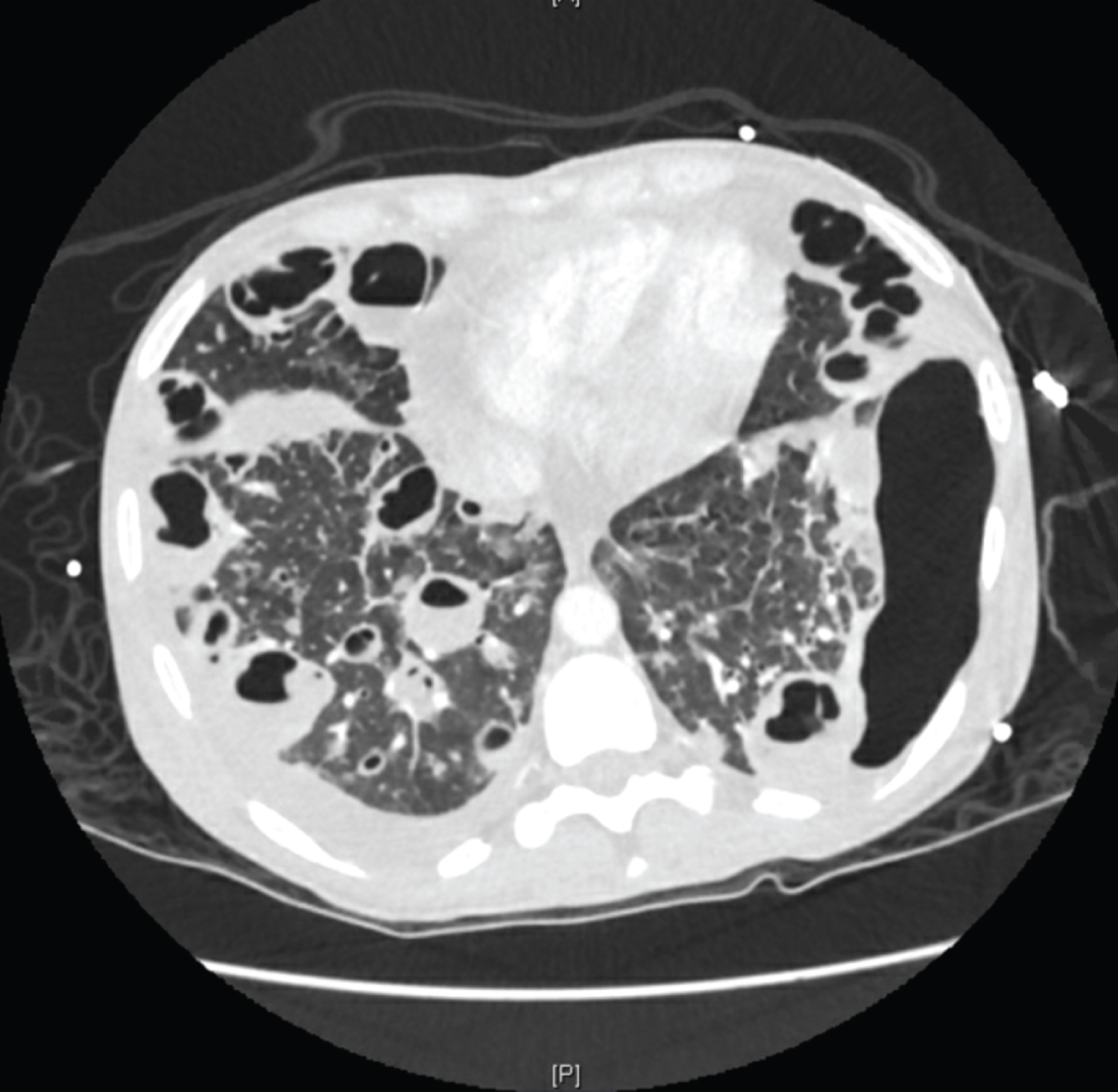
Figure 5: CT scan of the chest at the level of the lung bases.
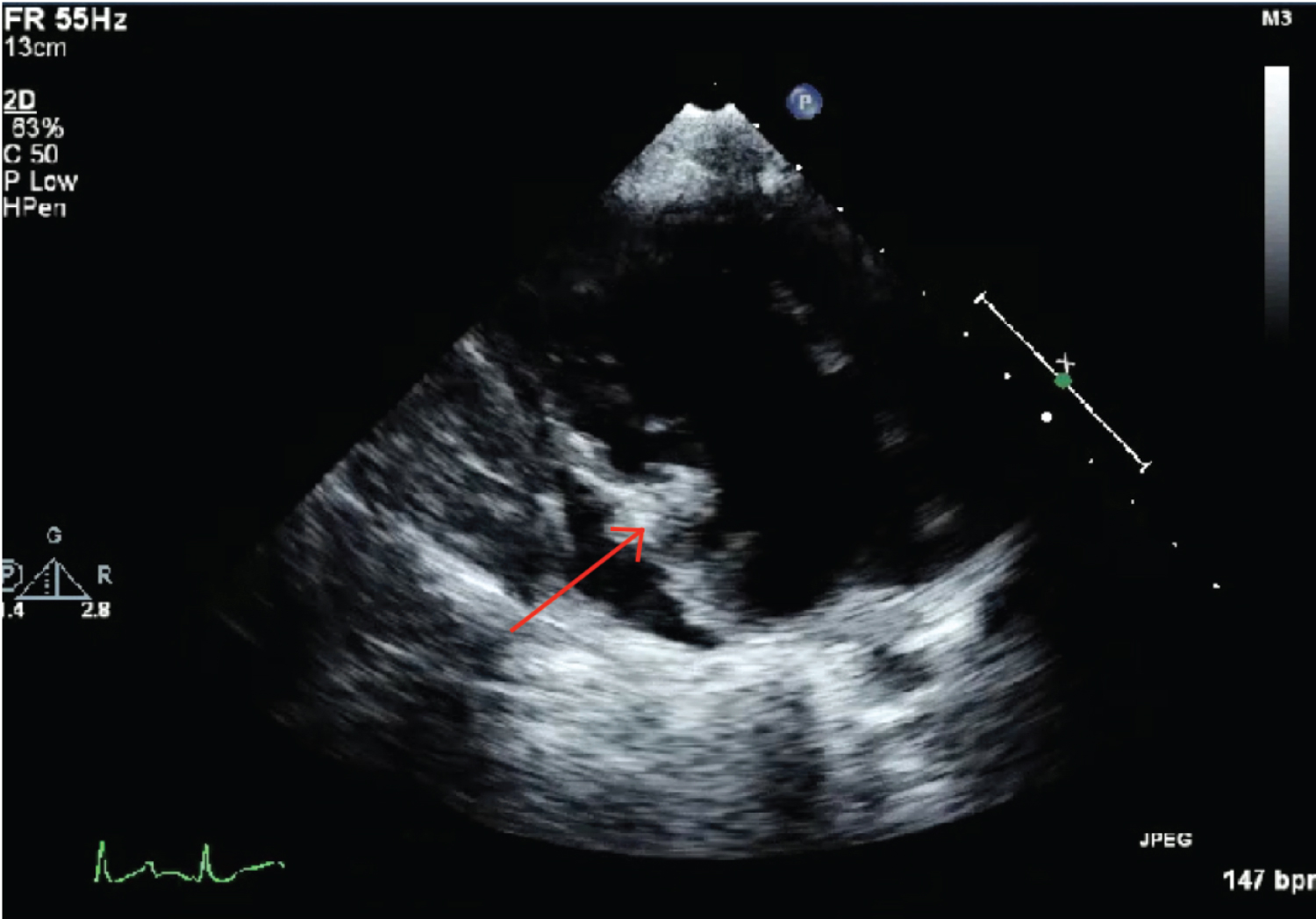
Figure 6: Echocardiogram snapshot showing tricuspid valve vegetation.