Obesity is rapidly escalating in Malaysia in all age groups. Prevalence of obesity and overweight is increasing in adults and in children in both developed and developing countries. Obesity is a risk factor for many conditions including respiratory disorders regardless of BMI. However, studies investigating pulmonary functions in obese adolescents in Malaysia are few. Hence, the present study was aimed to investigate pulmonary function variables in the adolescent obese students of management and science university (MSU) in Malaysia.
1. To evaluate the effect of obesity on pulmonary function among adolescent students of MSU.
2. To identify the association between waist circumference (WC), body mass index(BMI) and waist hip ratio with pulmonary function among adolescent students of MSU.
Dynamic lung functions were measured in 50 obese adolescent students of both sexes and an equal number of age-matched controls using Spirobank II MIR via Del Maggiolino125, 00155 Roma, Italy. Waist and hip circumference were measured using measuring tape.
There was no significant difference in mean pulmonary function parameters between obese and non-obese control group. However, some of the obese subjects had mild restriction, whereas no obstructive impairment was detected in any subject of the obese and control groups.
BMI, waist circumference and hip circumference has strong negative correlation with FEV1/FVC (P < 0.01), waist hip ratio was negatively correlated to FEV1/FVC but correlation was not significant. Waist circumference has strong positive significant correlation with FVC (P < 0.001), whereas waist hip ratio has no significant correlation with any pulmonary function parameters.
In conclusion, our study did not show a significant effect of obesity/overweight on dynamic lung volumes among adolescent of MSU. Significant negative correlation between BMI, waist circumference and hip circumference with FEV1/FVC suggest that obesity decreases FEV1/FVC ratio and obese are more prone to obstructive lung diseases.
Obesity, Pulmonary function test, Body mass index (BMI), Waist circumference, Hip circumference, Waist Hip ratio
The lifestyle of students has changed in the past decades. Nowadays many of them have adopted unhealthy habits, like lack of exercise, intake of fast food that may impair their health [1]. Prevalence of obesity and overweight is increasing in adults and in children in both developed and developing countries [2,3]. Obesity is a risk factor for many conditions including respiratory disorders such as asthma, increased airway resistance and atopy [4,5]. Therefore, increasing numbers of obese children with respiratory disorders are referred for lung function testing.
The effects of obesity on pulmonary function parameters are influenced by the amount and distribution of body fat [6-8]. Studies have shown that central obesity, which may be measured by waist circumference or by waist-to-hip ratio, can influence respiratory mechanics regardless of BMI [6,8]. Both BMI and WC are usual measures of overweight and obesity, but also indicators of body size, and they therefore may be associated with pulmonary function parameters such as forced expiratory volume in 1st second (FEV1) and forced vital capacity (FVC) [9,10]. However, studies investigating pulmonary functions in obese adolescent in Malaysia are few. Hence, the present study was aimed to investigate pulmonary function variables in the adolescent obese students of management and science university (MSU) in Malaysia.
1. To evaluate the effect of obesity on pulmonary function among adolescent of MSU.
2. To identify the association between waist circumference (WC) , body mass index (BMI) and waist hip ratio with pulmonary function among adolescent students of MSU.
A cross-sectional comparative study has been conducted among the adolescent students of MSU.
Necessary ethical approval has been taken from the university ethical committee
MSU students of both sexes aged between 16 to 22 years were randomly selected for the study. Written consent was obtained from each participant.
Body mass index (BMI) of each subject was calculated as per the following formula:
Body mass index = weight (kilograms)/height2 (meter2). Subjects having BMI greater than the 95th percentile for age were classified as obese [11]. A total of 50 such obese boys were identified. An identical number of age-matched non-obese with BMI = 18.50 - 24.99 kg/m2 were taken as controls. Subject with symptoms of illness like fever, cough, abdominal pain, etc., and anxious, apprehensive, and uncooperative ones were excluded from the study. All subjects were explained about the procedures to be undertaken. The following measurements/tests were performed.
Weight (in kilograms) and height (in centimeters) were recorded on a beam balance. Waist circumference was measured as the smallest circumference between the ribs and the iliac crest to the nearest 0.1 cm, while the participant was standing with the abdomen relaxed, at the end of normal expiration. Hip circumference was recorded as the maximum circumference between the iliac crest and the pubic symphysis.
The subjects were demonstrated the maneuvers of the pulmonary function tests. Computerized spirometry was carried out by using Spirobank II MIR, Del Maggiolino 125, 00155 Roma, Italy, observing the guidelines laid down by the American Thoracic Society and European Respiratory Society [12]. Calibration of the spirometer was carried out daily using a 3-L calibration syringe as recommended by the American Thoracic Society. For the FVC maneuver, the subjects were asked to take a deep inspiration and breathe out as rapidly as and as long as possible into the mouth piece of the spirometer. Flow volume curve was plotted with the best of three acceptable maneuvers being taken as the final reading. The following pulmonary functions were recorded: FEV1, FVC, FEV1/FVC (ratio of FEV1 and FVC), PEFR, FEF25–75% or maximum mid-expiratory flow rate (MMEFR).
The data of the obese and control groups were compared using Student's t-test. The following comparisons were made:
• BMI, Waist circumference, Hip circumference, waist/hip ratio.
• Pulmonary function parameters of the obese and control groups.
Correlation co-efficient was calculated to determine the relationship between various measures of adiposity (BMI, waist circumference, hip circumference, and waist-to-hip ratio) and pulmonary function parameters.
The general characteristics and anthropometric variables of the obese and control groups has been depicted in Table 1. Weight, Waist circumference, and hip circumference was found to be significantly higher in obese groups compared to control group. The comparison of pulmonary function parameters of the obese and control groups has been shown in Table 2 and Figure 1.
Table 1: Characteristics of the ‘obese/overweight' and ‘normal weight' groups. View Table 1
Table 2: Comparision of dynamic lung volumes among obese/overweight and normal weight group. View Table 2
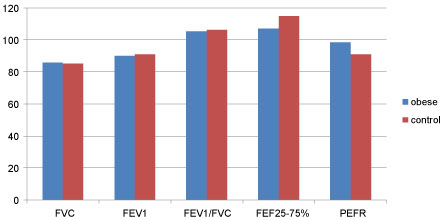 Figure 1: The comparison of pulmonary function parameters of the obese and control groups. View Figure 1
Figure 1: The comparison of pulmonary function parameters of the obese and control groups. View Figure 1
There was no significant difference in mean pulmonary function parameters between obese and non-obese control group. However, some of the obese subjects had mild restriction, whereas no obstructive impairment was detected in any subject of the obese and control group.
Table 3 presents the correlation matrix between various anthropometric variables and pulmonary function parameters. BMI has strong negative correlation with FEV1/FVC (P < 0.01), waist hip ratio was negatively correlated to FEV1/FVC but correlation is not significant. Waist circumference and hip circumference were strongly negatively correlated with FEV1/FVC (P < 0.01). Waist circumference has very strong positive correlation with FVC, whereas waist hip ratio has no significant correlation with any pulmonary function parameter.
Table 3: Correlation of anthropometric parameters with various pulmonary function parameters in adolescent of MSU (values are correlation coefficient r). View Table 3
Some studies have shown a significant reduction in spirometry parameters with obesity while others have not shown any effect [13-15]. Turan and co-workers have shown in a comparative study on obese and non-obese that although there was no statistically significant difference in FEV1, FVC, or FEV1/FVC, a significant reduction in peak expiratory flow rate (PEFR) and FEF25-75% was found in overweight and obese individuals [13]. Our study did not find any significant effect of obesity or overweight on dynamic lung volumes measured by spirometer, however the mean FVC was high in obese compared to non-obese control group which may be due to higher body surface area of the subjects in obese group.
In general, BMI is considered a measure of obesity and it cannot distinguish fat and lean body mass [16]. It is an index of nutritional status and its relationship with body composition is controversial. Waist circumference provides a simple measure of central fatness and it may have a direct effect on the chest wall properties. Waist Circumference mirrors body shape, while BMI provides an estimate of body mass and volume [17]. As previously shown, obesity is not a good parameter to evaluate body fat distribution when measured by BMI [18,19]. Abdominal obesity, measured by WC, was initially discussed as a risk factor for cardiovascular mortality and morbidity. Nowadays, other diseases are being studied to investigate the association with central obesity, including conditions related to pulmonary function [20]. One of the most discussed explanations in the literature is that abdominal fat may interfere in pulmonary mechanics, causing restrictions during breathing, potentially reducing respiratory volumes, such as FEV1 and FVC [7,18,21]. This mechanical effect is more evident if central obesity is considered instead of overall or peripheral fat [22]. The excess of fat in the abdomen and thoracic region may lead to decreases in the compliance and resistance of respiratory system, increasing energetic demands of breathing [21]. Another potential mechanism is that the increase in WC may have an effect on the diaphragm, limiting its movements [18]. There is no difference in the effect size on the respiratory system when different abdominal obesity indicators are used, such as WC and waist-to-hip ratio, and thoracic fat indicators [18], suggesting an interdependency of these measures with respect to pulmonary function parameters.
Our present study shows that BMI, waist circumference and hip circumference has strong negative correlation with FEV1/FVC (P < 0.01). A number of hypotheses have been proposed to explain the negative correlation between pulmonary function parameters and measures of visceral adiposity. One possible mechanism is a mechanical limitation of chest expansion during the FVC maneuver. Increased abdominal mass may impede the descent of the diaphragm and increase the thoracic pressure. Also, abdominal adiposity is likely to reduce ERV via compressing the lungs and diaphragm.
There are few limitations in our study. A bigger sample size would have given more concrete evidence. In our study we have only investigated the dynamic lung volumes since we did not have facilities to examine static lung volumes and ventilation-perfusion relationship in children.
In conclusions, our study did not show a significant effect of obesity/overweight on dynamic lung volumes among aldolescent of MSU. Significant negative correlation between BMI, waist circumference and hip circumference with FEV1/FVC suggest that obesity decreases FEV1/FVC ratio and obese are more prone to obstructive lung diseases.
None.