Glioma (astrocytoma) is one of the most common primary intra-axial CNS neoplasm and glioblastoma (GBM) is the most aggressive form of astrocytoma (grade IV). According to Central Brain Tumor Registry of the United States (CBTRUS), GBM is the most common primary malignant primary CNS neoplasm with median survival of only 15 months [1]. With emergence of new treatment options on the horizon, imaging precision is important to treatment planning. In this mini-review, we aim to demonstrate utility of efficacy of pre-neurosurgical planning for GBM using functional MRI (fMRI) and 3D tractography.
Task-based Functional MRI (fMRI) detects activation of neurons in the eloquent brain regions using Blood oxygen level dependent (BOLD) sequence. Neuronal depolarization leads to transient change in blood flow in region of activation which results in differential oxygenated-to-deoxygenated hemoglobin concentration. This differential results in positive signal on MRI BOLD sequence. The signal serves as surrogate marker of neuronal activation and when overlaid on structural imaging (T1 pre or post-contrast series) can aid in mapping of the eloquent cortex. Task-fMRI is commonly used for presurgical planning in academic centers and has become effectively the new standard of care [2,3]. Task-fMRI can identify motor, visual and language networks preoperatively and studies have shown this has allowed for reduced operative time, craniotomy size, and increase extent of surgical resection [4,5]. Also fMRI can predict hemispheric dominance and can help evaluate operative risks and perioperative neurologic deficits [6-8]. Diffusion tensor imaging (DTI) is a gradient echo planar based MRI sequence similar to conventional diffusion weighted imaging (DWI). DTI detects Brownian motion of water molecules restricted by cell membrane to identify white matter tracts. As such, DTI can help evaluate white matter tracts including orientation and integrity, which can play critical role in preoperative surgical planning especially in setting of GBM which tends to spread along white matter tracts. Advanced post-processing techniques can provide 3-dimensional (3D) evaluation of white matter tracts, commonly referred to as 3D tractography.
Combined fMRI and 3D-tractography can provide detailed assessment of spatial extent of tumor-core and provide information of about the integrity of white matter tracts adjacent to the tumor. For example, Figure 1, a 49-year-old female with multifocal gliomatosis underwent functional MRI of the brain to evaluate eloquent cortex and 3D tractography for presurgical planning. Multiplanar multisequence MRI of the brain was performed without and with contrast including T1 MPGR pre- and post-contrast, T2 weighted imaging, Fluid attenuation inversion recovery (FLAIR), Diffusion tensor imaging (DTI), perfusion weighted images PWI (including DSC and DCE) were acquired. Additionally multi voxel MR spectroscopy was performed. Also, functional MRI of the brain was performed and the following paradigms were assessed: Rhyming, silent word generation, sentence completion, right finger tap, bilateral foot movement, and memory. The 3-D post-processing was performed on Prism Clinical Imaging software (FDA approved) utilizing an independent workstation under physician guidance. The functional MRI paradigms delivered during the examination and 3-D processing was performed per the referring clinician's request.
Structural MRI demonstrates an enhancing 3.1 × 1.6 cm mass in the left insular cortex with surrounding FLAIR hyperintensities extending into the subjacent temporal lobe. Functional MRI demonstrated left lateralization of the language network with Broca's (not shown) in the IFG and Wernicke's (arrow) in the posterior left superior temporal sulcus. 3D Tractography demonstrates intact associated white matter fiber tracts (arcuate fasciculus and superior longitudinal fasciculus).
Functional MRI and 3D tractography can successfully evaluate the eloquent cortex and white matter tracts which can help preoperative planning in patients with brain tumors. The added value of fMRI and 3D tractography, as studies have shown, includes reduced operative time, craniotomy size, and increase extent of surgical resection. Presurgical DTI and fMRI should be especially considered in patients who have tumor involving or adjacent to expected eloquent cortex as it can potential improve immediate and long term postsurgical outcomes.
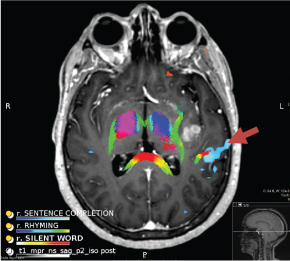
Figure 1: Functional MRI and 3D Tractography.