Duodenal perforation due to endoscopic sphincterotomy is an uncommon but occasionally fatal complication. This serious complication has been traditionally treated by immediate surgical exploration when digestive fluid leakage occurs.
Herein, we will present the percutaneous treatments of an endoscopic sphincterotomy-related duodenal perforation and perforation-related retroperitoneal abscess by using percutaneous drainage techniques. An 8-F internal-external biliary drainage catheter provided mechanical obstruction of the periampullary perforation site and also prevented continuous bile or pancreatic fluid leakage through the perforation. Additionally, a perforation-related retroperitoneal abscess was also successfully treated by utilizing percutaneous drainage catheters.
This is, to the best of our knowledge, the first report of percutaneous treatment of endoscopy-related duodenal perforation requiring emergency surgical treatment.
Duodenal perforation, ERCP, Percutaneous treatment
ERCP: Endoscopic Retrograde Cholangiopancreatography; PTC: Percutaneous Transhepatic Cholangiography; CRP: C-Reactive Protein; ESR: Erythrocyte Sedimentation Rate
Endoscopic retrograde cholangiopancreatography (ERCP) with sphincterotomy is commonly performed to treat hepato-pancreato-biliary disease. Duodenal perforation due to endoscopic sphincterotomy is an uncommon but occasionally fatal complication. Although the perforation occurs in about 1% of these patients, it is associated with a relatively high mortality rate of 7% to 25% [1,2].
Traditionally, duodenal perforation has been treated with early surgical repair. Recently, nonoperative early endoscopic management techniques including clips or fibrin glue have been reported. The treatment of perforations depends on the characteristics of the perforation, the type of perforation should be determined as soon as possible. Peri-vaterian or type 2 injuries are injuries at the sphincter of Oddi and can be managed conservatively to a large extent [3,4]. If conservative treatment is performed, biliary drainage is necessary to prevent further bile leakage from the perforation site. If endoscopic biliary drainage is difficult to perform, percutaneous transhepatic biliary drainage should be considered. Surgical treatment should be considered if consistent biliary obstruction or cholangitis occurs or the patient's condition worsens after conservative treatment.
This case may be the first report, but by no means the first use of percutaneous treatment of endoscopy-related duodenal perforation.
A 42-year-old female patient was admitted to our hospital with a history of intermittent abdominal pain and abnormal liver function tests. She underwent ERCP for suspected dysfunction of the sphincter of Oddi. Following several failed cannulation attempts of the ampulla and common bile duct, a precut sphincterotomy was indicated. Despite attempts to perform a precut sphincterotomy, cannulation of the ampulla was again unsuccessful and the procedure was terminated. The following day, the patient's condition deteriorated as she became pyrexial and unstable. Her right upper and lower quadrants were tender by palpation. Vital signs were as follows: Blood pressure 110/80 mmHg, heart rate 108/min, respiratory rate 27/min and temperature 38.7 ℃. The laboratory studies as follows: WBC 17,610/mm3, amylase 1461 U/L, lipase > 300 U/L, C-reactive protein (CRP) 15.1 mg/dL and Erythrocyte Sedimentation Rate (ESR) 42 mm/hr. SGOT, SGPT, alkaline phosphatase, total bilirubin, albumin, total protein, BUN/Cr and serum electrolyte levels were normal. Abdominal computed tomography showed a large amount of air and fluid collections in the paraduodenal, perirenal and right retrocolic spaces (Figure 1a). After diagnosis of duodenal perforation, intravenous fluids were administered, a nasogastric tube was inserted, and intravenous antibiotics were administered. The patient was than referred to our interventional radiology unit. Percutaneous transhepatic cholangiography (PTC) and drainage catheter deployment were scheduled.
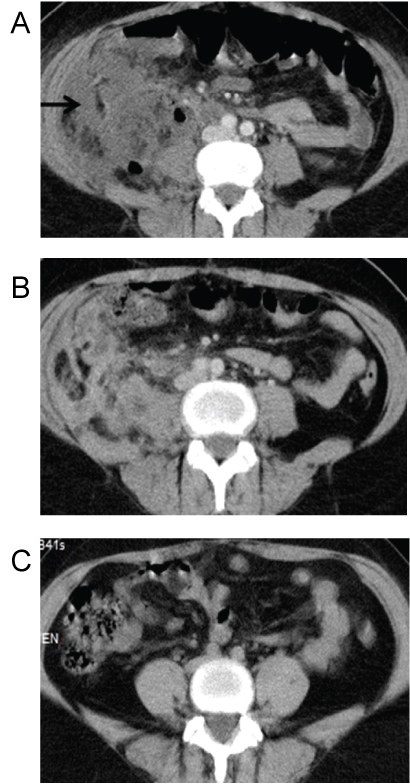 Figure 1: a) Contrast enhanced abdominal computed tomography showed a large amount of air and fluid collections in the retroperitoneal spaces (black arrow); b) Resolution of abscess after 25 days; c) Recent CT after one year follow up.
View Figure 1
Figure 1: a) Contrast enhanced abdominal computed tomography showed a large amount of air and fluid collections in the retroperitoneal spaces (black arrow); b) Resolution of abscess after 25 days; c) Recent CT after one year follow up.
View Figure 1
PTC was performed using the standard technique from the right mid-axillary approach using a 21G Chiba needle. As intrahepatic bile ducts were not visible during abdomen ultrasonography, fluoroscopy guidance was used to enter the bile ducts. After contrast medium injection, cholangiography showed mild dilatation and distal stenosis of the common bile duct and contrast leakage into the retroperitoneal cavity from medial wall of the duodenum, which was diagnosed as Type II duodenal perforation (Figure 2a). The stenosis of distal common bile duct was crossed by using 5-Fr vertebral catheter and 0.035-inc hydrophilic guide wire. Over the wire, an 8-Fr biliary drainage catheter was deployed across to ampulla and perforation site (Figure 2b). The tip of the catheter was placed into second part of the duodenum.
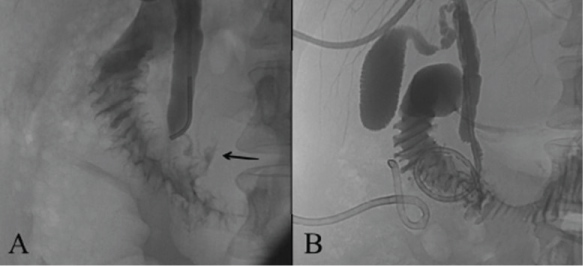 Figure 2: a) Percutaneous transhepatic cholangiography showed mild dilation and distal stenosis of the common bile duct and contrast lekage into the retroperitoneal cavity from medial wall of the duodenum (black arrow); b) An 8-Fr biliary drainage catheter was deployed across to ampulla and perforation site.
View Figure 2
Figure 2: a) Percutaneous transhepatic cholangiography showed mild dilation and distal stenosis of the common bile duct and contrast lekage into the retroperitoneal cavity from medial wall of the duodenum (black arrow); b) An 8-Fr biliary drainage catheter was deployed across to ampulla and perforation site.
View Figure 2
On the sixth day after the endoscopy, the patient developed a non-remitting fever. Blood investigations showed leukocytosis, altered CRP and ESR. Control abdomen computed tomography (CT) showed the development of large abscess formation within the retroperitoneal space. Two 10 Fr drainage catheters was deployed under CT-guided for treatment of perirenal and retrocolic abscesses. E. coli was isolated from the abscess samples. On the 10th day, nasogastric tube was removed and on the 15th day after the endoscopy, follow-up catheter cholangiography showed no leakage of contrast medium from the duodenum. Over the next three weeks, the amount of the abscess drainage decreased and abscess drainage catheters were removed on the 25th day after the perforation (Figure 1b). On the 35th day, the internal-external biliary drainage catheter was removed, and two internal plastic stents crossing the ampulla were deployed percutaneously. No complication related to these procedures was observed. Full recovery was observed after one year follow-up (Figure 1c).
Duodenal perforation during endoscopy is a rare and serious complication with high risk of mortality and morbidity. Stapfer, et al. clinically classified perforations into four distinct categories according to severity [5]. The treatment option depends on the characteristics of the perforation and clinical status of the patient [6,7]. Our patient was diagnosed as Type II periampullary perforation with a large accumulation of digestive fluid into the retroperitoneal spaces. A percutaneous biliary drainage catheter provided mechanical obstruction at the periampullary perforation site and also prevented continuous bile or pancreatic fluid leakage through the perforation. After the biliary drainage catheter deployment, the perforation site was closed and repaired completely, but subsequent retroperitoneal abscesses emerged due to previous fluid leakage. Those perforations were also successfully treated by utilizing additional percutaneous drainage catheters within four weeks.
This is an promising technique but it can't be performed in case of hemodynamic instability. PTC can usually be performed in cases where intrahepatic biliary tracts are dilated. In cases where intrahepatic biliary tract is minimally dilated, PTC can be performed by experienced specialist but success rate may be lower.
In conclusion, this report showed that the placement of a percutaneous biliary drainage catheter provided mechanical obstruction at the perforation site and prevented continuous bile or pancreatic fluid leakage through the perforation. These beneficial effects resulted in rapid recovery of the perforation within one week. Additional perforation-related complications such as retroperitoneal abscesses were also successfully treated by percutaneous drainage catheters.
This is an promising technique but it can't be performed in case of hemodynamic instability. PTC can usually be performed in cases where intrahepatic biliary tracts are dilated. In cases where intrahepatic biliary tract is minimally dilated, PTC can be performed by experienced specialist but success rate may be lower.
Written approval was obtained from Cukurova University Faculty of Medicine Clinical Ethical Board.
Written informed consent was obtained from all patients and parents.
Consent for publication: not applicable.
The datasets used and/or analysed during the current study are available from the corresponding author on request.
The authors declare that they have no competing interests.
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
All authors have made substantial contributions to the conception and design of the study, acquisition of data, or analysis and interpretation; drafting the article or revising it critically for important intellectual content and final approval of the version to be submitted.
All named authors meet the International Committee of Medical Journal Editors (ICMJE) criteria for authorship for this article, take responsibility for the integrity of the work as a whole, and have given their approval for this version to be published. All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.