Increased expression of Bcl-2 protein has been demonstrated in various cancerous and precancerous lesions. The B-cell lymphoma-2 gene is a proto-oncogene that inhibits apoptosis, therefore keeping the cell alive. Bcl-2 Mutations leads to an overexpression of Bcl-2 products leading to apoptosis impairment resulting in neoplastic changes as a consequence. Hence, the objective of the study was to investigate the expression of Bcl-2 in fibro epithelial polyp (FP), oral epithelial dysplasia (OED) and oral squamous cell carcinoma (OSCC).
Twenty-three formalin-fixed paraffin-embedded specimens of previously diagnosed cases of FP (n = 9), OED (n = 5) and OSCC (n = 9) were retrieved from the archives of Oral and Histopathology lab of the Faculty of Dentistry, Kuwait University. Immunohistochemical analysis was performed using monoclonal antibody against anti-human Bcl-2 oncoprotein.
The total positivity for Bcl-2 was seen in 100% (9/9) OSCC cases, 60% (3/5) OED cases and 11.1% (1/9) FP cases The difference in Bcl-2 expression was observed to be significant between FP and OED (P < 0.05) and highly significant between FP and OSCC (P < 0.001). No statistically significant differences between the expression of Bcl-2 in OSCC and OED were observed (P > 0.05).
Bcl-2 expression was found to be least in FP and highest in OSCC. The results suggest alterations in Bcl-2 expression could be a favorable environment for malignant transformation. The strong immunoreactivity of Bcl-2 in OED and OSCC suggests alterations in Bcl-2 functioning, hence may play an important role in the early stages of oral carcinogenesis.
Bcl-2, Immunohistochemistry, Fibro epithelial polyp, Oral epithelial dysplasia, Oral squamous cell carcinoma
Bcl-2 is a proto-oncogene which produces proteins that inhibits apoptosis [1]. Dysregulation of apoptosis is thought to play an important part in cancer and degenerative diseases [2]. Bcl-2 is a main member in the family of apoptotic regulators. It modulates the intrinsic apoptotic pathway by binding and neutralizing the mitochondrial Bax and Bak as well as other pro-apoptotic proteins [3].
When a mutation affects the control mechanism of apoptosis and cell survival, cancer occurs, favoring the immortality of the cells and their overgrowth [1]. This increase in survival rate allows new genetic mutations to occur and increases risk of malignant transformation [4]. An increase in Bcl-2 expression is not only important in carcinogenesis, but it also affects the progression of the disease because it increases the survival rate of neoplastic cells and allows higher resistance to therapy.
Bcl-2 proto-oncogene is associated with developing lymphoma [5]. It was first discovered in B-cell lymphoma with a translocation of t (14; 18) (q32; q21) [2]. Over expression of Bcl-2 has been discovered in several human neoplasms including squamous cell carcinoma of the lung, skin, cervix, and also in squamous cell carcinoma of the head and neck and the oral cavity [6-10].
The initial stages of oral squamous cell carcinoma can go unnoticed and remain usually painless [11]. Therefore, early detection of these lesions in susceptible populations is very essential. Detection of apoptotic abnormalities before the consequences become clinically or histologically detectable, will greatly enhance the potential for early diagnosis. The detection of these aberrations by immunohistochemistry (IHC) or molecular techniques may serve as an additional diagnostic tool [12].
Numerous studies have revealed a correlation between expression of Bcl-2 proteins and the progression of neoplastic disease. Bcl-2 expression serves as a biomarker of a neoplastic transformation that would take place in precancerous conditions like oral epithelial dysplasia as well as in already transformed lesions like oral squamous cell carcinoma [13].
This study investigates the differential immunohistochemical expression of Bcl-2 protein in fibroepithelial polyp (FP), oral epithelial dysplasia (OED) and oral squamous cell carcinoma (OSCC) and its potential for allowing identification of dysplastic lesions with increased risk of malignant transformation as well as early diagnosis of OSCC.
This study was approved by the Ethical committee of the Health Science Center of Kuwait University. This study is a retrospective immunohistochemical analysis of twenty-three formalin-fixed paraffin-embedded specimens of previously diagnosed cases of fibro epithelial polyp (FP) (n = 9), oral epithelial dysplasia (OED) (n = 5), and oral squamous cell carcinoma (OSCC) (n = 9), using monoclonal antibody against anti-human Bcl-2 oncoprotein.
All specimens were retrieved from the archival paraffin blocks of the oral histopathology lab, Faculty of dentistry, Kuwait University.
Sections of 5 µm thickness were taken on pre-coated silanized slides for immuno staining. The slides were dried followed by fixing on stretch table at 60° c for 5 minutes, followed by 37° c incubation for 10 minutes for fixing. Then the slides were de-waxed by passing through two changes of xylene for 5 minutes each. Then the slides were dehydrated in 95% alcohol, then in 90% alcohol, and then in 70% alcohol for 3 minutes each. After that, they were washed in tap water for 1 minute. Slides are then dipped in phosphate buffer saline, PBS, for a minute. Later, slides were treated with preheated antigen retrieval solution in 95-100° c water bath for 20 minutes followed by cooling for 20 minutes. Peroxidase block was then added to the slides for 5 minutes. Then primary antibody was added for one hour at room temperature. Then link label for 10 minutes, and slides were washed in 2 changes of PBS for 2 minutes. DAB chromogen was added for 7-10 minutes then washed in 2 changes of PBS for 2 minutes, each. Then counterstained with Mayer’s hematoxylin for 2 minutes, followed by washing in tap water for 1 minute. Slides were dehydrated in graded changes of alcohol (95% and 90% alcohol) for 2 minutes each. The slides were treated with xylene for 5 minutes. Finally, mounting with DPX was done and then slides were observed under the microscope. Positive controls provided along with the immunohistochemistry kit were used. The specimens were analyzed by one observer.
The analysis was done after the staining. The positive cells in each histological section of the specimens were counted in 20x magnification, then classified according to the positivity and intensity.
The percentage of positive cells were counted/intensity was observed by a single observer and were scored according to the method adopted by Fedchenko and Reifenrath; intense staining (+++), moderate staining (++), weak staining (+), and no staining (-) [14]. Statistical analyses were performed using the statistical package of social science (SPSS) software. The proportions were compared using chi-square test of significance.
Table 1 shows the age and sex distribution of the various study samples. Out of the 23 cases, 14 (60.87%) were males and 9 (39.13%) were females. The mean age distribution in FP was 47.12 ± 14.76 years (Mean ± SD) while in OSCC it was 64.29 ± 10.01 years.
Table 1: Demographic characteristics of the study sample. View Table 1
The total positivity for Bcl-2 was seen in 100% (9/9) OSCC cases, 60% (3/5) OED cases and 11.1% (1/9) FP cases (Table 2). On evaluation of intensity of Bcl-2 expression in 9 cases of FP, while 88.9% (8/9) of the cases showed complete negative expression for Bcl-2, 55.6% (5/9) of the OSCC cases demonstrated moderate Bcl-2 intensity. An equal percentage (40%) of the dysplastic cases showed negative and weak Bcl-2 staining (Figure 1).
Table 2: Immunohistochemical staining intensity demonstrating Bcl-2 expression in the different lesions. View Table 2
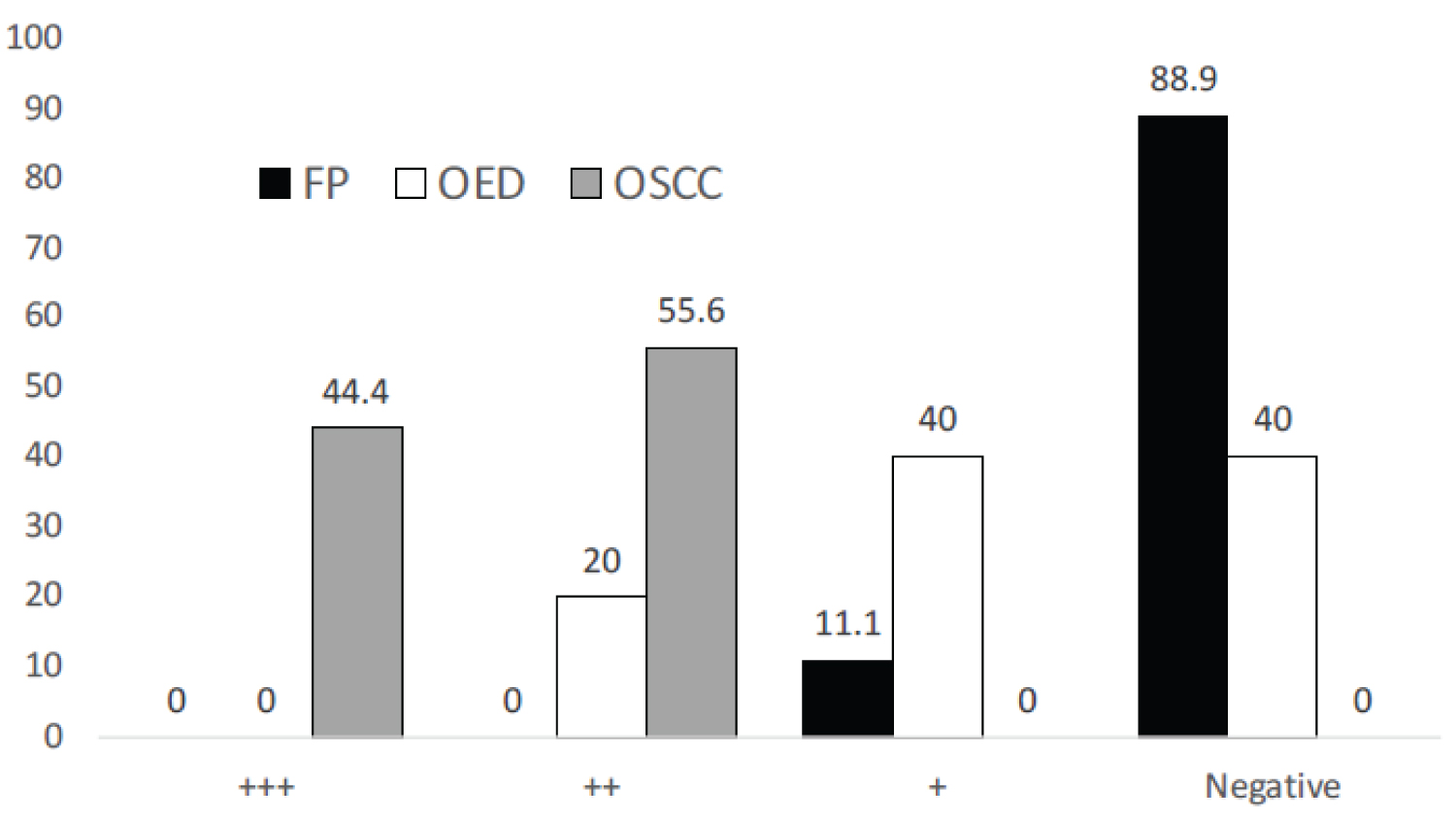 Figure 1: Comparison of intensity of Bcl-2 expression in the different study groups.
View Figure 1
Figure 1: Comparison of intensity of Bcl-2 expression in the different study groups.
View Figure 1
Sections of FP showed weak (+) staining and few positive cells were evident on the basal cell layer (Figure 2A and Figure 2B). In OED, immunostaining for Bcl-2 protein was identified in the basal keratinocytes and parabasal cell layer (Figure 3A and Figure 3B). In sections of OSCC, the distribution of positive cells was seen in peripheral cells that are infiltrating the tumour islands and more extensively in other cases (Figure 4A and Figure 4B).
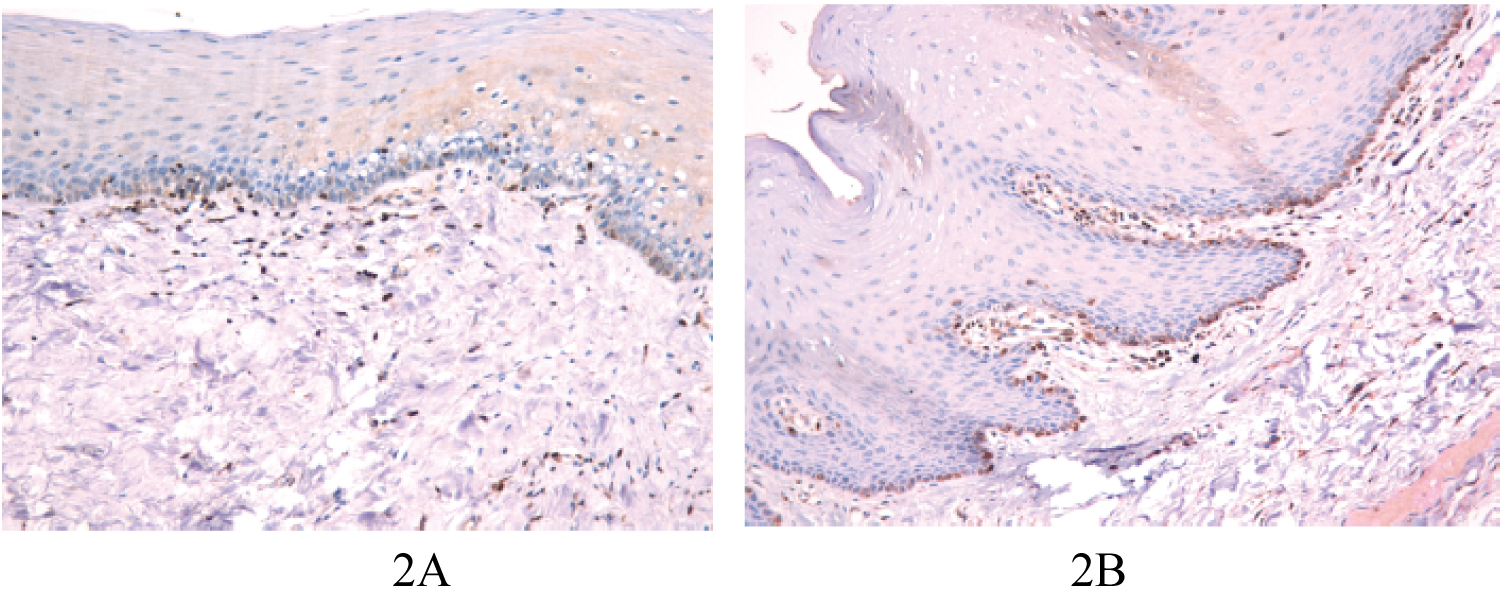 Figure 2: A) Bcl-2 positivity in fibro epithelial polyp (x20); B) Sections of FP showed weak staining, few positive cells were evident on the basal cell layer.
View Figure 2
Figure 2: A) Bcl-2 positivity in fibro epithelial polyp (x20); B) Sections of FP showed weak staining, few positive cells were evident on the basal cell layer.
View Figure 2
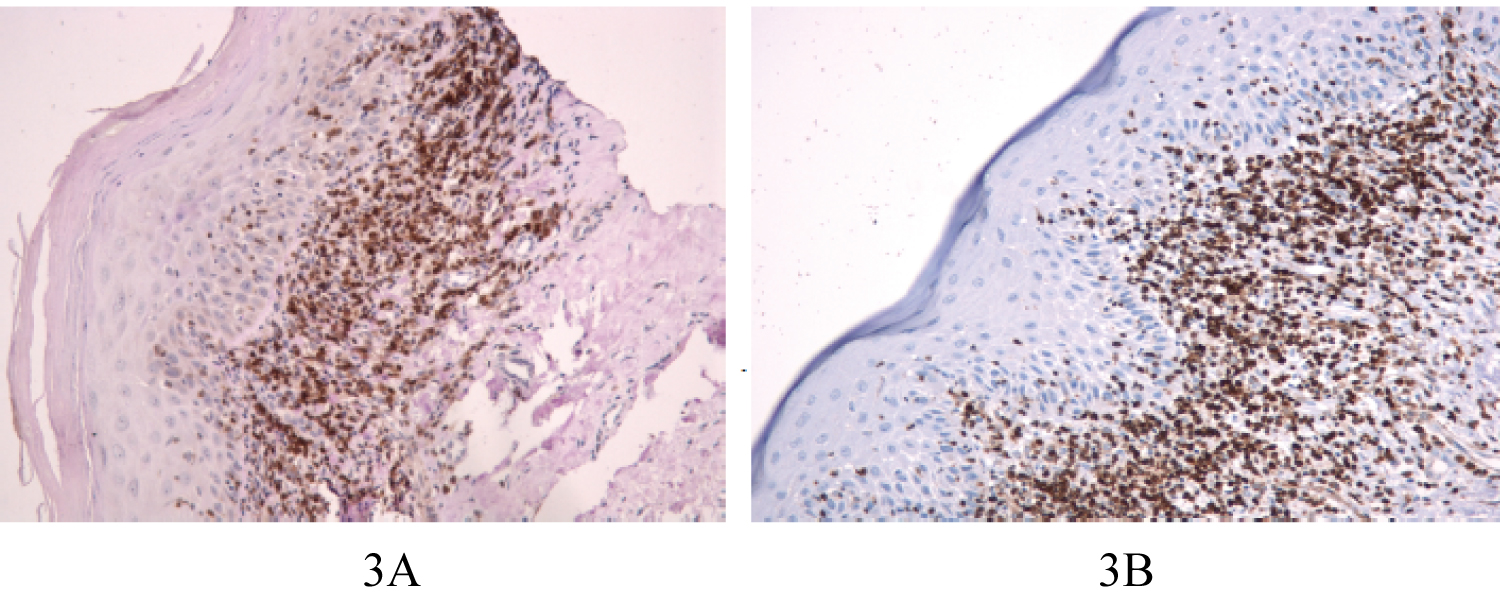 Figure 3: A) Bcl-2 positivity in OED (x20); B) Sections of OED showed Bcl-2 positive cells in basal and parabasal layer of cells.
View Figure 3
Figure 3: A) Bcl-2 positivity in OED (x20); B) Sections of OED showed Bcl-2 positive cells in basal and parabasal layer of cells.
View Figure 3
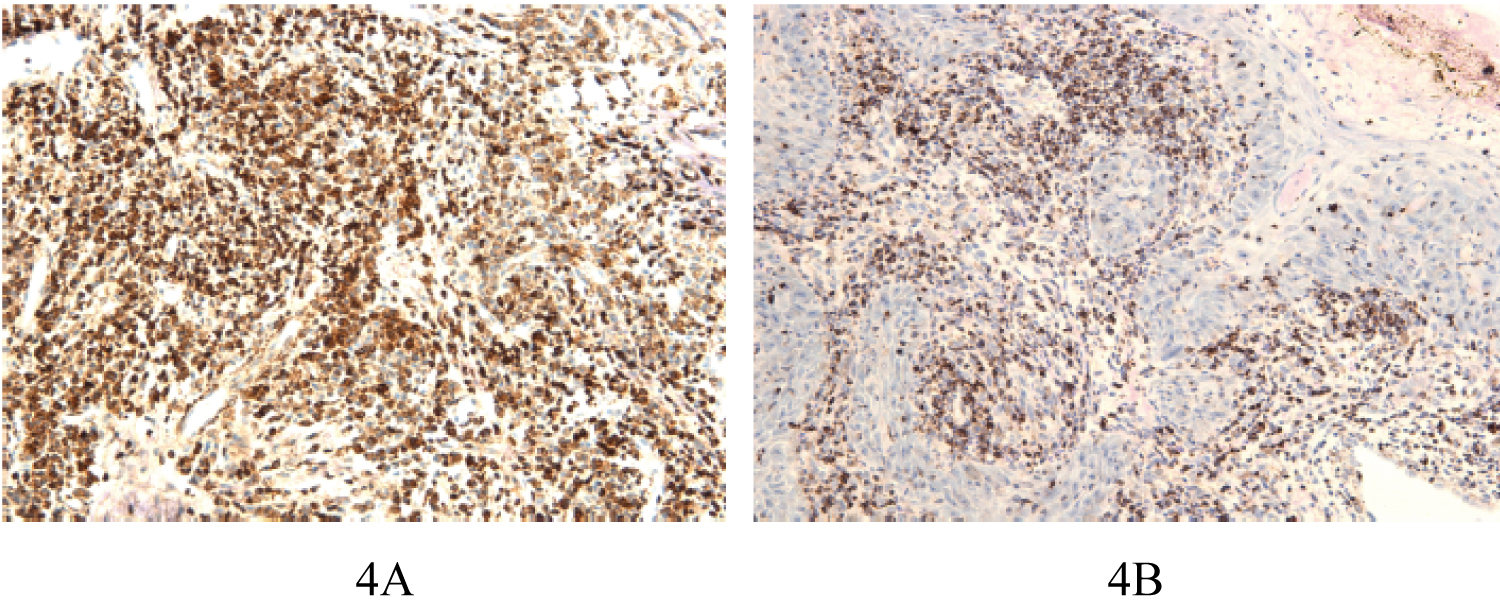 Figure 4: A) Bcl-2 positivity in OSCC (x20); In sections of OSCC, Bcl-2 positivity was seen in peripheral cells that are infiltrating the tumor islands; B) Sections of OSCC showing more extensive Bcl-2 staining.
View Figure 4
Figure 4: A) Bcl-2 positivity in OSCC (x20); In sections of OSCC, Bcl-2 positivity was seen in peripheral cells that are infiltrating the tumor islands; B) Sections of OSCC showing more extensive Bcl-2 staining.
View Figure 4
Positive immunostaining of OED was significantly higher than that of FP (P < 0.05). The expression of Bcl-2 in OSCC was significantly higher than FP (P < 0.001). However, there was no statistically significant difference in Bcl-2 immunostaining between OSCC and OED (P < 0.005).
Bcl-2 was first described in follicular lymphoma that has the translocation (14: 18). This structural abnormality caused the overproduction of Bcl-2 messenger RNA and protein [2]. The protein product of Bcl-2 inhibits apoptosis by preserving the mitochondrial membrane integrity [15]. The increased expression of the anti-apoptotic Bcl-2 favors the accumulation of new mutations because it makes the removal of the genetically modified cell difficult, which can result in the appearance of cells with a malignant phenotype [16].
OSCC has a worldwide prevalence with diverse trends in different regions owing to multifactorial aetiologies [17]. Polverini and Nor suggested that the upregulation of Bcl-2 in human premalignant and malignant keratinocytes may be an early key event in epithelial carcinogenesis [18]. In oral cancer, Bcl-2 is observed from the initial stages of carcinogenesis up to the appearance of metastasis [10,13,19].
Although there is no dearth of literature regarding the Bcl-2 expression in OED and OSCC, limited studies are available regarding Bcl-2 expression in hyperproliferative reactive oral lesions. The sheer global burden of oral cancer and precancer necessitates more studies on the topic. Therefore, the purpose of the current study is to assess and compare the intensity of Bcl-2 immunohistochemical staining in fibroepithelial polyp, oral epithelial dysplasia, and oral squamous cell carcinoma.
Previous studies have reported Bcl-2 expression in the basal layer of the normal oral mucosa (5%-24%) and suggested that Bcl-2 in the proliferative layer of epithelium may protect it from apoptosis. This ensures that the supply of cells for differentiation is not halted and is continuously available [19-21]. Studies have been reported where the Bcl-2 expression was higher in reactive lesions when compared to normal oral mucosa and was mostly confined to the basal layers of epithelium [21,22]. This suggested that anti-apoptotic activity was higher than proliferative activity in reactive lesions as compared to normal oral mucosa.
In our study, only 1 out of the 9 (11.1%) FP cases showed weak positivity (+) and mostly confined to the basal layers of epithelium while the remaining (88.9%) stained negative. Jiang, et al. reported the complete absence of Bcl-2 expression in hyperplastic oral mucosa. The result of current study further supports the hypothesis that the hyperproliferative state, in lesions like FP, may be due to the presence of alternate molecular mechanisms. A study on fibrous epulis revealed that the altered expression of Inhibitor of apoptosis protein (IAP) family in addition to Bcl-2 family leads to increased proliferation and apoptosis inhibition [23].
Similar findings were observed in non-tumorigenic hyperproliferative, keratinocytic lesions and in hyperplastic polyps of colon [24,25]. This leads to the speculation that increased cell proliferation is the key explanation for hyperproliferative state in reactive lesions while in only some lesions, decreased apoptosis plays a role. Nakagawa, et al. clearly indicated that Bcl-2 protein may play a role in proliferation of malignant tumours of keratinocyte origin but may not be responsible for proliferation induced by inflammatory stimuli [7].
Statistically significant difference was observed in the expression of Bcl-2 when FP was compared to OED and OSCC. These results were comparable with those of Nitya, et al., Ravi et al., and Núñez, et al. [21,22,26]. Nitya, et al. attributed the altered expression to the chronic irritation and inflammation in OED and OSCC cases resulting in changes at the cellular level [21]. It would be worthwhile to stress that the increased expression of Bcl-2 (antiapoptotic protein), in reactive lesions with atypical epithelium, like that of OED should be regarded suspicious. Reactive lesions that exhibit dysplasia need to be observed and followed up in a similar fashion as dysplastic lesions [21].
In this study, an overall positivity of 60% (3/5) was observed in OED cases of which 40% were weakly positive (+) and the remaining were moderately positive (++). These findings were like those of Pigatti, et al. (57.1%) and Pallavi, et al. (60%) [27,28]. Other studies showed Bcl-2 positivity ranging from 12% to 37% in OED cases [1,4,19,21,26,29]. Perhaps, the differences in the total positivity of OED in different studies correlates to difference in grades of dysplasia included in the various study populations. Subtle inherent genetic differences among population, gender and age of the population and anatomical location of the studied lesions have been attributed as plausible reasons for the varying results [29].
However, several studies reported a significantly higher Bcl-2 expression compared to normal mucosa and including the parabasal and suprabasal epithelial layers like our study [27,28]. The upregulation of Bcl-2 as observed in dysplastic lesions prolongs genetically altered cell survival, thereby increasing the possibility of appearance and accumulations of mutations which provide a selective growth advantage to the neoplastic clone of cells comprising an oncogene or a tumor suppressor gene [16]. Bcl-2 expression was found to be increasing with increasing grades of dysplasia, thereby suggesting a possible role in malignant transformation [1,19,21].
In this study, the total positivity in OSCC was 100%. While the role of Bcl-2 immunoexpression has been widely investigated, different studies have showed significant difference in percentages. Our results were similar to those of Suri (100%) [20]. Some studies showed high percentage of OSCC cases exhibiting Bcl-2 positivity ranging from 83% to 97% [12,26]. However, few studies showed lower percentages. Juneja, et al. showed a total positivity of 30%, 60% by Jordan, et al. a range of 16.67% to 25% by Singh, et al. and 27% by Sulkowska, et al. [1,10,13,19]. Even though the percentages were lower, most of the studies reported significant upregulation of Bcl-2 immunoexpression. On the other hand, contrary to our findings, a few studies showed a decline in Bcl-2 expression [19,28]. They postulated that Bcl-2 dysregulation is a key event in early tumorigenesis and subsequently diminishes once the tumour gets established.
In this study, there was no statistically significant difference between the expression of Bcl-2 in OSCC and OED. However, and as evident, the increased expression of Bcl-2 in OSCC compared to OED might be an indication of the disease progression from OED to OSCC. Similar results were found in a study conducted by Juneja, et al. [1].
Previous studies have revealed differing levels of Bcl-2 expression with differing tumour grades [1,13]. The limitation of this study is the sample size due to the low prevalence of oral squamous cell carcinoma in Kuwait [30]. Also, owing to the low number of samples, Bcl-2 expression with relation to different grades of dysplasia and carcinoma was not explored. Further studies with more cases pertaining to those parameters are required to reach conclusive significance of Bcl-2 expression in grading, staging and outcome in Oral squamous cell carcinoma.
Bcl-2 is an important molecular marker that has been identified in several carcinomas. There is a significant upregulation in Bcl-2 expression in oral epithelial dysplasia and oral squamous cell carcinoma. More focus on studies exploring the interaction of Bcl-2 with other oncogenes implicated in oral tumorigenesis would offer multiple prospects to alleviate the disease.
We wish to show our gratitude and appreciation for the assistance provided by Mrs. Lovely James from the Department of Diagnostic sciences, Faculty of Dentistry, Kuwait University, Jabriya, Kuwait.
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
The authors hereby declare no conflict of interest.