81-year-old man presented with one day history of visual disturbance with associated chest discomfort. At the time of initial assessment his visual deficits had resolved. Initial CT brain showed area of hypoattenuation involving right occipital lobe concerning for an infarct. His background history included atrial fibrillation for which he was therapeutically anticoagulated with warfarin and INR was 2.7. Transthoracic echocardiogram showed a severely dilated leftatrium with a large mobile mass attempting to enter the left ventricle measuring 3.8 by 2.6 cm, consistent with a tumour (Panel 1). MRI brain showed bilateral regions compatible with recent infarction involving all vascular territories with a large area of established territorial infarction within the right occipital lobe (Panel 2A & Panel 2B). Findings were suggestive of a large recent embolic burden from atrial myxoma with haemorrhagic transformation.
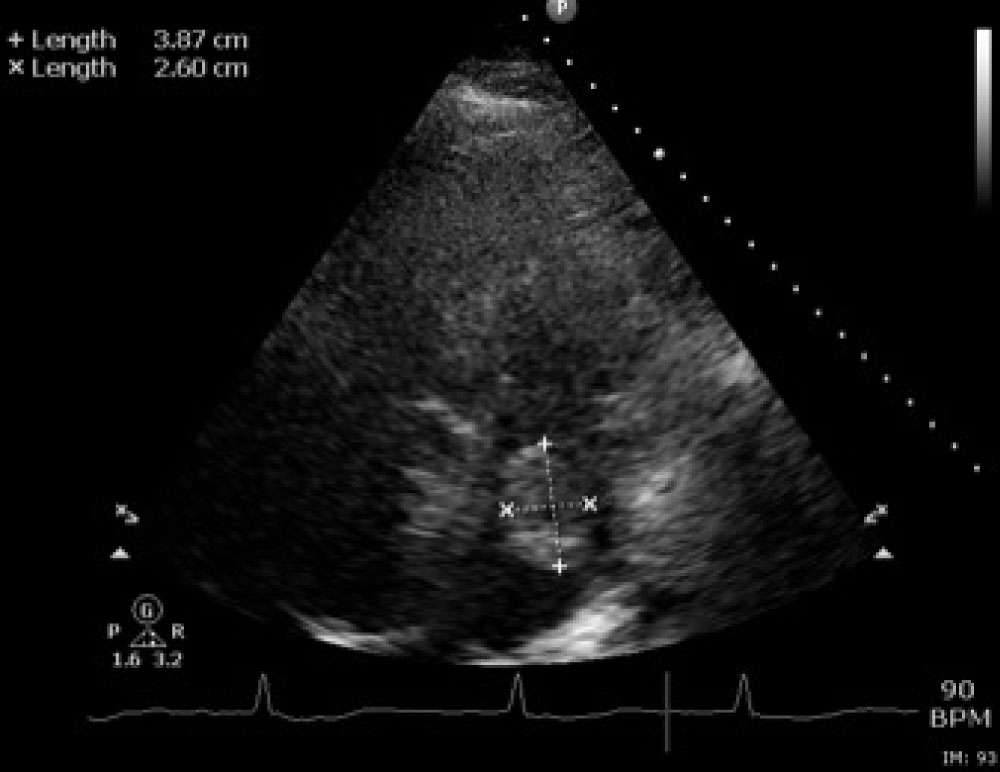
Figure 1: Severely dilated left atrium. Large mobile mass within the left atrium, attempting to enter the LV, measuring 3.8 by 2.6 cm, likely tumour. In some views the mass appears free in the LA.
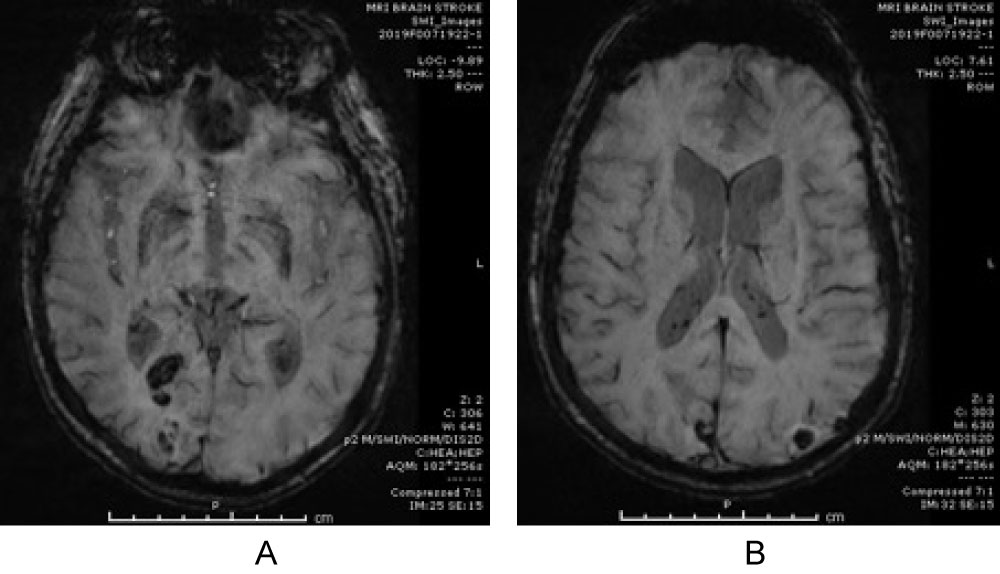
Figure 2: A,B) Bilateral regions of diffusion restriction compatible with recent infarction involving all vascular territories with a large area of established territorial infarction within the right occipital lobe. Findings suggestive of a large recent embolic burden with haemorrhagic transformation.