Open fractures present a significant challenge to the patient and his family and the managing surgeons. Open fracture often results from high energy injuries such as road traffic crashes, gunshot injuries, falls from heights and high-speed sports. Open fractures are associated with life-threatening and limb threatening injuries and are often associated with complications such as infection, malunion, and non-union. Controversies abound in the pattern of presentation, management, and outcome of open fractures. This study aims to evaluate the pattern of presentation, treatment, and outcome of open fractures treated in a regional trauma centre in Nigeria.
Prospectively collected data of all cases of open fractures treated at the Regional trauma centre from 1st January 2007 to 31st December 2012 was evaluated to determine the pattern of presentation, treatment given and outcome of the cases. Cases of open fractures referred to other centres or those that died shortly on arrival before treatment was commenced were excluded. Descriptive statistics of the obtained result was generated and presented in tables and scientific figures while inferences were drawn as considered appropriate.
The total number of the cases were open fractures seen at the centre during the period under evaluation was 1758 which constituted (39.10%) of all the fractures seen at the centre during the period. Persons between the ages of (21-30) years were the highest affected group with open fractures at the centre (706, 40.2%) while children and persons older than 60 years contributed 67 (3.8%) and 45 (2.6%) respectively. The male to female ratio was 4.3:1. A significant proportion of the cases resulted from road traffic crashes (1262, 71.8%) while gunshot injuries contributed 313 (17.8%) of the cases. Type I and II open fracture constituted (587, 33.4%), and (500, 28.4%) respectively while types III open fractures represented 671 (38.2%) of the cases and a significant proportion of the cases involved the tibia (869, 41.4%). Most of the fractures were treated by external fixation (731, 41.6%) but 38 (2.2%) cases had amputation. The most frequent complication was infection in 126 of the cases (7.2%). The length of hospitalization, duration to fracture union and occurrence of infection were all significantly related to the severity of the open fracture.
Open fractures are relatively common at the centre particularly amongst males in the age group of (21-30) years and often result from high energy injuries such as road traffic crashes and gunshot injuries. Adherence to established principles of management produces acceptable outcome even in the face of limited resources. Preventive approach for open fractures will require increased advocacy on road safety and stricter control of light weapons and criminality in the region.
Fractures, Open fractures, Presentation, Treatment, Outcome, Nigeria
Open fracture often results from high energy trauma and presents a significant challenge to, the patient and family, the managing orthopaedic surgeon and healthcare institution [1]. Aside from the fracture, the associated soft tissue injury exposes the fracture and its haematoma to the exterior, thus increasing the risk of microbial contamination and infections [2]. Such infections alter the natural history of fractures as they are often associated with adverse outcomes such as delayed fracture union, malunion, non-union and in some cases amputation [1-3].
The pattern of presentation of open fractures, therefore, varies from causative factor, age, and gender of patients, the bone involved and geographical location of the patient. Whereas most open fractures result from high energy injuries such as road traffic crashes (RTC), gunshot injuries (GSI), falls from heights, stab wound and high-speed sports [4-6] especially in the young active males. Some open fractures also result from low energy injuries such as domestic falls particularly in children and elderly patients [7].
Open fractures are classified based on the severity of soft tissue injury, fracture configuration and the level of energy producing the fracture [2]. Classification of open fractures helps to define the severity of the injury, to plan management and to prognosticate the outcome of the injury [2]. Various classifications methods have been produced to categorize open fractures including those of Gustilo and Anderson [2], Tcherne [8], and AO/OTA [9]. The various classifications have their shortcomings, but the popular one commonly used to be that of Gustilo and Anderson classification which categorised open fractures into four specific groups, types 1, II, IIIA, IIIB, IIIC [2,10]. The Gustilo-Anderson classification has the shortcoming of having high inter-observer variability in up to 50% to 60% of cases [11] and since the size of injury on the skin surface may not reflect the extent of deeper soft tissue injury, the actual grading of open fracture using Gustilo and Anderson classification can only be done in the operating room [12]. Gustilo-Anderson classification is easily reproducible and applicable as such has remained a prevalent classification method despite having been produced more than four decades ago. The limitations of the original classification of open fractures by Gustilo-Anderson led to its subsequent revision in an attempt to improve its validity, reliability and predictability [10].
Aside from diverse presentation patterns, the management of open fractures also presents some challenge to both the patient and the managing team. Open fractures are considered muskulo-skeletal emergencies and should be managed as a surgical priority as much as possible. The management of open fractures follows the essential principles of trauma care, which is prioritised to saving the life, saving the limb, restoring function and then aesthesis of the affected part [12].
The initial treatment of open fractures follows the Advanced Trauma Life Support (ATLS) protocol [13] to save the life, to prevent infections with early antibiotic and anti-tetanus prophylaxis, early wound irrigation and debridement of the associated soft tissue wound, and early skeletal stabilisation of fractures 14. Subsequent care requires the early cover of the soft tissue wound by methods ranging from simple wound suturing to complex flap cover, and definitive skeletal stabilisation [14]. Skeletal stabilisation includes non-operative methods such as casting with plaster of Paris (POP) and use of traction forces applied either as skin traction or skeletal traction for lower grade open fractures, e.g. Types I and II particularly in children [15]. Operative methods are reserved for more severe open fractures using external fixation [16] internal fixation with implants such as intramedullary nails, plate and screws, K-wires and others [17] for Types I, II, and some type III A open fractures especially if the associated soft tissue wound is not very contaminated, there was no associated bone loss and there is early cover of the soft tissue wound [1]. Some extreme cases of open fractures are treated by amputation either as a primary option in non-salvageable mangled limbs or as a secondary amputation as a salvage option when the other methods of treatment fail [18,19].
Controversies abound in the management of open fractures. Such controversies include the timing of wound debridement and wound closure [20], and the appropriate fluid for wound irrigation [21,22]. Recently, a Level I evidence study found that there is no significant difference between antibiotic and liquid castile soap solutions as irrigation fluids in wound infection or bone-healing rates in the management of open fractures. This same study also found a statistically significant relationship between wound-healing problems and antibiotic (bacitracin) irrigation [23]. Generally, there is a lack of evidence-based recommendations in the literature to guide surgeons on the appropriate additives for irrigations for open fractures. Other areas of controversy include, the choice of antibiotic treatment [24] the timing of soft tissue cover [1,25,26] , the choice of definitive fixation of the fracture especially on the place of internal fixation in open fractures 18 and the decision to amputate or salvage the limb in severe open fractures [27] remain topics of ongoing debate in the management of open fractures.
Open fractures are associated with higher complications such as infections, delayed fracture union, malunion and non-union as compared to closed fractures [1]. The outcome of open fracture is influenced by the promptness and quality of treatment given. Such treatment is influenced by the availability of resources, the experience of the managing surgeon, existing local protocols and socio-economic condition of the patients [1].
This study aims to evaluate the cases of open fractures treated in a regional trauma centre in Nigeria looking at the pattern of presentation, treatment given and outcome of such fractures with the view to make recommendations to address problems of open fractures in the region.
Information of the patients presenting with open fractures between January 2007 and December 2012 in a dedicated regional trauma centre in Nigeria jointly run with an International Non-for profit, a non-governmental organisation was collected prospectively and analysed. Since the treatment of all patients at the centre was free of charge, the cost of care did not influence the choice treatment method, choice of implant and type of surgery for fracture fixation. However, the decision for the choice of treatment was influenced by the severity of the injury, available resources including implants and expertise at the facility at any particular time.
Open fractures in the centre where this study was undertaken were treated as emergencies with immediate resuscitation using the ATLS Protocol, administration of intravenous opioid analgesic either with morphine or fentanyl, commencement of intravenous antibiotics with cephazolin for types I and II open fractures and ceftriaxone, gentamycin, and metronidazole for types III open fractures. Tetanus prophylaxis was also commenced for all open fractures with human tetanus immunoglobulin and the associated soft tissue wound, and whole injured limb thoroughly washed and irrigated with dilute chlorhexidine in pre-sterilized water of visible debris and sand in the emergency room before a formal wound debridement in the operating room. The and fracture was initially splinted temporarily with casts, or traction especially skeletal traction pending definitive skeletal stabilization of the fracture in the operating room depending on the type and configuration of the fractures. Following the fracture stabilization, the soft tissue wound was managed till healing by delayed primary healing, secondary wound healing, split skin grafting (SSG), of flap cover as considered appropriate and within the available capacity. Most of the patients were hospitalised until the fracture had been stabilised and the associated soft tissue wound had been controlled to a point where further wound care can be done on an out-patient basis.
Information relating to age, gender, cause of injury, location and type of open fracture, level of contamination, treatment given and outcome including postoperative complications, lengths of hospitalisation and duration of fracture union evidenced which were analysed. Cases that were referred out to other centres for advanced care which was not available at the centre and patients that died before definitive fracture fixation were excluded from outcome analysis.
Obtained data were analyzed using statistical package for Windows version 20 (IBM SPSS Statistics for Windows, Version 20.0. IBM Corp. Amok, NY). Descriptive statistics were generated and presented as considered appropriate and inferential statistics when necessary. Categorical variables are presented as proportions and percentages and numerical variables presented as means and standard deviation (SD) and median with interquartile ranges (IQR) as considered appropriate. Chi-Square (χ2) was used to test for observed differences among categorical variables while the Student's t-test and Analysis of Variance (ANOVA) were used to compare means for numerical variables. P-values less than 0.05 are accepted as statistically significant.
The total fractures seen at the centre during the period under evaluation was 4498, of which the 1758 (39.10%) of the cases were open fractures.
The age distribution of open fractures showed that persons between the ages of (21-30) years were the highest affected group with open fractures at the centre (706, 40.2%) followed by the age group (31-40) years (480, 27.3%), while children below 10 years and persons older than 60 years contributed 67 (3.8%) and 45 (2.6%) respectively, P < 0.0001. The mean age distribution ± SD was 31.7 ± 12.3 years (Table 1, Figure 1, Figure 2 and Figure 3).
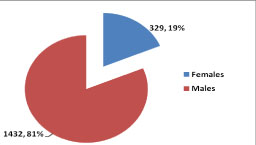 Figure 1: Gender distribution of open fractures.
Figure 1: Gender distribution of open fractures.
χ2 = 688.282; P < 0.00001; Male:Female = 4.3:1.
Classification of Associated soft tissue Wounds using Altemeier's Contamination Classification [28].
View Figure 1
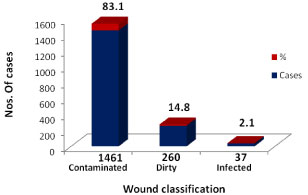 Figure 2: Classification of Associated soft tissue Wounds.
Figure 2: Classification of Associated soft tissue Wounds.
χ2 = 2002.222; P < 0.00001.
View Figure 2
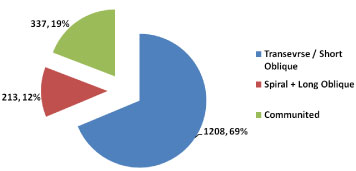 Figure 3: Showing geometry of the fractures.
Figure 3: Showing geometry of the fractures.
χ2 = 1003.437; P < 0.00001.
View Figure 3
Table 1: Age distribution of fractures. View Table 1
A significant proportion of the injuries resulted from road traffic crashes (RTC) (1262, 71.8%) followed distantly by gunshot injuries (GSI) (313, 17.8%). Assaults and falls contributed 88 (5.0%) and 26 (1.5%) respectively, P < 0.00001 Table 2.
Table 2: Cause of Injury. View Table 2
The commonest type of open fracture seen at the centre was Type II (587, 33.4%), followed closely by type I open fractures (500, 28.4%) and type IIIA open fractures (411, 23.4%). Type III C open fractures was recorded in 78 cases (4.4%), P < 0.00001 Table 3.
Table 3: Type of Open fracture. View Table 3
Most of the open fractures in this series involved the tibia and fibula (869, 49.4%) followed distantly by the femur (249, 14.2%) then the radius and ulna (179, 10.1%), while the patella was the bone least involved with open fracture (6, 0.3%), P < 0.00001. Generally, the left side of the body was the most commonly involved of all the bones of the body except for the ankle and small bones of the hand and foot. These observed differences were not statistically significant, P > 0.05 Table 4.
Table 4: Location and lateralization of fractures. View Table 4
Most of the open fractures were treat xed by external fixation (EXFIX) (731, 41.6%), followed by open reduction and internal fixation (ORIF) with implants including intramedullary (IM) nailing (104, 5.9%), plates and screws (109, 6.2%). Non-operative methods as Casting and traction was used as a definitive treatment in 413 (23.5%) and 24 (1.4%) of the cases respectively Table 5.
Table 5: Definitive treatment given. View Table 5
Infection was the commonest complication recorded among the cases (124, 7.1%), non-union and malunion were recorded in 47 (2.7%) and 31 (1.8%) of the cases respectively, Table 6.
Table 6: Complications recorded. View Table 6
Eight hundred and twenty-one (47%) of the 1087 patients with type I and type II open fractures were hospitalised for less than 14 days as compared 313 (17.8%) of the 671 cases with types III open fractures. The mean length of hospitalisation for persons with Type I open fractures was 11 ± 21 days while patients with Type III B open fractures had the longest length of hospitalisation Mean LOS (34 ± 29.3 days). t-test = 9.96 (95% CI = 11.4 - 17.0), P < 0.0001.
Evaluation of the relationship between the types of open fracture and time to radiological union, showed that there was significant difference in the fracture union rates between the different types of open fractures over the same period (P < 0.05). However, whereas within each group of particular type of open fracture there was no significant difference in the fracture union rates at six weeks, 12 weeks, 18 weeks and 24 weeks except for types I and IIIB open fractures P = 0.028 and 0.0007 respectively. There was no statistically significant difference in the fracture union rates between cases of Type I & II open fractures (418/1024, 40.8%) compared to of types III A, B, and C open fractures (164/608, 27.0%) at 12 weeks post definitive treatment (χ2 = 2.882, P = 0.09). As at 18 weeks, 24.9% (255/1024) of types I and II open fracture had not united as compared to 26.2% (158/604) of types III A, B, and C fractures combined, P > 0.05.
When the recorded complications were disaggregated for the various categories of open fractures, it was observed that type III B had the highest infection rate (28/182, 15.4%) followed by type III C (11/78, 14.1 whereas, open type I had the least infection rate (16/500, 3.2%), χ2 = 22, P = 0.0002. Similarly, type III B open fractures had the highest malunion rate (5/182, 2.7%) as against type I open fractures (6/500, 1.2%), whilst the highest non-union rates were amongst the type III C open fracture (6/78, 7.7%) as compared to type I open fractures (5/500, 1.0%). These differences were, however, not statistically significant P > 0.05. One patient with the type II, and type III-A open fracture, and four patients each with type III B and Type IIIC had secondary amputations after a failed primary treatment.
The result of this study showed that open fractures constituted approximately 40% (1758) of the fractures seen at the centre during the period under evaluation. This proportion may be considered relatively higher than those reported in other series from Europe [29,30] and North America [1,31] but not much different from those reported from other centres in the region [32]. The reasons for this pattern may be related to the high number of road traffic crashes in the region which is amongst the highest in the world [33]. Other high energy injuries such as gunshot injuries which was relatively higher in the region from increased militancy, civil rife and agitations, and criminality in the region [34], and falls from heights such as trees [35] which is commoner in school-age children who are often out of school for reasons of higher levels of poverty and child labour in the region [36]. The comparatively higher propensity of open fractures in persons aged between 20 years and 30 years (Table 1) in the male gender (M: F; 4.5:1) as compared to the distribution of all fractures even from the same centre with (M:F; 2:1) [37] is indicative of the higher risk exposure of young active males who are often the bread-winners of the family. This peak age of incidence observed in this study was lower than that reported in Europe [38]. The observed pattern may not be unconnected to the fewer patients older than 60 years with open and the lower Life-expectancy in Nigeria which was reported as 54.5 years by the World Health Organisation (WHO) in 2018 [39]. This life–expectancy is much lower to those reported from the developed countries [39].
A higher proportion of the injuries were of Type II (587, 33.4%) and types III open fractures (571, 38.2%) confirming the fact that most of the fractures resulted from high energy injuries (Table 3). The numbers of Type III C open fractures (78, 4.4%) were indicative of the magnitude of life and limb-threatening injuries recorded during the period. The observed pattern from this series while similar to reports from other studies in the region [40,41], as well as other developing nations [42] differs considerably from those reported from the developed countries where only 22% of the open fractures resulted from high energy injuries (RTC and Falls from heights) [38]. Most of the fractures involved the tibia/Fibula (869, 49.4%) which constituted almost half of the open fractures (χ2 = 1054.619, P < 0.00001). This pattern may be due to the subcutaneous location of the tibia which is devoid of soft tissue cover especially in its anteromedial surface [43]. This pattern is in keeping with an earlier report from other studies [44].
A significant proportion of the fractures were treated by external fixation (731, 41.6%) which remains the standard of care for severe open fractures [17]. Almost a third of the fractures (531, 29.1%) were treated by internal fixation particularly in Type 1 open fractures which is in keeping with the current recommendation of the place of internal fixation in the treatment of open fractures especially in minimally contaminated fractures and fractures without significant bone loss [45]. Griffin and colleagues had suggested that definitive stabilisation of the skeletal injury even in cases of types III open fractures is best achieved with an IM nail, as it provides the greatest mechanical stability of available surgical methods [46]. Even the more recent prospective randomised study by OʼToole and colleagues on the choice of fixation method in severe open fracture appears also recommend IM nailing for severe open fractures [47]. The choice of IM nailing in types III open fractures may be as a result of extra caution for higher risks of complications in the centre since the wounds are often grossly contaminated by the time the patients arrive the trauma centre. The choice of amputation in 38 patients (2.2%) of patients including the ten patients that had secondary amputation for failed initial definitive treatment is indicative that appropriate patients' selection using validated criteria for limb salvage will help as to avoid unnecessary surgical interventions which may fail in due course. However, the proportion of Type III C open fractures that had successful limb salvage indicates that limb salvage is possible and perhaps preferable in appropriately selected cases. Similar results have been reported in other studies in developed countries [48] but contrary to reports from some other centres in developing countries where most Type IIIC open fractures are treated by amputation (28% in Northwest Nigeria, 57% in Rwanda respectively) for reasons of lack of capacity and capability required for advanced limb salvage [40,42]. In addition, the number of patients that opted for limb salvage as against amputation in this study contrary to the 3.3% (125/3777) reported by Tampe and colleagues in Sweden [49] confirms the reluctance to accept amputation as treatment option in the region for socio-cultural reasons, non-availability of functional prosthesis in the region and none existence of social welfare for the physically challenged person in the country as compared to what exist in the developed nations [27].
Evaluation of the duration of hospitalization (LOS) revealed that about 47% (821/1758) of Type I and Type II open fractures were hospitalized for less than 14 days compared to 17.8% (313/1758) of cases with Types III open fractures. The observed difference was statistically significant when subjected to further statistical tests on the mean LOS between the various types of open fracture (F = 182.43532, P < 0.00001) and the mean LOS between Types 1and II fractures, and Types III fractures, (t-test = 9.96 (95% CI = 11.4 – 17.0), P < 0.0001) (Table 7). The reasons for these differences are not farfetched; the extent of associated soft tissue wounds in types I and II fractures did not require complex wound management and did not require prolonged hospitalization as compared to types III open fractures which required complex and multiple soft tissue reconstructions which often necessitated prolonged hospitalization [1]. Besides, types I and II open fractures were amongst the group that had earlier soft tissue wound cover and healing, and a higher likelihood of internal fixation for definitive fracture stabilization which allowed for earlier mobilization and discharge of the patient from the hospital [17].
Table 7: The relationship between grade of open fracture and length of hospitalization. View Table 7
Similar pattern was also observed in the time to radiological union of the fractures (Table 8). There was a clear significant difference in the fracture union rates between the various types of open fractures, e.g. the union rates progressively reduced with increasing severity of open fracture at various intervals after treatment P > 0.05. However, there was a statistically significant difference in the fracture union rates between cases of Types I and II open fractures (40.8% {418/1024}) as compared to Types III A, B, and C open fractures (27.0% {164/608}) at 12 weeks post definitive treatment (χ2 = 32.148, P < 0.0001). Also, the observed difference in union rates was not statistically significant between the Type I and II open fracture, and type III fractures beyond 18 weeks (24.9% {255/1024}) as compared to (26.2% {158/604}) respectively P > 0.05).
Table 8: The relationship between grade of open fracture and time to radiological union. View Table 8
The observed infection rate of 7.1% (124/1758) for all open fractures can be considered a comparatively good outcome for open fractures considering that open fractures are prone to infection which is one of the most dreaded complications which alters the natural history of fractures. For a hospital in the developing country, this may be considered a comparatively good outcome bearing in mind the much higher infection rates (74% {142/192) (39% {35/91}) reported from Kigali, Rwanda and Ile-Ife, Nigeria respectively in the same region [41,42]. When the observed infection rates were disaggregated for the different categories of fractures, it demonstrated that the risk of infection in different types open fractures was significantly associated with the severity of the open fracture, P = 0.0002, (Table 9). Various authors have reported different infection rates for open fractures ranging from (0 to 2) % for Type I fractures, (2 to 10) % for Type II fractures, and (10 to 50) % for Type III fractures [2,12,50]. Patzaki and Wilkins had shown that the rates of clinical infection increased to 1.4% (7/497) for Type I fractures, 3.6% (25/695) for Type II fractures, and to 22.7% (45/198) for Types III fractures [3]. Again, this observed pattern in the index study may be related to the level of energy producing the fracture with more devitalisation of tissues, higher grade open fractures with a higher degree of wound contamination and a higher risk of infection [1,2]. Also, since patients with a higher grade of injuries have prolonged hospital stay, they are more prone to hospital-acquired infections which in some cases can be resistant to conventional antibiotics [51,52]. Also, the observed malunion and non-union rates in the treated fractures were higher in the more severe type III open fractures as compared to types I and II fractures. These complications are often related to the associated infections, challenges of fracture management aside from the severity of the primary injury [1,53].
Table 9: Grades of open fracture and outcome variables. View Table 9
Open fractures are relatively common and constituted about 40% of fractures treated at the centre during the period under evaluation. Open fractures are predominantly a disease of the active young males within the age group of (21-30) years and often results from high energy injuries particularly road traffic crashes and gunshot wounds. Most of the types III open fractures in the centre were treated by external fixation while internal fixation and non-operative methods were used for Types I and II open fractures with a comparatively favourable outcome. Infection remained a significant complication of open fractures. Infection, prolonged hospitalization, and delayed fracture union were directly related to the severity of the open fracture.
Since open fractures present a significant challenge to the patient and the managing surgeon, every attempt should be made to reduce the incidence of open fractures. Such efforts will require improving road safety standards in the region as well as addressing issues of militancy, civil and communal unrest, reducing the number of out-of-school children, and stricter firearms control in the region which are the common aetiological factors.
The study was approved by the Research and Ethical Review Committee of International Centre for Advanced Medical Care and Development (ICAMCAD) who are the developers of the registry.
Not applicable.
The data that support the findings of this study are available from the authority of International Centre for Advanced Medical Care and Development (ICAMCAD) but restrictions apply to the availability of these data, which were used under license for the current study, and so are not publicly available. Data are however available from the authors upon reasonable request and with permission of the authority of the International Centre for Advanced Medical Care and Development.
We acknowledge the Board and Management of the International Centre for Advanced Medical Care and Development for allowing access to the data from their trauma registry.
Authors have declared that no competing interests exist.