There are no reported series that specifically deal with repair of infected nonunion of the diaphysis of the forearm bones. We sought to determine whether a standardized treatment protocol we have utilized for 21 patients from 2014 to 2018 results in a high union rate, resolution of infection, and a good functional outcome.
The study cohort included fourteen male and seven female patients who presented to our hospital setting with an infected nonunion of the diaphysis of the radius or ulna. Every patient had a minimum of 2-year follow-up. The average patient age was 35.3 years (range 21-45). Thirteen patients had initially fractured both the radius and ulna. six patients had an isolated radius fractures, and two patients had fracture ulna alone. All patients underwent a protocol that combines aggressive surgical debridement associated with definitive fixation by intramedullary flexible nail and external fixation in the same session followed by after tricortical iliac crest bone grafting for segmental defects after 6 weeks. We sought to report our success rate of nonunion repair, number of re-interventions, complication rate, final ROM, and the ability to eradicate the infection using this treatment regimen.
At follow-up, all patients had fully united and the infection has been resolved with at least 50º of supination/pronation and 30-130º of flexion/extension arc. The average time to union was 131 days (range 100-183 days).
The results of this study indicate that, our standard protocol for treatment of infected nonunion of the shafts of the radius and ulna is reliable at obtaining fracture union with a good functional result, while also resolving the infection.
Forearm bones, Infection, Nonunion, External fixation and intramedullary nailing
With use of AO techniques of fracture fixation and with application of compression plates in the treatment of forearm fractures, expected union rate of forearm fractures has been greater than 95% [1,2]. Infection rates following ORIF of diaphyseal forearm fractures have ranged from 2 to 6% in the literatures but in the developing countries with lower economic resources infection rates are usually higher [1,3].
Although infected nonunion in the forearm are rare, they are considered as a complex problem due to the presence of bone necrosis, segmental bone defect, sinus tract formation, fracture instability, and scar adhesion of the soft tissues [4,6].
Only a small number of reports exist specifically dealing with infected nonunion of the diaphyseal radius and ulna [6-10]. Most of literatures looking at the forearm either deal solely with aseptic nonunion, or they lump all etiologies of forearm nonunion together [5,11-18]. Several other studies look at infected nonunion of long bones all together [19,20].
The main goals in our protocol of treatment of infected nonunion of diaphyseal forearm fractures are to adequately eradicate all infections of bone and soft tissue with excision of all sequestrate and implants and reaming of medulla, adequate stabilization with combined internal and external fixation, achieve bone union and attain an optimal functional outcome.
The purpose of the study was to review the results of this protocol utilized for 21 patients treated in our institution between 2014 to 2018.
After obtaining approval from our Institutional Review Board, a retrospective case series study was conducted to review all patients treated from infected nonunion of forearm bone fracture either radius alone, ulna alone or both bone forearm in our institute in the period between 2014 till 2018.
Inclusion criteria consisted of skeletally mature patients (≥18 years) with non-united, infected diaphyseal forearm fractures with a minimum of 2-year follow-up. All cases were treated by the first author by the same protocol of treatment as mentioned later.
Nonunion was defined as an unstable fracture with a lack of progressive healing following three consecutive radiographs, or the persistence of an obvious non0-united fracture a minimum of 4 months from injury. Patients were determined to have an infected nonunion based on clinical, laboratory, and radiographic criteria. Clinical indicators included: erythema or warmth around the incision sites, purulent discharge or palpable abscess, a draining sinus tract, localized pain, gross motion at the fracture site, and systemic signs of infection. Routine laboratory studies including white blood cell (WBC) count and erythrocyte sedimentation rate (ESR) were measured. All our patients had these clinical signs of infection with elevation of white blood cell count and ESR.
Radiographs were examined for persistent radiolucent lines or obvious gap at the fracture site, osteolysis, implant loosening or failure, and periosteal reaction.
There was a total of 21 consecutive patients treated by a single surgeon in this study. Included are fourteen males and seven females with a mean patient age of 35.29 ± 7.5 (range 21-45 years). The dominant arm was involved in 11 of the 21 patients (52%). The injury mechanisms included: six falls, nine motor vehicle collisions (MVC) and six crush injuries. Twelve of the injuries were open fractures. All had previously undergone open reduction and internal fixation. Thirteen patients had initially fractured both the radius and ulna (62%), six patients had an isolated radius fractures (29%), and two patients fractured the ulna alone (8%). All patients had documented infections at the nonunion site.
Eight patients were active smokers. Four patients had multiple comorbidities, including two with insulin-dependent diabetes mellitus. Two patients had been treated for psychiatric disorders. Fourteen patients had initially been treated at an outside institution.
The mean time from injury to presentation to us was 9 ± 2.90 months (range 6-15 months).
After the patients are identified as likely having an infected nonunion, they were taken-off of antibiotics for 10-14 days if they are actively being treated. After this period of stopping antibiotic, patients were taken to the operating theatre to start first stage of treatment protocol.
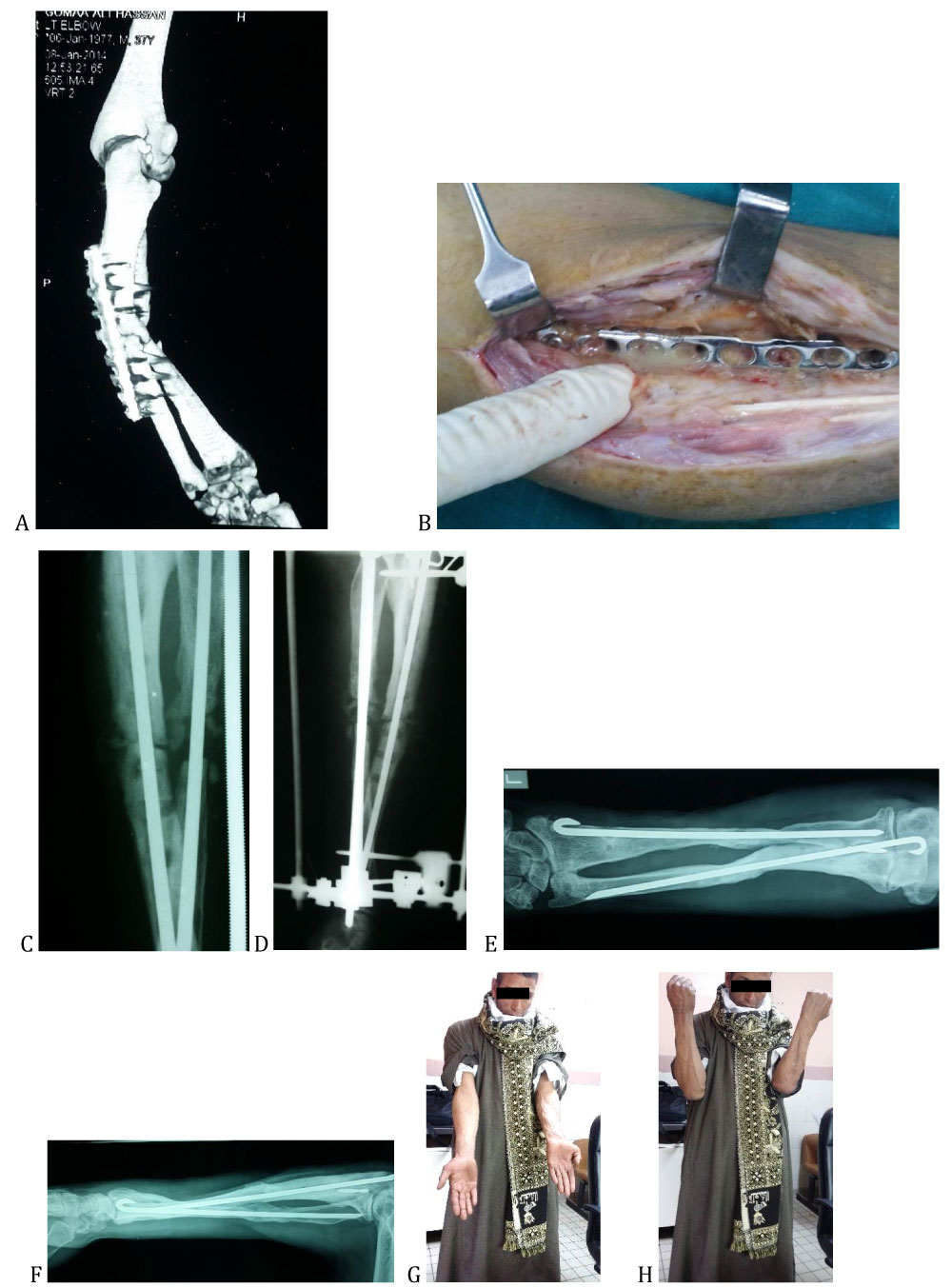 Figure 1: a) Preoperative CT of infected non-united both bone forearm b) Intraoperative photo of infected plate c) Postoperative x-ray after fixation with rush pin and ilizarov d) X-ray after bone grafting e) AP X-ray view after full union f) Lat. X-ray view after full union G) Photo of patient with full elbow extension H) Photo of the patient with full elbow flexion.
View Figure 1
Figure 1: a) Preoperative CT of infected non-united both bone forearm b) Intraoperative photo of infected plate c) Postoperative x-ray after fixation with rush pin and ilizarov d) X-ray after bone grafting e) AP X-ray view after full union f) Lat. X-ray view after full union G) Photo of patient with full elbow extension H) Photo of the patient with full elbow flexion.
View Figure 1
1st stage: depend mainly on good debridement by debridement of soft tissue layer by layer and removal of all hardware from radius and ulna then removal of a biofilm.
Previous surgical incisions were utilized when possible. Avascular Scars were resected along with any established sinus tracts.
Great care is taken to sharply debride any inflammatory or fibrous tissue in the wound. Deep cultures are obtained, and bone specimens sent to pathology for analysis. Any necrotic bone is debrided until punctate bleeding of the bone ends was visualized (Paprika sign). A 2.5-mm drill is utilized to drill the intramedullary canal in both the proximal and distal segments. The wound is copiously irrigated.
After good debridement we did fixation by intramedullary rush pin of radius and ulna with acute shortening and compression.
This leads to good coaptation of both bones or one bone and remaining of a defect of the other bone; until this stage there is good Varus valgus stability but no rotational and axial stability.
To add more stability after skin and soft tissue closure, we did additional stability by external fixation by ilizarov external fixator formed of one ring at wrist and ½ ring at elbow joint with distal radioulnar fixation by ilizarov wire.
2nd stage: after 6 weeks from the 1st stage while the patient on antibiotic treatment, laboratory investigations with CBC, ESR and CRP were done. All patients were started with parenteral broad-spectrum antibiotic until appearance of culture and sensitivity then continued with specific antibiotic according to culture and sensitivity.
When laboratory investigations were good; we did bone grafting by iliac crest bone graft for the small defect and segment transfer if defect more than 3 cm.
After that we did follow up of the patient with laboratory and radiological investigation until radiological union has been obtained then removal of ilizarov was done.
After that patient did rehabilitation with physiotherapist to improve range of motion of elbow, wrist and forearm and increase muscle strength and hand grip strength.
A total of 21 consecutive patients have been treated by a single surgeon for infected nonunion of diaphyseal forearm fractures utilizing this protocol. The average follow-up was 2.5 years (range 2-4 years). All patients eventually achieved infection-free union and had no evidence of infection after initial fixation in this protocol.
The mean time to union was 131.19 ± 22.34 days (range 100-183 days) (Table 1).
Table 1: Preoperative and postoperative results. View Table 1
Intra-operative and radiographic findings in all patients demonstrated atrophic nonunion. Cortical bone destruction with a moth-eaten appearance was observed in all cases. Dense fibrous tissue was always present at the nonunion site with surrounding inflammatory tissue.
Tricortical iliac crest graft was used in all 19 cases in which this was found. The average gap measured 1.5 cm, with a range of 1-3 cm while 2 cases undergo segment transfer as gap measured 4 cm in both.
All cases were noted to have inadequate fracture fixation at the time of revision, and consequently hardware was removed universally. The plates used at index procedures were often tubular or pelvic reconstruction plates, or the implant chosen was simply deemed to be too short to provide adequate stability. Often there were less than six cortices of fixation on either side of the plate in the face of a short implant. Gap was universally noted at the fracture site, indicating a lack of adequate compression or possibly bone resorption.
Deep wound cultures are positive in all cases. Most of them are polymicrobial infection, most common organism is staphylococcus aureus. The surgical pathology demonstrated necrotic bone and inflammatory fibrous soft tissue.
As regard of postoperative range of motion at the end of treatment protocol is as follow:
The mean pre-operative elbow flexion was 95 ± 13º (range 90-110º) while mean post-operative elbow flexion range was 118.1 ± 8.14 (range 120-130º) with highly significant P- Value (P = 0.0001). the mean pre-operative elbow extension was 18.10 ± 8.73º (range 10-30º) while post-operative elbow extension range was 6.67 ± 4.83º (range 0-10º) with highly significant P- Value (P = 0.0001). average Supination/0/Pronation range preoperatively was 32/0/0° changed to postoperative average range 82/0/15º with highly significant P- Value (P = 0.0001).
Thirteen patients had no complications, seven patients suffered from mild to moderate pin tract infection and the two heavy smoker patients had delayed union. All patients returned to their work and all had general satisfaction.
Most manuscripts act on treatment of infected nonunion deal with lower extremity infected nonunion especially tibial nonunion [19-21]. Few manuscripts deal with infected non-union of forearm fractures, most reports were either individual case reports [6-8,10], in association with forearm nonunion that were not infected [5,11,18], or in conjunction with infected nonunion of other long bones [19-21].
Only one report has dealt specifically with infected nonunion of the forearm [9]. In this case series of four patients, the authors discuss their results with transfer of a vascularized fibular graft to create a one-bone forearm. They fixed the graft to the ulna proximally and the radius distally with internal fixation. In three of the cases it was necessary to use adjunctive external fixation, and one patient required additional supplemental bone grafting [9].
In most reports, the method of treating infected forearm nonunion is not precisely delineated, and the number of cases is so small that it is difficult to draw conclusions about the efficacies of the treatment modalities, which have also varied widely [6-10,12,15,22].
Ring, et al. have reported on a large series of nonunion of diaphyseal forearm fractures. Their retrospective study consisted of 35 patients, eleven of them had deep infections. The main emphasis of the paper was dealing with segmental defects with bridge-plating and adjuvant autologous bone graft. All patients were treated with cancellous autograft, and no patient required a vascularized bone graft or even structural cortical autograft. They did not provide a detailed description of their treatment protocol for the infected patient subset, and never commented on whether the infection was completely eradicated following treatment [7].
In a similar study of forearm nonunion, the authors also had a mixed cohort of septic and aseptic nonunion but treated them with compression plating and structural autologous bone graft. They demonstrated an excellent union rate (30/31 patients), but once again gave no specific mention to the treatment of the infected patient subset [18].
The open technique of bone grafting for patients with large segmental defects of bone secondary to chronic osteomyelitis has been described previously. The authors of these studies emphasized that delayed secondary closure of the skin was essential. They also stated that stable skeletal fixation was an integral component of the method. These authors simply used autologous bone graft and avoided the high morbidity of vascularized bone transfer as well [17,22].
In our study, we depend on good debridement and optimal skeletal fixation for treatment of infected nonunion of forearm fractures, no manuscript discussed before the use of combined fixation method for the treatment of infected nonunion of forearm fractures, With the use of this protocol for treatment of infected nonunion of forearm fractures, we obtained infection free union for all patients with functional range of motion.
Radical debridement was considered the key for treatment in our protocol for treatment of infected nonunion forearm followed by adequate stability of fracture through intramedullary flexible nail combined with external fixation to give good environment for fracture healing.
From our results, full union of all patients was taken, and functional range of motion of elbow and forearm was obtained. Good elbow flexion, extension and forearm supination were obtained with some limitation of forearm pronation.
From our results only two cases had delayed union and from their medical history; both are heavy smoker.
combined intramedullary and external fixation after good debridement is an efficient method for treatment of infected nonunion of forearm fracture.
None of the above authors claim any conflicts of interest or received any funding for this investigation.